

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Treatment options using implants can be mainly divided into fixed types and removable types in edentulous patients.1 The appropriate type should be determined by considering the radiographic findings, the intra-oral examination, the diagnostic cast, and the patient's demand in the diagnostic stage, and by assessing the amount of residual ridge resorption and the biomechanical condition.2 The removable type is classified into implant-supported overdentures that achieve support from multiple implants, and implant-tissue-supported overdentures that achieve support from both tissues and implants by having distal extension areas.3
The attachments used for implant overdentures are mainly divided into the bar type and the solitary type, and into the resilient type and the rigid type, depending on the movement allowance. The attachment selection is affected by the implant number, distribution and alignment, bone quality, arch shape, retention, and denture design.4
A locator can be used in implant overdentures with a bar for retention improvement. Three methods-the gold bar casting method, the laser welding method, and the drill and tapping method-are used to manufacture locators bar system.5 If the retention in the plastic male part of the locator is reduced due to friction, the locator can be replaced, as can other attachments. If the retention in the metal female part of the locator is reduced due to wear, it is difficult to restore.6 Using the drill and tapping technique, however, the female part can be replaced, thereby easily recovering the retention.
In these cases, locator bar overdentures using the drill and tap technique were presented.
CASE REPORT
In the first case, a 55-year-old healthy woman visited the authors' hospital for re-treatment of her maxillary fixed partial denture and mandibular removable partial denture, which had been used for more than 10 years. All the remaining teeth were floating. After the extraction of all the remaining teeth, a complete denture in the maxilla and an implant overdenture in the mandible were planned. No medical history of implant installation concern was found.
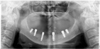
One week after the extraction of all the remaining teeth, an impression was obtained using alginate impression materials (Tokuso A-1, Tokuyama Dental Corp., Tokyo, Japan) for the manufacture of a temporary denture. A temporary denture was prepared and the mandibular temporary denture was duplicated to prepare a stent for the diagnosis and operation of implants, followed by the installation of the implants at 3 months after the extraction (Osstem US II, Osstem Implant Co., Busan, Korea) at sites #33, 36, 37, 43, 46, and 47 (Fig. 1). A rigid type prosthesis which was supported by multiple implants was planned, so milled bar and Locator were assembled. Two weeks after the implantation, relining was performed using a tissue conditioner (Coe comfort, GC America Inc., Alsip IL, USA). After 6 month healing time for osseointegration, a final impression for a complete denture in the maxilla and a preliminary impression in the mandible at the fixture level were obtained using vinyl polysiloxane impression materials (Imprint II, 3M ESPE, St. Paul, MN, USA) by pick-up impression technique. To accurately transfer the position of the implants to the master cast, the impression coping (Osstem Implant Co., Busan, Korea) was splinted in the master cast using autopolymerized acrylic resin (GC Pattern Resin, GC Corp., Tokyo, Japan). After the impression coping was separated into individual copings, fastening and splinting were performed in the oral cavity, after which a final impression was made using vinyl polysiloxane impression materials (Imprint II, 3M ESPE, St. Paul, MN, USA) at the fixture level. The master cast was prepared using improved dental stone (GC Fujirock, GC Europe, Interleuvenlaan, Leuven, Belgium), and the recording base was prepared using autopolymerized acrylic resin (Orthodontic resin, Dentsply International, Milford, DE, USA). The lip support was checked using a silicone medium (Fit checker, GC Corp., Tokyo, Japan), and the interocclusal record was obtained using recording wax (Aluwax, Aluwax Dental Products Co., Allendale, MI, USA), followed by mounting. After preliminary artificial teeth arrangement was performed, the lip support and facial appearance were again assessed in the oral cavity. The interocclusal space was also assessed. A silicone index (Express STD, 3E ESPE, St. Paul, MN, USA) was prepared using the arranged teeth, after which it was used as a reference for setting the bar location. In this case study, a large dead space was expected to be formed in the anterior region of the mandible if the splinting was performed with a cross-arch. Based on the maxillary complete denture and the implantation in the mandible with good bone quality, the milled bar was bilaterally prepared. Drill and tapping technique was presented by schematic diagram (Fig. 2).The plastic sleeve was placed for the Locator (Zest Anchors, Inc., Escondido, CA, USA) (Fig. 3), after which the bar was cast. Subsequently, after the locator was checked with a tapping tool, the Locator female part was fastened to the bar with a force of 20 Nm (Fig. 4). The bar fitness was checked in oral cavity, as was the sufficiency of the interocclusal space. The metal framework and the Locator metal housing were connected using autopolymerized acrylic resin (ADFA, Shofu, Inc., Kyoto, Japan) (Fig. 5). In oral cavity, milled bar and the metal framework were checked, and the lip support and facial appearance with the wax denture were finally checked after the teeth arrangement. After denture curing and lab remounting, selective grinding was performed to form a fully balanced occlusion. The final denture was placed in the oral cavity. The stability, retention, and support of the lip support, esthetic, and denture were shown to be appropriately secured. The blue plastic male part (Zest Anchors, Inc., Escondido, CA, USA) of the Locator was used for retention (Fig. 6. A, B).
In the second case, a 61-year-old healthy woman visited the authors' hospital for re-treatment of her unsatisfying complete denture. According to the intraoral findings from her first examination, in the mandible, severe residual bone loss was observed. A complete denture in the maxilla and an implant overdenture in the mandible were planned. No medical history of implant installation concern was found.
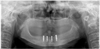
The mandibular denture was relined by a tissue cocnditioner (Coe comfort, GC America Inc., Alsip, IL, USA) and was duplicated, a stent was prepared for the diagnosis and operation of implant, followed by the installation of the 4 implants (Osstem US II, Osstem Implant Co., Busan, Korea) in front of mental foramen area because of alveolar bone deficiency in the molar region (Fig. 7). Overall procedure was simlliar to the first case. But in this case, resilient type prosthesis which allows movement in the distal edentulous area was planned, so Hader bar, clip, and locator were assembled. (Fig. 8. A, B).
DISCUSSION
Overdenture treatment using implants can secure the appropriate stability, support, and retention of the denture, and allows functional recoveries such as lip support, esthetic, and phonation via a denture flange.7 Celik and Uludag8 reported that more stress was observed in the solitary type than in the bar splinting type when the photoelastic stress distribution was assessed in overdentures with three mandibular implants according to the retention mechanism. When a bar attachment is planned after three or more implants are installed for stress distribution, the inter-arch space must be assessed. Pasciuta et al.9 reported that at least 14 mm interocclusal space was required when considering teeth size, denture base thickness, bar thickness for the rigidity, the space from the mucosa to the bar for hygiene, and the soft tissue thickness. If the interocclusal space is insufficient, the bar manufacturing may cause a prosthesis overcontour, denture fracture, or poor oral hygiene.10 When considering attachments for retention with bar splinting, ERA attachments for the resilient type, and a multiple clip with different directions, friction pin, and swivel latchet for the rigid type have been previously used.4 Such attachments had the disadvantage of retention loss due to the wear caused by the repeated insertion and removal of the denture.11 In case of wear, plastic male parts can be replaced. Metal female parts, however, require remanufacturing of the prosthesis. To solve this problem, a Locator can be used. It is very durable and allows 0.2 mm vertical movement. It can be used with a bar as it has the lowest vertical height6 and enables the metal female part to be replaced using the drill and tapping technique, unlike with other methods. The biggest advantage of a drill and tapping technique is that it can achieve total retrievability by just replacing new metal female part.
In these cases, one case was a rigid-type prosthesis that was supported by the implants, the other was a resilient-type prosthesis that was supported by the tissue and implants. Using the drill and tapping technique to connect the bar and the locator, female part wear can be easily managed during regular management.
CONCLUSION
Overdenture treatment using implants can provide stability, support, and retention to a denture for fully edentulous patients. Via the Locator bar system using the drill and tapping technique, retention loss due to the wear of the attachments can be resolved and total retievability can be achieved by easily replacing the female parts.






 XML Download
XML Download