

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Conventional maxillary complete denture and implant-supported mandibular denture are standards of care for edentulous patients.1-3 The following benefits of an immediately loaded implant-supported prosthesis in edentulous patients are reduced surgical and prosthetic visits along with improved function and patient's comfort, as for a functional prosthesis delivered immediately after surgery.4,5 Immediate loading of mandibular overdenture supported by 2 to 4 implants connected with a gold bar appears as a very promising treatment modality similar to delayed loading protocol.6,7 Ball, magnet and bar attachments have been commonly used to retain implant-supported overdenture over the last several decades. Despite the greater retention and low maintenance of bar attachment system,8,9 a longer clinical time and an increased cost are associated in bar attachment system. Besides, soldering or laser welding procedure is often required for the appropriate adaptation of bar to compensate the dimensional change due to impression and laboratory errors.
These problems can be solved by SFI-Bar® (Cendres et Métaux, Biel/Bienne, Switzerland). The system is mounted by bar tubes and retentive balls as connectors to the implants. The retentive element for the denture is the bar tube which can be shortened to any length so that all inter implant distances from minimally 8 mm up to a maximum of 26 mm can be treated. In addition, the adaptor is allowed to have 15 degree of implant angulation. As some parts of system are not fixed to one bar by soldering or welding, there is room for stress release that avoids implant preload. Moreover, the absence of soldering joints, which sometimes reduce the length of the retentively usable bar surfaces, also can be advantageous. As soldering is not required, there is no risk of corrosion, which also supports using titanium grade 5 as a bar material. This clinical report outlines a method of rehabilitating a mandibular edentulous patient with an immediately loaded implants supported by bar overdenture.
CASE REPORT
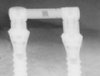
A 65-year-old Korean female visited the Department of Dentistry at the Korea University Medical Center for a new denture on the mandible because of unstable lower denture with pain in the region. Her medical history included hypertension controlled by medication. She was wearing an old denture which was made in Russia 20 years ago. On clinical examination the patient showed maxillary partial edentulism and mandibular full edentulism (Fig. 1A). She had been wearing removable partial dentures (RPD) on the maxilla and complete denture (CD) on the mandible. The patient was advised to opt for the implant supported fixed prosthesis with distal cantilever as suggested by Brånemark. Considering severely absorbed mandible, inadequate lip support and cost effectiveness implant supported removable prosthesis was chosen as a treatment. Therefore, placing two implants in the mandible and immediately loading on them with her old denture was suggested to the patient as a treatment option. In preparation for the procedure and due to patient's medical status, she consulted with her physician. She was instructed to hold out from aspirin for 5 days prior to surgery. Upon clinical and radiographic evaluation, the mandible was classified as type 1 for Complete Edentulism Class D according to Misch classification (Fig. 1B).10 Before surgery, the old denture was rebased as the vertical dimension was lost. Alginate impressions (Aroma Fine DF II, GC, Tokyo, Japan) of the edentulous arches were taken and the patient's mandibular denture was duplicated. This duplicated denture was used as a guide to fabricate the radiographic and the surgical templates. A supra-crestal incision was made from the canine extending to the other canine in contralateral side. Then 3.3×10 mm implants (SLActive Standard, Straumann, Basel, Switzerland) were placed between lateral incisor and canine on each side. SFI-bar® adapters (Lot 142333, Cendres et Métaux, Biel/Bienne, Switzerland) were connected to each implant fixture with 35 Ncm of torque (Fig. 2). The soft tissue was sutured. A Tube bar gauge (Cendres et Métaux, Biel/Bienne, Switzerland) was connected to the tube bar (Lot 113198, Cendres et Métaux, Biel/Bienne, Switzerland). The end of the gauge was fitted into the implant adapter. Thus, the tube bar gauge could be fitted into the other implant adapter (Fig. 3) and the inter-implants distance was measured. The tube bar with the tube bar gauge were removed from the mouth and separated with Premium Disc (08000100, Cendres et Métaux, Biel/Bienne, Switzerland) (Fig. 4). The separated surface was polished, and two pieces of bar were reconnected with mechanical interlocking (Fig. 5). The tube bar was 2.8 mm away from gingiva. SFI-bar® asymmetrical female (Lot 136209, Cendres et Métaux, Biel/Bienne, Switzerland) was separated into two pieces considering the length of bar and was attached to the bar. The old denture was hollowed out to be placed on mandible without any premature contact (Fig. 6). The space under the bar was blocked out with polyvinyl siloxane (Injection type, 3M ESPE, MN, USA). The asymmetrical female was attached to the denture with self-curing attachment processing material (ERA PickUp, Germany) in the mouth (Fig. 7). On 2 week follow-up appointment, denture adjustment and relining was proceeded. The patient was given oral hygiene instructions and was scheduled for follow-up appointments. After 3 months, periapical standard view was taken. There was not any special symptoms found during intra oral exam as well as radiologic change (Fig. 8) and the patient was very satisfied with the new denture.
DISCUSSION
Patients with a severely resorbed edentulous mandible often complain of denture instability and discomfort in the denture bearing area caused by the pressure on the mental foramen. Implant supported overdenture using bar attachment system can be offered to the suffering patients to provide adequate denture stability. In this case, the pre-fabricated bar system required straightforward procedure and allowed the clinician to provide an immediately loaded overdenture to the patient with the added benefits of reduced time and cost. Patient's satisfaction was significantly increased when immediately loaded prostheses were delivered at the time of surgery. Otherwise, patients would be left without dentures for a while and often complain of denture instability as well as persistent pain thereafter.11,12 Immediate loading of mandibular overdenture supported by 2 implants splinted with a gold bar is a very promising treatment modality.13 It has been reported that there was no significant difference in the survival rate between immediately loaded implants and delayed loaded implants in the rehabilitation of edentulous jaws.6,14,15
Non-submerged implants have an internal implant-abutment connection, resulting in better stress distribution. Hence, in 2 implant tissue supported overdenture, non-submerged type implants are considered more appropriate than submerged type implants. It is important, however, that the nonsubmerged implants should be placed in a parallel position to each other, as non-parallel implant angulation cannot be prosthetically compensated readily as much as compensated in submerged implant system. Although a study states that non-splinting implants were comparable with splinting implants when immediately loaded for the rehabilitation of the edentulous mandible, bar attachment would aid in stress distribution. The prefabricated SFI-Bar® utilized in this case is the innovative chairside simplified solution that eliminates the need of soldering or welding procedure and pre-fabricated bar can overcome laboratory errors encountered in conventional bar attachment. From patient's perspective, as immediately loaded implant supported overdenture is delivered for function on the same visit just after surgery, it is a more favorable treatment modality considering reduced treatment time and costs.
The immediate loaded overdenture with SFI-Bar® is a desirable treatment modality particularly in patients with a severely resorbed edentulous mandible. However, the limitation of this system is that a previous denture is required, weather it is a new provisional denture or an old denture for immediate loading. Additionally, an acrylic resin base is preferred to a metal base as the denture base. The presence of adapter and joint components of bar attachment may be attributed to the increased risk of prosthetic fracture; a thorough preoperative diagnosis should be taken. It is recommended to cut the prefabricated bar under water coolant where possible, to reduce substantial heat generated while cutting the bar. Patients should be routinely followed for the care of implant components and denture and periodic denture reline is necessary to avoid detrimental stress on implants.







 XML Download
XML Download