This article has been
cited by other articles in ScienceCentral.
Abstract
Flabby ridges commonly occur in edentulous patients. Inadequate retention and stability of a complete denture are the often encountered problems in these patients. A liquid supported denture due to its flexible tissue surface allows better distribution of stress and hence provides an alternate treatment modality in such cases. This case report presents the use of a liquid supported denture in a patient with completely edentulous maxillary arch with flabby tissue in anterior region opposing a partially edentulous mandibular arch.
Keywords: Liquid supported denture, Flabby ridges, Flexible tissue surface
INTRODUCTION
'Fibrous' or 'flabby' ridge is a superficial area of mobile soft tissue affecting the maxillary or mandibular alveolar ridges. It can be developed when hyperplastic soft tissue replaces the alveolar bone and is a common finding, particularly in long term denture wearers.
1 Such ridges are reported to be caused due to trauma from denture bases.
2 In the edentulous patient, it is found more commonly in the anterior region.
3-
5
Histologically, flabby ridges are composed of hyperplastic mucosal tissue and loosely arranged fibrous connective tissue and dense collagenised connective tissue. In the soft tissue, a great amount of metaplastic cartilage and/or bone are observable.
6
Prosthetic rehabilitation in these patients can be challenging. Major problems encountered in these patients are loss of stability and inadequate retention of the dentures. These problems occur because of the easily distorted flabby tissue during impression taking. Treatment options for these patient's include surgery, implant retained prosthesis or conventional prosthodontics without surgical intervention.
1 Treatment modality has to be chosen depending on patient's state of health and need, extent of flabby tissue, financial capacity and skill of the dentist. In most situations, surgical intervention or use of implants is not possible and conservative management is the treatment of choice.
In 1961, Chase
7 introduced the use of elastic impression material to relieve traumatised tissue. But this can be only a temporary provision. Moreover, it might easily derive candidal growth. In a flabby ridge condition, an ideal denture should be able to withstand masticatory forces and have flexible tissue surface to reduce stress concentration and trauma on the underlying tissues.
8 A liquid supported denture can hence be a solution for this problem.
This case report describes the use of a liquid supported denture in a patient with completely edentulous maxillary arch with flabby tissue in anterior region opposing a partially edentulous mandibular arch.
CASE REPORT
A 52 year old female patient reported to Goa dental college and hospital (GDCH) for replacement of missing teeth. The patient had a history of wearing a maxillary complete denture for 5 years. Her chief complaint was the poor fit of the denture and it felt loose while eating. She was also using denture adhesive. Missing mandibular teeth were not replaced by any prosthetic treatment. By intraoral examination, a completely edentulous maxillary arch with flabby tissue existing in the anterior region (
Fig. 1) and a partially edentulous mandibular arch (Kennedy's Class II) were observed (
Fig. 2).
Keeping the various challenges associated with the case, clinical steps and treatment plan was modified to suit the patient's need. It was decided to give a maxillary complete denture (liquid supported) opposing a mandibular cast partial denture.
Primary impressions were made with alginate (Zelgan, Dentsply/caulk). On the maxillary cast, a special tray was made with two posterior handles. Border molding was performed by using low fusing impression compound (Aslate, India) and medium body addition silicone wash impression (Aquasil, Dentsply/caulk) was made. The flabby tissue was marked in the mouth and transferred on the tray. This area on the tray was cut to form a window to expose the flabby tissue. It was recorded in rest position by injecting light body addition silicone material (Aquasil, Dentsply/caulk).
For the mandibular impressions, a cast framework replacing the missing teeth was tried and adjusted. An altered cast impression technique was used to get the master cast. Jaw relations were recorded. Face bow transfer was made and casts were mounted. Teeth were set and the try in procedure of the waxed denture was done.
The upper denture design was modified to make a liquid supported denture. Lower cast partial denture was acrylised using conventional procedure.
Steps in fabricating a liquid supported denture:-
-
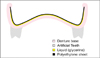
Vaccum heat pressed polyethylene sheet of 1 mm thickness was adapted on the master cast. The sheet was made 2 mm short of the sulcus and was not extended in the PPS area. This sheet was incorporated in the denture at the time of packing (Fig. 3).
Upper complete Denture (with 1 mm thick sheet) and lower cast partial denture were then delivered after making occlusal adjustments. The patient was recalled after 2 weeks to convert the denture into a liquid supported one. This was done to check the comfort level of the patient to the polyethylene sheet.
At recall appointment, the 1 mm thick sheet which was used as a spacer was removed from the denture (Fig. 4). Due to removal of the sheet crevices were formed all along the denture borders. These crevices were helpful in final placement of 0.5 mm thick sheet. An addition silicone putty impression was made of the tissue surface of the denture and cast was made of it (Fig. 5). This was done to record the exact junction of the sheet to the denture. On this cast a 0.5 mm thick polyethylene sheet was vacuum pressed which was used in place of 1mm thick sheet creating a 0.5 mm space.
The polyethylene sheet was cut using the putty index as guide. The borders of the 0.5 mm thick sheet were placed in the crevice formed due to removal of 1 mm thick sheet. Cynoacrylate adhesive and autopolymerising acrylic resin were used to seal the borders and prevent escape of liquid.
The space created due to the replacement of a 1 mm thick sheet with a 0.5 mm thick sheet was filled with glycerine. This was done by making two holes in the buccal flange area of the denture and injecting glycerine through these holes and checking the vertical dimensions simultaneously. The holes were sealed using self cure acrylic resin.
Finally the upper liquid supported denture was delivered (
Fig. 6,
7,
8). Denture care instructions were given to the patient. Patient was told to clean the tissue surface using soft cloth. Recall appointments were scheduled at 1 day, 1 week, 1 month and 3 months. At 1 week appointment, patient complained of floating feeling. But, at 3 months recall appointment, patient was comfortably using the denture. The denture was well maintained.
DISCUSSION
Major problems associated with this case were the presence of flabby tissue in maxillary arch (anterior portion) and the presence of natural dentitions in the opposing arch causes unfavourable distribution of forces that can cause unfavourable tissue changes. These problems were solved by modifying the impression procedures and by fabricating upper liquid supported denture.
Liquid supported denture is based on the theory that when the force applied on the denture is absent, the base assumes its preshaped form that is the one during processing. But under masticatory load, the base adapts to the modified form of mucosa due to hydrodynamics of the liquid improving support, retention and stability.
9 There will also be optimal stress distribution of masticatory forces over a larger area which reduces tissue overloading.
9 Prevention of soreness and increased comfort level are other advantages of the liquid supported denture.
9,
10
In this case, polyethylene thermoplastic clear sheet (Biostar vaccum forming machine, Scheu-dental, Germany) was used because of its softness, flexibility and biocompatibility. Glycerin was used because it is clear, viscous, and biocompatible and also has been used as a vehicle in liquid medications.
CONCLUSION
Fibrous ridges pose a prosthodontic challenge for the achievement of stable and retentive dental prostheses. Surgical removal of the fibrous tissue and implant retained prostheses may not be possible to be used in all cases. Considering conventional prosthodontics, the use of liquid supported denture can further improve the patient's acceptance due to more uniform distribution of forces and due to the improved comfort level.


 PDF
PDF ePub
ePub Citation
Citation Print
Print









 XML Download
XML Download