

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dental occlusion has been an essential part for all dental works in restorative dentistry. Dental treatment has the ability to basically alter static and dynamic occlusal relationships, while trying to accomplish as near "ideal" occlusion as possible. For dynamic occlusal relationships, there are three main concepts regarding tooth contact during the lateral excursion of mandibular movement: 1) balanced occlusion, which was developed from the work of Bonwill,1 2) canine guidance, described by D'Amico,2 and 3) group function, as discussed by Beyron.3
Tooth loading in canine guidance and group-function occlusions is considered to be different.4 According to Glossary of Prosthodontic Terms (8th edition),5 group function is defined as multiple contact relations between the maxillary and mandibular teeth in lateral movements on the working side. The simultaneous contact of numerous teeth acts as a group to distribute occlusal forces. Whereas canine protected articulation is defined by the glossary as a form of mutually protected articulation in which the vertical and horizontal overlap of the canine teeth disengages the posterior teeth in the excursive movements of the mandible.
Both canine guidance and group-function guidance occlusions are considered normal. The latter occlusal scheme occurs naturally as a result of occlusal wear.6 When an entire occlusion to be restored, either occlusal scheme will serve effectively. However, when only a part of the occlusion is to be restored, the restoration must be consistent with the existing occlusal scheme. Despite which occlusal scheme is used, the dentist must preserve that scheme during routine postoperative appointments.7-11
For the field of restorative dentistry especially during the process of oral rehabilitation, the rationale to choose occlusal scheme could be based on epidemiological data in combination with study on physiology of the masticatory system. For this reason, the purpose of this study was to obtain the epidemiological data on the distribution of 2 major occlusal schemes (group function and canine protected occlusion) as well as associated static occlusal relationship such as vertical and horizontal overlap and its relationship with the occlusal scheme among Thais.
MATERIALS AND METHODS
The population for this study consisted of 104 subjects attending clinic at Faculty of Dentistry, Mahidol University (67 males and 37 females). The age of subjects ranged from 18 - 50 years, with a mean age of 25.01±6.87 years. The study was approved by Mahidol University Institutional Review Board. (MU IRB# 2009/093.1905) Subjects who met the following criteria were selected:
No previous or current orthodontic treatment.
The presence of completed permanent dentition except for the third molars
No previous occlusal adjustments
No large restorations involving the incisal edge or a cusp tip
No crowns or fixed partial dentures
No apparent pathologic periodontal problems
Upper and lower canines in the line of the arch
No tooth showing attrition into the dentine
The static occlusion of each subject was assessed by intraoral examination on a dental chair under direct vision. The incisor relationship were recorded according to the classification of the British Standard Institute.12 Dynamic occlusion was determined with the aid of shimstock with 8 mm width, 8 µm thickness (Almore shimstock, Hanel, Langenau, Germany) to confirm tooth contact.
The examination was carried out with subjects seated in an upright position in a dental chair with the Frankfort plane parallel to the floor. All recordings were made by the same operator in the same period of the day (morning hours) to avoid possible diurnal variation.13 For the lateral excursion, occlusal contacts were recorded on the working and the nonworking sides.
Subjects were asked to perform the movements with the aid of a handheld mirror. The shimstock was placed on the occlusal surfaces of teeth from the canine backward; the subject was then asked to close his/her mandible into maximum intercuspation. Gliding movement was performed to the right or the left while the examiner maintained a constant pulling force on the shimstock. On reaching the 0.5 mm position, the teeth holding the shimstock were recorded as working side contacts. The subject was asked to repeat the movement with the shimstock placed on the opposite side to record the non-working side contact. Occlusal contacts at the protrusive excursion of mandibular movement were recorded at the edge-to edge position. The shimstock was placed on the incisal edges of the anterior teeth. The subject was asked to close into maximum intercuspation and then slide to the edge-to-edge protrusive position while the examiner maintained a constant pulling pressure. Once the teeth were at the edge-to-edge position, teeth holding the shimstock were considered to be in contact and were recorded. The shimstock was then placed on the occlusal surfaces of posterior teeth, and the subject was asked to repeat the same movement to check for the presence of posterior tooth contact.
Chi-square test was used to examine the relationship between types of occlusal scheme and gender as well as the relationship with the presence of interferences. For the comparison of vertical and horizontal overlap distances among types of occlusal scheme, the oneway analysis of variance (ANOVA) was employed. Lastly, the Mann-Whitney U test was used to compare the vertical and horizontal overlap in relation to the presence of protrusive interference. The level of significance for all statistical analysis was set at P=.05.
RESULTS
Total of 104 subjects were included in this study. The ratio for Male to Female was 1.8:1. The mean vertical overlap and horizontal overlap found in this population were 1.94±1.20 and 2.41±1.32 mm respectively.
The majority of the populations (68.3%) possessed group function occlusal scheme. For the remaining, 17.3% of the populations possessed canine protected occlusion, 12.5% possessed combination of both occlusal schemes. There were 2 subjects (1.9%) with their occlusal schemes unclassifiable as there was only one pair of the opposing posterior teeth in contact during lateral excursions.
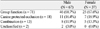
The study also found that majority of the populations (79.8%) did not have any occlusal interference. For the population with occlusal interference (20.2%), we found that the most common interference was protrusive interference (57.14%), the second was balancing interference (38.1%) and the third was working interference (4.1%). Next we examined the distribution of occlusal scheme within each gender as well as the distribution of gender within each occlusal scheme and discovered that there was no statistical differences (Chi-square test; P=.743) for either distributions. There was almost equal distribution of group function, canine protected occlusion and combination occlusal scheme for each gender (Table 1).
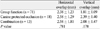
For the incisal relationship, the distance of both horizontal overlap and vertical overlap were not statistically different among both occlusal schemes and the combination group. On the other hand, there was a tendency of less vertical overlap in group function when compared to canine protected occlusion occlusal scheme. However, there was no statistical significant difference for this observation (Table 2).
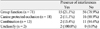
Our study revealed that the majority in each occlusal scheme does not process occlusal interferences ranging from approximately 89% in canine protected occlusion to 79% in group function (Table 3). However, there was no significant relationship between the presence of interferences and occlusal scheme (Chi-square test; P=.743).
Lastly, we examined the difference in distance of horizontal overlap and vertical overlap in population with or without protrusive interferences (Table 4). We found that for vertical overlap, there was less distance for the population with protrusive interference (1.33±0.62 mm) than the distance for the population without the protrusive interference (2.02±1.24 mm).
DISCUSSION
Our findings of the majority of studied population processed group function occlusal scheme. This is similar to the earlier epidemiological data such as study by Beyron3 showed fairly overwhelmingly that adult Australian aborigines had group function occlusion. Weinberg14 found that 81% of his studied population possessed group function occlusal scheme, whereas only 5% had canine guided occlusal scheme. By contrast, Scaife and Holt15 examined 1200 individuals, and discovered that the majority had either unilateral or bilateral canine protected occlusion. The discrepancy among studies may be due to the difference in examined population, culture and regular food intakes as well as influence of the materials used to register the contacts. As Tarazi et al.16 demonstrated that the number of recorded tooth contacts varies with the material used to record registrations.
For the occlusal interference, Posselt17 described this term as a cuspal contact forcing the mandible to deviate from a normal pattern of movement. The eighth edition of the glossary of prosthodontic terms5 states an occlusal interference as any tooth contact that inhibits the remaining occluding surfaces from attaining stable and harmonious contacts. Ash and Ramfjord18 described the term occlusal interference as an occlusal contact relationship that interferes in a meaningful way with function or parafunction. Even though there were slight differences of definition of this term, it has been long a subject of interest, study and debate in dental field. Our study found that majority of the population does not process occlusal interferences. The type of occlusal interferences that has the highest percentage is protrusive interference followed by balancing side interference. This is surprising that our finding was less occlusal interferences which the most common was balancing or non-working interference.
The result of the incisal relation found from this study was similar with previous study18 in the Thai population. They found the average of vertical overlap (2.28±1.13 mm) was greater than horizontal overlap (2.68±1.1 mm). They also found that the common range of vertical overlap was 1 - 3 mm. and the horizontal overlap was 2 - 4 mm. This finding was similar to our finding. Interestingly, we found that the shorter distance of vertical overlap was found in the population with protrusive interference. However, there was no difference for the horizontal overlap between the population with or without protrusive interference.
A number of limitations can be noted in the above mentioned studies. No reference was made to the location of the canine in terms of its relationship to the line of the arch nor to the degree of attrition of the canine, which is of particular importance in examining the assumption that attrition could lead from one type of contact during lateral movement to another.19 In this study, subjects with marked attrition were excluded based on the assumption made by McAdam4 and Woda et al.19 that canine guidance and group function appear to correspond to two successive states of the evolving dentition under the effect of attrition.
The inclusion criteria for this study were set to assure the presence of a natural dentition as well as the absence of noticeable periodontal problems. These criteria were set because the neuromuscular control of occlusal stability as well as masticatory muscles can be influenced by the periodontal input.20,21
Moreover, the position at which the occlusal contact pattern was recorded (cusp to cusp) may not be representative of the functional range of the lateral excursion of mandibular movement. Chewing kinematics can vary based on several factors such as age, dental static occlusion, facial morphology, and so on.22,23
Another fact for consideration is that changes occurring during the development of occlusion could influence the occlusal contact pattern. Heikinheimo et al.24 reported an increase in occlusal interferences between the ages of 12 and 15 years. Other studies showed a decreasing prevalence with increasing age.19,25,26 The fact that the sample was composed of subjects aged from 18 to 50 years, could be the explanation for the slight differences in the result from other studies as the changes occurring during occlusal development could influence the occlusal contact pattern.
CONCLUSION
This study demonstrated that among Thais, the most common occlusal scheme is group function, but there was no demographic or occlusal factors that strongly related to any particular occlusal scheme. However, we did not focus our study on the exact association between other static occlusal relationship parameters such as Angle's classification with the other dynamic occlusal relationship parameter other than occlusal scheme. This should be conducted in the future study.

 XML Download
XML Download