

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
As the role of dental implants in the oral rehabilitation has become more important, reducing the failure rate of implant treatment has become one of the most concerned problems. Osseointegration has been thought to be the most important prerequisite for the long-term success of the dental implant. Implant stability at the time of implant fixture placement, known as the primary stability, has been suggested as the crucial factor for achieving successful osseointegration.1,2 It has been thought that primary stability largely depends on the three major factors: (1) the implant bed condition such as bone quantity and quality, (2) the mechanical shape of the fixture placed in the bone, and (3) the procedure how the fixture has been inserted in the bone.3
A number of test methods to assess the primary stability have been suggested: histology and histomorphometry, insertion torque, removal torque, push-through and pull-through, radiographic assessment, Periotest ultrasonic method, and resonance frequency analysis.1 Among these test methods, resonance frequency analysis has been revealed and widely used as the most effective method to evaluate primary stability because of its easiness, accuracy, and non-invasiveness.4-11
A device called Osstell (Integration Diagnostic Ltd., Goteborg, Sweden) was invented to measure the resonance frequency value of the implant fixture through the transducer which is mounted directly to the fixture with a screw. The instrument measures the resonance frequency and display the result as the implant stability quotient (ISQ) value on a scale from 1 to 100. Higher ISQ value means higher resonance frequency value, which means more primary stability. Finite element analysis also has been recently used to analyze the mechanical and vibration behavior of the three dimensionally designed structure.12-15
The aim of this study was to investigate the influence of bone quality and surgical technique on the ISQ value. Moreover, by means of the finite element analysis, a three dimensional implant fixture-bone structure was also designed to evaluate the correlation between density of bone surrounding the implant fixture and resonance frequency value of the structure.
MATERIALS AND METHODS
Implant
Six Brånemark - type parallel implants with anodized oxidation surfaces (3.75 × 7 mm, Warantec, Seoul, Korea) were prepared for this study. Each implant was used nine times so that the total number of implant installation was 54 in this experiment. After each removal of inserted implants, the fixtures were cleansed with streaming water and re-used for next installation.
Specimen
Two different types (type 1 and type 2) of bone specimens from pig rib bone were prepared for this experiment (Fig. 1). Type 1 bones were harvested from the distal part of the pig rib with thick cortical bone and dense cancellous bone. Type 2 bone was harvested from the proximal part with less cortical bone and loose cancellous bone in comparison with the distal region. The bones were sawed to get about 4 - 5 cm long and the upper parts of cortical portions were trimmed away so that only cancellous components could be in direct contact with implant fixtures. Nine bone specimens for each type of bone were made from nine pig rib bones.
Surgical procedure
For each bone sample, three implant fixtures are installed in three different types of installation methods: (1) Compaction, (2) Self-tapping, and (3) Tapping (Fig. 2). To get rid of the potential influence of implant location in bone sample on the ISQ value, each implant of different insertion technique was placed in middle for three times and in edge for six times for each bone type.
In the conventional tapping technique, the implant sites were marked first by 1.5 mm diameter round bur with drill speed of 1000 rpm, followed by twist drills of 2 mm diameter, and 3 mm diameter with 500 rpm. Finally tapping was performed in the drilled holes before the implant fixture installation. The fixtures were then inserted with an Elcomed (W&H Dentalwerk, Bürmoos GmbH Austria) with engine speed of 30 rpm.
For the self-tapping installation method, round bur was used first to make a mark on the implant site, and twist drills of 2 mm/3 mm in diameter were used in sequence to make drill holes for implant fixture installation. The implant fixtures were then installed with engine speed of 30 rpm.
In the cancellous compaction technique, the implant sites were first marked by 1.5 mm diameter round bur and drilled with 2 mm wide twist drill. Then the holes were subsequently widened using varying diameters of taper-type osteotomes (2 mm/2.5 mm/3 mm) by light malleting until holes of 3 mm diameter were obtained. In the prepared holes, the implant fixtures were inserted with 30 rpm.
Implant stability measurement
Immediately after three implant fixtures were installed differently in each bone sample, the resonance frequencies were measured using Osstell (Integration Diagnostic Ltd., Goteborg, Sweden). The L-shaped transducer was firmly connected by hand-screw and the ISQ values were recorded in two different orientations perpendicular to the long axis of bone samples.
Statistical analysis
The data were analysed by using SPSS statistics 17.0 (SPSS Inc., Chicago, IL, USA) with 5% of significance level. The average value and standard deviation of ISQ value for each six groups was calculated. Student t-test was used to compare the ISQ values of two independent groups of different surgical techniques in each bone type. One-way ANOVA test was used for the comparison of the ISQ values of three different surgical procedure groups in each bone type.
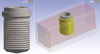
Finite element analysis
A three dimensional model for finite element analysis was created by using a finite element analysis program (ANSYS 12.1, ANSYS, Canonsburg, PA, USA) on a personal computer. Like the implant fixtures used for RFA study, a fixture model was designed to the shape of Brånemark type straight implant fixture with thread. The block bone model was composed of three compartments: (1) outer cortical bone, (2) inner cancellous bone, and (3) interfacial bone between implant fixture and cancellous bone (Fig. 3). To mimic the actual RFA experiment, the upper and the two side of cortical bone was removed. The interfacial bone layers surrounding the fixture were created to be 0.2 mm in thickness. All interfaces between two different compartments were assumed to be perfectly boned, and the model was medium meshed to generate 23764 elements and 60365 nodes.
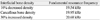
The titanium (Density of 4.5 g/cm3, Young's modulus of 117,000 MPa, and Poisson's ratio of 0.3) was chosen as the material of the model implant, and both cancellous and cortical bones were assumed to be orthotropic and linearly elastic.12,14 For the interfacial bone layer, three different densities were defined : (1) normal cancellous bone density, (2) 30% increased density of the normal cancellous bone, and (3) 10% decreased density of the normal cancellous bone. All three interfacial bone layers were assumed to be orthotropic and linearly elastic, having same Poisson's ratio with cancellous bone. Each Young's modulus, however, was calculated from the equation E = Cu0.06ρ3 (where E is Young's modulus, C a constant, u the strain rate during testing, and ρ the density of bone).16 All the material properties of titanium, cancellous bone, cortical bone, and three interfacial bone layers are presented in Table 1.17,18
The resonance frequency of the model could be determined in the harmonic response analysis by forcing varying frequencies of cyclic loads and observing the maximum displacements for each corresponding frequency. On the cyclic load of the resonance frequency, the maximum displacement of the model would be increased dramatically. For three different interfacial bone layers, each resonance frequency was determined.
RESULTS
Resonance frequency analysis
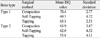
The mean values and standard deviations calculated are shown in Table 2 and Fig. 4. In each type of bone, the Compaction group has the highest mean of ISQ value and the tapping group has the lowest mean of ISQ value. All surgical technique groups showed higher ISQ values in type 1 bone than in type 2 bone. The result of one-way ANOVA test showed that statistically significant difference in ISQ values between three different surgical techniques existed in each of the bone types (Table 3). The student t-test revealed statistically significant differences in ISQ value between the Self-tapping group and the Tapping group, and between the Compaction group and the Tapping group for each type of bone (P < .05). However, the Compaction and the Self-tapping group were not significantly different in both type 1 and type 2 bones (Table 4).
Finite element analysis
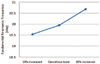
The fundamental resonance frequencies for the three dimensional models with three different density of interfacial bone layers were determined and the result is presented in Table 5 and plotted in Fig 5. The result showed that the first mode of resonance frequency was increased as the interfacial bone layer becomes denser.
DISCUSSION
This study was to examine the influence of bone quality and surgical technique on the implant stability quotient (ISQ) value. Two different types of bone (type 1 and type 2) were extracted and the same implants were installed in three different ways.
A clinical instrument was recently developed to analyze resonance frequency, which is calculated into the implant stability quotient (ISQ). Some authors4,19 have shown strong correlation between ISQ value and cortical bone thickness, which suggests that cortical bone thickness plays a crucial role for implant primary stability. It has been reported that no statically significant difference in ISQ value existed between different implant design types.20 In the aspects of surgical technique, especially between conventional drilling technique and osteotome technique, some authors21 have concluded that the cancellous compaction technique increased the ISQ value than the conventional drilling technique. However, the other author22 has shown that osteotome technique resulted in decreased ISQ value, thus less primary stability, than conventional drilling technique.
In this study, only Brånemark type of straight implants were used so as to get rid of the influence of implant design to ISQ value. According to the quality of the cancellous bone, two types of bone were grouped: (1) type 1 bones were gained from the distal portion of the pig rib bone where cancellous bone is denser, and (2) type 2 bones were extracted from the proximal part where cancellous bone is less dense than that of distal region. Upper cortical portions in all samples were trimmed off to exclude the influence of the cortical bone.
Comparing the results between type 1 and type 2 bones in each surgical method, the ISQ values in type 1 bones were significantly higher than those in type 2, which suggests that density of bone has positive relation to the implant primary stability. Among three different insertion methods, the Tapping group showed the lowest ISQ value in both bone types. As a matter of fact, when removing the inserted fixture from the bone sample, especially in type 2 bone, it was so weekly anchored that even hand force would be enough to remove the implants. This result suggests that tapping before the implant placement is not a recommended procedure if implant fixture site is absent of or with little cortical bone and not enough dense cancellous bone.
This study showed slightly higher ISQ mean values in the Compaction group than the Self-tapping group, but the difference was not statistically significant in both bone types. In fact, the drilled hole size right before the fixture placement was 3 mm in diameter in the Self-tapping group, and the size of implant used was 3.75 mm in diameter, so during the self-tapping procedure, the cancellous bone would have been compacted in some degree. This un-intended cancellous compaction from fixture itself might have raised the ISQ value approximately to the level of Compaction group. If we had used bigger size of final drill for implant fixture bed preparation in Self-tapping group, the expected ISQ value would have been a little bit lower.
Through the finite element analysis, we could confirm that quality of bone directly surrounding the implant fixture plays a crucial role in determining resonance frequency. The resonance frequency value of the model increased as the density of the interfacial bone surrounding the implant fixture increased.
CONCLUSION
The present study showed that both bone quality and surgical technique have influence on the implant primary stability. Therefore, we could confirm that quality of bone directly surrounding the implant fixture plays a crucial role in determining resonance frequency.
According to this experiment, the followings could be concluded:
In each three different surgical technique groups, the ISQ values were higher in type 1 bone than those in type 2 bone.
Among three different insertion methods, the Tapping group showed the lowest ISQ value in both type 1 and type 2 bone.
In both bone types, the Compaction groups showed slightly higher mean ISQ values than the Self-tapping groups, but the differences were not statistically significant.
Increased interfacial bone density raised the resonance frequency value in finite element analysis.






 XML Download
XML Download