

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Adequate treatment planning is one of the most important factors in successful conventional implant prosthesis, requiring clear communication between the prosthetic dentist and surgeon. It becomes more critical when the patient has unfavorable conditions such as a severely resorbed alveolar ridge. Treatment planning must be based on a thorough dental diagnosis and a prognosis assessment for the remaining dentition. Improper planning may result in a range of prosthetic complications and a poor prognosis due to unfavorable mechanical stress and poor oral hygiene. Partial edentulism can be restored with implants by several methods.1 In considering implant placement, the numbers and position of implants should always contribute to the convenience and longevity of a definitive prosthesis fulfilling esthetic and functional demands. Implants in partial edentulous patients involve either fixed type implant prosthesis or removable type implant prosthesis. There are several reports that removable partial dentures with posteriorly-placed implants showed a favorable outcome and counted as an adequate treatment option.2,3
This clinical report concerns the rescuing procedure for inadequately planned prosthodontic case for a partially edentulous patient with severely resorbed alveolar ridge. Predetermined impractical fixed type prosthesis to restore posterior teeth was properly re-evaluated and restored with a removable partial denture with milled bars and magnetic attachments.
CLINICAL REPORT
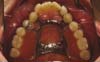
A 26-year-old male patient presented to the Department of Prosthodontics at Yonsei University Dental Hospital to restore the posterior edentulous area. The patient had implant surgery with a sinus lift procedure without proper prosthodontic evaluation. Radiographic examination showed that implants were placed in the area of teeth number #17, 16, 22, 25 and 27 and clinical examination revealed 3 degree of hypermobility on teeth number #15 and #24 (Fig. 1).
Teeth #15 and 24 were diagnosed as hopeless and were extracted. Impressions were made with alginate and casts were poured and mounted in centric relation for prosthodontic evaluation. A provisional denture was fabricated on the articulator and placed in the patient's mouth. Occlusal vertical dimension and phonetics were clinically verified. An impression was made with implant level impression coping and casts were mounted for prosthetic treatment planning. It was determined that implant supported fixed partial denture was not indicated due to severe bone resorption resulting in a poor crown-to-root ratio and buccal placement of implants. So, the treatment option of removable partial denture was presented to the patient which involved fabrication of a milled bar with a magnetic attachment.
A customized abutment and a crown for tooth number #22 were fabricated on the articulator and delivered to the patient. The milled bar was fabricated accounting available interocclusal space, as measured from the vinyl index on mounted casts of provisional denture. A two-degree tapered milled bar wax pattern was fabricated on the master cast and magnet keepers were embedded in the pattern, which was then invested and casted (Figs. 2, 3, 4).
The fit of the milled bar and framework were checked in patient's mouth, and the fit between them was adjusted with a tungsten carbide bur (Bredent Medical, Senden, Germany), and the maxillomandibular relationship was recorded for denture fabrication using an occlusal rim. The tooth arrangement on the trial wax denture was transferred from the prepared index. The prosthesis was remounted on the articulator after polymerization and the occlusion was adjusted on the articulator. The prosthesis was inserted; phonetics, esthetics, function, and comfort were clinically verified. The magnet was embedded in the denture with GC pattern resin at 2 weeks after initial placement of the final prosthesis. Postoperative instructions were given to the patient, and no complications have arisen since insertion of the prosthesis five years ago.
DISCUSSION
As number of implants and their position depend on prosthesis type, making presurgical prosthetic treatment planning critical for the success of the prosthesis. In our case, implant surgery had been performed without proper evaluation of remaining teeth or adequate prosthodontic treatment planning. As a result, two hopeless teeth had to be extracted at six months after initial implant surgery. Because of additional extraction followed implant surgery, supplementary implants were necessary for the fixed-type prosthesis especially due to poor crown to root ratio. However, the patient rejected additional implants placement but accepted a removable prosthesis to reduce treatment time and cost. Removable prosthesis is more advantageous as restore prosthesis with a poor crown-to-root ratio caused by severe resorption of the alveolar ridge. Though guidelines for the crown-to-root ratio in natural teeth are not applicable to implants4, the ratio is still a prognostic indicator.
When treating partial edentulism with implants, an implant-supported, fixed-type prosthesis is usually the first option. It is reported that implant supported removable partial denture is suitable and has advantages to restore Kennedy Class I posterior edentulous patients.5 Those advantages include enhancing retentive or supportive elements of removable partial dentures.6-7 Strategically-placed dental implants in conjunction with the remaining natural teeth can also establish a favorable removable partial denture design by significantly reducing the effect of the reciprocal arm and improving the fulcrum line position.7 In this case two milled bars with magnet attachments connected to upper posterior implants were used to provide enhanced support for the denture. Stability and retention were also improved by the bars and framework.
SUMMARY
This report illustrates how improper planning may prolong treatment and give rise to complicated treatment procedure with poor prognosis. Countermeasures in this case consisted of correcting to an implant supported removable partial denture in conjunction with careful evaluation of the oral condition during treatment. Dental treatment should be based on an adequate treatment plan, and procedures must be guided by proper planning achieved by cooperation between implant surgeon and restorative dentist. Implant-supported removable-type prosthesis with milled bar and attachment is a viable and useful treatment option in patients with improperly placed implants.



 XML Download
XML Download