

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The metal-ceramic crown is currently the most popular complete veneer restoration that can be used in the anterior esthetic zone. Although various types of esthetic all-ceramic crown systems have been introduced to dentistry, many dentists still use a metal-ceramic crown system for anterior restoration because of its higher durability and lower cost compared to alternative all-ceramic systems. However, in many cases, the metal cervical collar on the facial margin was unaesthetic and unacceptable to patients. This metal collar caused dark gingival discoloration, which became the primary disadvantage. This phenomenon was named "umbrella effect" which is characterized by gray marginal gingiva and dark interdental papilla.
Traditionally, the facial margin of a metal-ceramic restoration had a narrow metal collar and could be modified to invisible thin metal. However, even if a thin metal collar was covered by opaque porcelain, an unesthetic gingival portion could be found, especially in cases where the gingiva of the anterior tooth was a thin scalloped type.
Increased esthetic demands led to the development of the porcelain facial margin that eliminated any possible display of a metal collar. Although the facial porcelain margin has been used in place of the metal collar margin, this did not solve problems such as the cervical opaque reflection of porcelain veneer. Especially when the cervical tooth preparation was not sufficient, the opaque color that masked the metal showed through at the cervical region.
Geller stated that it was necessary to overcome dark and shadowed zones in the root structure adjacent to crown margins to obtain a proper esthetic appearance.1 Recently, metal copings have solved this esthetic problem by designing their faciocervical ends 1-2 mm coranally from the shoulder. As a result, the metal was invisible in the faciocervical region, and the opaque reflection in the cervical region disappeared. This framework design allowed increased light transmission to the adjacent root structure.2,3 O'Boyle et al. reported that a 2-3 mm unsupported facial porcelain margin gave better light transmission than a 0-1 mm porcelain margin.4 This type of coping design can be used for enhancing cervical esthetics.
This concept had already been introduced by Choung et al.5 and Behrend.6 The weak point of this design was the unsupported facial margin porcelain, which meant the loss of the ferrule effect of a metal collar. As a result, the strength of the prosthesis could be decreased compared to conventional restorations with metal collars. The unsupported facial porcelain veneer might not be able to resist the stress caused during cementation and mastication. Several studies showed that this modified collarless metal-ceramic crowns had sufficient fracture strength to endure the maximum human incisive biting force.4,7-9 It was suggested that 1 mm of unsupported cervical shoulder porcelain could be used safely in clinical situations.4,9
Currently, enhanced all-ceramic systems such as In-Ceram and Empress 2 make it possible for dentists to use all-ceramic fixed partial dentures (FPDs). However, fractured all-ceramic FPDs were observed frequently. All-ceramic systems must be set and used carefully, because they have inherently lower fracture strength.
A collarless metal-ceramic system has been used successfully as the retainer of anterior metal-ceramic FPD. Its strength is higher than the strength of an all-ceramic crown, and it has an esthetic cervical configuration. This system can be the first choice of retainer in anterior FPDs. However, modified collarless metal-ceramic FPDs could have lower fracture strength than conventional ones, and these FPDs must be used carefully in the patients who have abnormal habits like bruxism and clenching. The purpose of this study was to evaluate the fracture strength of collarless metal-ceramic FPDs according to their metal coping designs.
MATERIALS AND METHODS
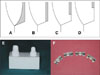
A resin maxillary left central incisor and a maxillary right lateral incisor analogue (Nissin dental products Inc., Kyoto, Japan) were prepared for a collarless metal-ceramic FPD. The preparation followed the protocol of Shillingburg et al., except the proximal wing.10 The preparation finish lines were shoulder at the facial margin and chamfer at the palatal margin. Two finish lines were blended continuously at interproximal margins. These resin teeth were fixed in yellow stone with their axis parallel to each other and vertical to the earth. The distance between the two teeth was as wide as a maxillary central incisor. Two teeth were copied to the same dimension copper dies by a CAD/CAM procedure (Fig. 1). Then, the fabricated copper dies were used as anodes to make a negative mold of the die specimen via electric erosion. The negative mold was used as an injection mold (Fig. 2). Polybutylene terephthalate (PBT) resin was selected as the master die material. The PBT resin (SPESIN®, Kolon Chemical Co., Kumi, Korea) was melted and injected into the prepared negative mold of the specimen. One metal coping of a three-unit FPD was made in advance and used to confirm that the duplicated dies had same sizes in all three dimensions. The metal coping fitted on almost all of the duplicated dies accurately. These dies were used as respective master dies.
Four different facial margin design groups were investigated. Group A was a coping with a thin facial metal collar, group B was a collarless coping with its facial metal to the shoulder, group C was a collarless coping with its facial metal 1 mm short of the shoulder, and group D was a collarless coping with its facial metal 2 mm short of the shoulder (Fig. 3). Each group had 15 specimens.
First, a full contour wax-up of the 3-unit FPD was carried out on the resin die, and indexes for wax coping and porcelain build-up were prepared. The wax-up of copings was done by the dipping method and adjusted by indexes and wax gauge. All of the wax copings were sprued and invested in phosphate-bonded investment (Ceramvest, Protechno, Girona, Spain). Castings were made in Ni-Cr-Be alloy (Rexillium III, Jeneric/Pentron Industries, Wallingford, Conn., USA) with a centrifugal casting machine. After divesting, copings were adjusted again to confirm their size and thickness.
Porcelain build-up was carried out on all prepared copings with feldspathic porcelain powder (Noritake Dental Supplies, Nagoya, Japan). The direct lift technique was used to make the facial porcelain margin. The overall contour and thickness of FPDs were checked with prepared index and metal gauge. The base of the pontic did not contact the die material. If the base contacted the die, the specimen could not be deformed adequately under vertical loading during the fracture test.
Every FPD was adapted to a spare PBT resin die to avoid scratches and deformation of the PBT resin master dies. The adjusted FPDs were finally adapted on the respective master dies.
The prepared resin dies were cleaned with rubber cup and pumice. The inner portion of the facial unsupported porcelain veneer was etched with 37% phosphoric acid (Panavia etching agent V, Kuraray Medical Inc., Tokyo, Japan) for 60 seconds and treated with silane agent. Then, all of the FPDs were cemented to their original dies with dual curable composite resin cement (Panavia F, Kuraray Medical Inc., Tokyo, Japan). Immediately after the FPDs were seated onto their respective dies with resin cement in them, finger pressure was applied, and light cured for 20 seconds. The excess of resin cement was removed and an air-blocking gel (Oxyguard II, Kuraray Medical Inc., Tokyo, Japan) was applied (Fig. 4).
The fracture strength test was carried out using a universal testing machine (Instron 4465, Instron Co., Norwood, MA, USA) at a cross head speed of 0.5 mm/min (Fig. 5). Cemented specimens were fixed on a metal jig for the fracture strength test. The load was directed parallel to the long axis of the teeth. A 6 mm diameter flat end plunger was used to apply load on the incisal edge of the pontic. Aluminum foil folded to about 1 mm of thickness was inserted between the plunger tip and the incisal edge of the pontic. Vertical load was applied until catastrophic porcelain fracture.
One-way ANOVA was used to compare the mean fracture strengths, and Scheffe's test was used to compare all four means with each other.
RESULTS
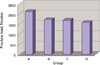
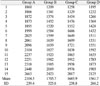
The mean failure loads of group A, B, C, and D were 2105 N, 1706 N, 1686 N, and 1562 N, respectively. The highest failure load exceeding 2000 N was found for the control group A (Table 1, Fig. 6).
One-way ANOVA revealed that there were significant differences between the mean failure loads of the FPDs investigated (P < .05, Table 2). Scheffe's test indicated significant differences between group A and the other groups (P < .05). There was a trend that the failure load decreased as the reduction of framework increased. However, Scheffe's test revealed that there were no statistically significant differences among group B, C, and D (P > .05, Table 3).
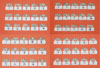
All specimens showed similar failure modes (Fig. 7). Fractures occurred at the facial veneer of pontics and retainers. Palatal veneer was also fractured out in several specimens, which occurred more often in group C and D. The main failure mode of the porcelain veneer was adhesive failure.
Usually, the fracture directions were similar to the direction of load, so the bulk of the facial porcelain was expected to be detached from the metal at the boundary of the porcelain and metal. Cracks seemed to propagate from beneath the loading point to the connectors and finally to the facial and palatal veneer of the retainers. The load that was aligned with the boundary between the metal and facial porcelain seemed to reach disto-facial line angles of retainers. Distal fracture lines of facial veneers were located at those areas where metal support ended (Fig. 8).
The facial veneer of retainers with a large bulk of unsupported porcelain failed at lower load. Almost all of the unsupported facial porcelain veneers were detached from the retainers. On the contrary, many palatal veneers did not fail. The number of retainers that experienced palatal veneer failure were 5, 5, 14, and 19 for group A, B, C, and D, respectively (Table 4). The number of failed palatal veneers increased as the amount of unsupported porcelain increased. The failure of the palatal veneers seemed to occur after the detachment of the facial porcelain veneers from the metal copings.
When fractured FPDs were observed, there were some typical features (Fig. 9, Table 4). Seven out of 30 retainers remained intact after the fracture of pontic porcelain in group A. Four out of 30 retainers in group B remained intact, but all the facial veneer of retainers in group C and D were definitely fractured. In the metal support group A and B, some load values at which the veneer of retainers could be fractured were higher than that of the pontic veneer, so the bonding strength between metal and porcelain in the facial cervical region seemed to be strong enough to survive the load at pontic failure. On the other hand, there were some cases in which the veneer of retainers were fractured without any failure of the pontic facing. Three and two such cases happened in group C and D, respectively. There were no such cases in group A and B. In the facial porcelain margin groups, some load values at which the veneer of retainers could be fractured were lower than those of the pontic veneer. These phenomena seem to indicate that the amount of metal support of facial porcelain veneer contributed a great deal to the strength of the retainers.
The graphs of the fracture tests were typical within each group. In the control metal collar group A, catastrophic fractures happened as soon as the load reached its highest value. In the facial porcelain margin groups, deformation continued for a short period after the load reached the highest value. It was generally true that catastrophic fractures occurred at lower load values past the time of maximum load in group D (Fig. 10).
DISCUSSION
The goal of this study was to confirm the capability of collarless metal-ceramic FPDs to survive the maximum human incisive biting force when the modified collarless copings were applied to their retainers. In the present study, control group A had the greatest fracture strength, as expected. The strength of the 2 mm gap group D was the lowest among them, at a mean failure load of 1562 N.
In Waltimo's study, the mean maximum incising force of anterior teeth was 263 N for men and 243 N for women.11 Kiliaridis et al. reported that physiological maximum incisive biting forces might vary up to 290 N, primarily depended on facial morphology and age.12 All of the failure loads in the present study were much higher than those of reported maximum incisal forces. From these results, it may be suggested that the 2-mm facial porcelain margin group can be used safely in natural teeth if the marginal fit is acceptable, and if it is cemented to prepared teeth without any crack or fracture of the porcelain.
Fabrication methods of collarless metal-ceramic FPD have been developed and improved.5,13-19 Recently, the direct lift technique has become the most popular method because of its simplicity. However, it has a weak point of technique sensitivity. If the direct lift technique were used in the fabrication of FPDs with the modified collarless coping, margin porcelain build-up would be very difficult. As the amount of unsupported porcelain increased, the qualities of the FPDs became less reliable. The most difficult part of the procedure was to complete the porcelain margins of both retainers. If sufficient condensing of margin porcelain powder was not accomplished, cracks or voids could be trapped into the porcelain bulk. Even if direct lift-off was done correctly, the margin porcelain could be deformed toward the inward direction of the retainer during firing schedules. The shape of the melted porcelain could be changed by the shrinkage of the porcelain or by gravity. This phenomenon occurred much more in group C and D, which had a greater bulk of margin porcelain. Before the next margin correction build-up, the technician had to grind and correct the inner portion of the margin porcelain to adapt the FPD on the die, so the internal angle of facial porcelain veneer might become round, and the internal gap might become greater. There were some reports that the internal marginal gap was greater than the external marginal gap in porcelain margin of collarless metal-ceramic crowns.20,21 This phenomenon could have caused the lower fracture strength of the porcelain margin groups.
Usually, porcelain margins were completed after two or three firings of the margin porcelain. In group C and D, one or two more correction firings were needed, so the overall number of firings increased as the bulk of the margin porcelain increased. The increased number of firings could influence the fracture strength of the FPDs in group B, C, and D. Repeated firings might increase the thickness of the metal oxide layer,22 and an increased metal oxide layer could be another cause of lower fracture strength.23
There was a report that 2 mm gap collarless metal-ceramic FPDs that had experienced thermocycling and cyclic loading could withstand the fracture test better than other all-ceramic FPDs.24 In that report, 100% of the collarless metal-ceramic FPD survived a simulation of five years of mastication in the oral environment, whereas the majority of the all-ceramic FPDs failed in the middle of the test. In that study, the fracture strength of the collarless metal-ceramic FPDs was 682 N, which was twice more than the strength of the survived all-ceramic FPDs. Although the experiment was performed on different conditions from the present study, the result of 682 N was much lower than the failure load of 1562 N in group D. The strength of ceramic restorations definitely decreased after thermo cycling and cyclic loading. However, the in vitro simulation of incisal function in the anterior segment is quite difficult because there are two kinds of teeth contact in the anterior region, incisal guidances and incisal tearing. It is very difficult to simulate all of these loading conditions.25 This was one of the reasons that our study did not select a preload condition. However, an investigation of fracture strength without preload itself is also valuable, because of the initial strength effect on the functional strength.
Generally, as the elastic modulus of the die became greater, the fracture strength of the restorations increased.26,27 PBT resin dies had an elastic modulus similar to natural teeth, and was stronger than common resin because it was reinforced by glass fiber. The resin die could be duplicated with identical size, and could endure the load during the fracture strength test without being fractured itself. Those were the reason that PBT resin was selected as die material.
There were several studies that showed the effect of resin cement on an all-ceramic crown.25,28,29 Yoshinari and Derand reported that the fracture strength of ceramic crowns was greater with resin cement than with zinc phosphate cement or glass ionomer cement.28 The intention of using resin cement in the present study was to improve the strength of the facial unsupported porcelain. The etching and silanation of the porcelain and the etching and bonding of the tooth could make it possible for the margin porcelain to be strongly bonded to the tooth, like a porcelain laminate veneer. When the veneer of the margin porcelain was under load, the bonded margin porcelain could resist more powerfully. If this works in a clinical situation, dentists should use resin cement in luting collarless metal-ceramic FPDs. Stangel et al. reported the ability of resin cement in bonding to porcelain. If the feldspathic porcelain was fluoric acid etched and silanated, the bonding strength increased to six times the original strength. If it was acid etched only, the bonding strength increased 3.5 fold.30
Tuntiprawn and Wilson reported that the fracture strength of all-ceramic crown decreases as the cement thickness increases.31 When a loading force was applied, the greater cement thickness allowed the porcelain to deform more into the cement, and therefore less force was needed to achieve the fracture strain of the porcelain. Another explanation was that the thicker the cement is, the thinner the crown become. And then the thin portion of crown could be fractured easily. In the collarless metal-ceramic restoration, the facial margin porcelain can be comparable to all-ceramic crowns. The faciocervical part of it consists of porcelain only, and the inner marginal gap is usually greater than the external marginal gap. In this region, increased cement thickness would affect the strength of the veneer of margin porcelain as in all-ceramic crowns.
The kind of metal substructures and thickness of connectors could influence the fracture strength. As in all ceramic fixed partial dentures, a higher elastic modulus material and a thicker connector would resist effectively against deformation. To get a higher fracture strength, dentists have to choose base metal and make the connector thicker.
There were two reasons that this fracture test used vertical load. The first reason was that load in vertical direction could influence the facial porcelain margin less than load in other directions. If the specimen received an oblique load, as in a clinical situation, the incisal portion of the pontic, which had a great bulk of porcelain, could be fractured out without the load reaching the facial porcelain margin. The second reason was that vertical load gave more consistent data compared to oblique load.32
Several experiments used loading points that simulated the centric occlusion of the incisor.9,31,33-36 The points were located on the palatal surface 1 - 4 mm below the incisal edge. In this case, the end of the plunger could slide along the palatal surface of the specimen during the loading test, so results showed inconsistent data. In any case, this simulates clenching at centric occlusion, or the contact without posterior teeth. These results could also be meaningful.
About a 1 mm thickness of folded aluminum foil was inserted between the load plunger and the pontic of the specimen. The aluminum foil helped to disperse the load over the incisal edge area. If the flat surface of plunger contacted the incisal edge of pontic directly, the load would be concentrated on one point. The failure pattern might be changed in that situation. The aluminum foil also acted like a food mass, and as a tool that prevented the sliding of the plunger.
There are two kinds of fractures in collarless metal-ceramic restorations. The first is an initial fracture, and the second is a functional fracture. The initial fracture is related to a try-in procedure or cementation. A functional fracture is a fracture sustained after long-term use in the oral environment. The initial fracture is another important factor that dentists must be careful about. Lehner et al. studied the capability of unsupported margin porcelain to resist the initial fracture.7 He reported that 90 degree shoulder porcelain could resist vertical load stress during cementation even if it was unsupported. However, the porcelain could be easily fractured if it was subjected to an oblique load at less than 45 degrees. Initial fracture was related to overly parallel preparation, tooth undercut, and premature contact due to improper impression. If binding with axial walls occurred, seating forces could result in the fracture of the porcelain margin. The tilting of crowns during insertion and removal actions could result in similar failures.
The deformation of the crown during cementation due to increased internal pressure could be another cause of initial fracture. After cementation without fracture, crowns had residual stress due to the contact between crown and tooth. The residual stress could cause a delayed fracture of the porcelain margin. To avoid these situations, sufficient thickness of a crown, passive fit, die spacing, low viscosity cement, and lower seating forces are needed.37 Another recommendation is slower seating speed. Because porcelain margins have no flexibility, fast seating evokes the fracture of a stiff unsupported porcelain margin by increased internal pressure. Exact teeth preparation and impression, proper cementation and adaptation are also needed to avoid unwanted porcelain fracture.
In conclusion, modified collarless metal-ceramic FPDs have several factors that decrease their fracture strength, including increased firings, trapped cracks or porosity in margin porcelain, increased internal marginal gap, and loss of ferrule effect. The strength of collarless metal-ceramic FPDs will decrease in an oral environment with time, but the most important point is that they could survive longer than any other esthetic systems.
CONCLUSION
Within the limitations of this in vitro study, the following conclusions were drawn:
Collarless metal-ceramic FPD groups had lower fracture strength than metal collared control group (P < .05).
The greater the bulk of unsupported facial shoulder porcelain was, the lower the fracture strength became. However, there were no significant differences between experimental groups (P > .05).
All the groups of collarless metal-ceramic FPDs had higher fracture strength than maximum incisive biting force.
The amount of porcelain bulk fractured from the retainers was greater in group C and D than in group A and B. The retainers of group C and D did not resist the vertical load effectively compared to those of group A and B.










 XML Download
XML Download