

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The frequency of esthetic restoration in prosthodontics has been increasing due to increased interest in esthetics. Due to this trend, there has been increasing clinical application of the all-ceramic crown, which is more esthetic and bio-friendly, whereas there has been decreasing clinical application of the metal ceramic crown, which is less esthetic due to the metal coping. As the all-ceramic crown has relatively higher embrittlement and lower tensile strength, its application has been particularly limited to fixed partial dentures.1-4
To improve the embrittlement and lower tensile strength, reinforced dental porcelain was developed using aluminum oxide, leucite, lithium disilicate, and zirconia (zirconium oxide), and all-ceramic restoration has been applied not only to single tooth replacement, but also to fixed partial dentures.5,6
In particular, the latest developed zirconia has a polymorphic structure with chemical stability and volume stability, and suppresses crack progression via the volume extension caused by the transformation toughening mechanism that occurs during the phase transition. Due to these properties, zirconia has higher deflection and fracture strength than conventional dental porcelains, which is why its clinical use has been increasing.7,8
A zirconia full-coverage crown without veneering dental porcelain was recently released (Zirkonzahn prettau; Zirkonzahn GmbH, Bruneck, Italy). The zirconia full-coverage crown without veneering dental porcelain has advantages in that no dental porcelain is fractured due to the absence of an upper structure in it, and more strength can be obtained even in the case of less abutment removal using zirconia with strong hardness to manufacture the crown, compared to previous all-ceramic crowns. On the other hand, the zirconia full-coverage crown has the disadvantage of the abrasion of the opposing natural tooth upon the formation of the occlusal surface with zirconia. No study on the abrasion of the antagonistic natural tooth by zirconia has been conducted so far, though.
Accordingly, this study was conducted to evaluate the clinical validity of the zirconia full-coverage crown by comparing zirconia's wear capacity over an antagonistic tooth with that of feldspathic dental porcelain.
MATERIALS AND METHODS
A. Materials
Zirkonzahn prettau® (Zirkonzahn GmbH, Bruneck, Italy) and feldspathic dental porcelain [Vita Omega 900® (Vita Zahnfabrik, Bad Säckingen, Germany)] were used for the present study testing antagonistic tooth wear. Maxillary premolars extracted for orthodontic purpose were used as antagonistic teeth (Table 1).
B. Methods
1. Preparation of the specimens
The dental specimens were produced by embedding the premolars that were recently extracted for orthodontic demands. The teeth were embedded in acrylic resin mould with only the buccal cusp exposed. The teeth with worn-out cusps or too sharp or fractured teeth were excluded from the subjects.9
2. Preparation of the dental porcelain specimens
The dental porcelain specimens, the control group, were produced into a cuboid with a width of 20 mm, a breadth of 10 mm, and a height of 5 mm, according to the manufacturer's manual; then the specimen surface was ground finished with 1200-grit silicone carbide abrasive under water cooling. These specimens were designated as Group 1.
3. Preparation of the zirconia specimens
The zirconia specimens underwent plasticity and were then produced into cuboids with a width of 20 mm, a breadth of 10 mm, and a height of 5 mm, according to the manufacturer's manual. After the specimen's surface was ground with a sheet of 1,200-grit abrasive paper, it was designated as Group 2. The polished specimens that underwent glazing were additionally designated as Group 3.
4. Wear testing machine
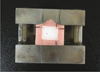
A wear test was conducted using the chewing simulator CS-4.8 (SD Mechatronik, Feldkirchen-Westerham, Germany) which has eight chambers simulating the vertical and horizontal movements simultaneously in the thermodynamic condition. Each of the chambers consists of an upper sample holder that can fasten the specimen with a screw and a lower plastic sample holder in which the specimen can be embedded (Fig. 1).
5. Wear test
A weight of 5 kg, which is comparable to 49 N of chewing force,10,11 was exerted. According to previous studies, as 240,000 - 250,000 loading cycles in a chewing simulator are comparable to approximately one-year chewing from a clinical perspective,12-14 the wear test was repeated 240,000 times to clinically simulate the one-year chewing condition, accompanying thermocycling (Table 2). The three-dimensional (3D) surfaces before and after the wear test were scanned using a 3D profiling system (MTS System Corporation, Eden Prairie, MN, USA), and the actual volume loss of the specimens was calculated with a computer by overlapping the 3D surfaces before and after the wear test using a 3D software (ANSUR 3D, University of Minnesota, Minneapolis, MN, USA).
RESULTS
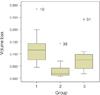
The degrees of wear of the antagonistic teeth based on the restorative materials were 0.119 ± 0.059 mm3 (the greatest degree in the group where Vita Omega 900® dental porcelain was polished with a sheet of 1,200-grit abrasive paper), 0.078 ± 0.063 mm3 (the second greatest degree in the group that underwent glazing of Zirkonzahn prettau® according to the manufacturer's manual), and 0.031 ± 0.033 mm3 (the lowest degree in the group where Zirkonzahn prettau® was polished with a sheet of 1,200-grit abrasive paper (Fig. 4).
The one-way ANOVA showed a statistically significant difference among the groups, and the results of the Tukey test are presented in Table 3.
The degree of wear of the antagonistic teeth based on the restorative materials was four times higher in the group wherein Vita Omega 900® dental porcelain was polished with a sheet of 1,200-grit abrasive paper than in the group wherein Zirkonzahn prettau® was polished with a sheet of 1,200-grit abrasive paper, and they showed a statistically significant difference. The degree of wear of the antagonistic teeth based on the restorative materials was two times higher in the group that underwent glazing of Zirkonzahn prettau® according to the manufacturer's manual than in the group wherein Zirkonzahn prettau® was polished with a sheet of 1,200-grit abrasive paper, and they showed no statistically significant difference. The degree of wear of the antagonistic teeth based on the restorative materials was two times higher in the group wherein Vita Omega 900® dental porcelain was polished with a sheet of 1,200-grit abrasive paper than in the group that underwent glazing of Zirkonzahn prettau® according to the manufacturer's manual, and they showed no statistically significant difference.
DISCUSSION
Dental wear is defined as tooth loss or surface damage caused by direct contact between teeth or between teeth and other materials. Dental wear, one of the physiological phenomena that are experienced in a lifetime, occurs as a complex form of chemical and mechanical wear.15
Dental wear of natural teeth is considered normal. If restorative dental materials have different wear properties compared to the natural teeth, however, they can change the wear rate of antagonistic natural teeth.16 In particular, excessive wear on the occlusal surface can cause an abnormal load and result in periodontal diseases, and can also cause temporomandibular disorders due to the vertical dimension, loss of centric occlusion, diagonal teeth, functional route change during chewing, or masticatory muscle fatigue.17,19,20 Therefore, wear that occurs between the enamel of teeth and restorations is a very important factor that should be considered in the selection of restorative materials in clinical practice. Seghi suggested that a restorative dental material should have a wear degree similar to that of the enamel.21
Dental porcelain was introduced approximately 100 years ago, and has been used for more natural and esthetic restorations. It has a few disadvantages, such as dental porcelain fracture and excessive wear of antagonistic teeth.22
Zirconia has a polymorphic structure with chemical stability and volume stability, and suppresses crack progression via the volume extension caused by the transformation toughening mechanism that occurs during the phase transition. Due to these properties, zirconia has higher deflection and fracture strength than conventional dental porcelains, which is why its clinical use is increasing.7,8 The zirconia full-coverage crown (Zirkonzahn prettau®) was recently released. This product has a few improved characteristics such as greater transparency than that of the previous zirconia, a color liquid that can express the dentin's color tone, and a stain that can be directly applied to the zirconia. In addition, the zirconia full-coverage crown has advantages in that no dental porcelain is fractured due to the absence of an upper structure, and more strength can be obtained even in the case of less abutment removal using zirconia with strong hardness to manufacture the crown compared to previous all-ceramic crowns.
The surface hardness and friction coefficient are commonly used to estimate the degree of wear of restorative dental materials. Conventionally, greater hardness has been believed to cause more wear. Therefore, more wear was expected from zirconia, as zirconia has strong surface hardness. According to scientific studies, however, there is no significant correlation between the restoration hardness and the degree of wear of antagonistic teeth. On the other hand, the degree of wear is more affected by the surface structure and the roughness of the restorations or environmental factors.24
A wear test was conducted to investigate the degree of wear of antagonistic teeth with zirconia using a dual-axis chewing simulator. Compared to previous wear tests, the vertical and horizontal movements were more accurately simulated with a computer, the degrees of wear were more accurately compared using volume rather than height, and the condition of the oral cavity was more realistically simulated with the accompanying thermocycling.25
According to a previous study led by DeLong et al.17 on dental wear caused by dental porcelain, 300,000 chewing cycles showed a volume decrease of 0.162 ± 0.057 mm3. That result is significantly correlated to this study's resulting in volume decrease of 0.119 ± 0.059 mm3 in 240,000 chewing cycles with feldspathic dental porcelain. In this study, the degree of wear of the antagonistic teeth was much lower in zirconia than in dental porcelain. This is likely to be attributable to the fact that zirconia is harder but softer than dental porcelain. More wear was shown in the polished zirconia group with glazing than in the polished zirconia group. This result is likely to be attributable to the fact that porcelain composite was added in the glazing process. Therefore, the polished zirconia full-coverage crown without glazing is more effective in reducing antagonistic teeth wear.
Wear in the oral cavity can be classified into two-bodied wear and three-bodied wear.18 Two-bodied wear is wear in the condition of the saliva alone, whereas three-bodied wear is wear in the condition of other mediators such as food and paste, besides saliva.18 This study measured two-bodied wear, with the limitation that the complex wear phenomena were not fully simulated. Therefore, long-term clinical follow-up will be required for the zirconia full-coverage crown. In addition, a study on the effect of zirconia weakness caused by tetragonal change due to chewing force or water based on direct zirconia exposure upon clinical application of zirconia will also be required.
CONCLUSION
Despite the limitations of this study on the evaluation of antagonistic teeth wear, less wear of antagonistic teeth was shown with zirconia than with the previous feldspathic dental porcelain. As for the zirconia surface process, the degree of wear of the antagonistic teeth was less in the polished zirconia group than in the polished zirconia group with glazing, but no statistically significant difference was found. It is likely that the polished zirconia full-coverage crown without glazing is more effective in reducing antagonistic teeth wear.





 XML Download
XML Download