

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Computer-aided design and computer-aided manufacturing (CAD/CAM) technologies were introduced to the dental profession in 1971 as “Optical Impressions”.1 After continuous development, CAD/CAM was applied to prostheses and orthodontics in the 1980s. CEREC (Sirona Dental System GMBH, Bensheim, Germany) was the first intraoral scanner to be commercialized in the dental market.23 Since then, a number of manufacturers have developed intraoral scanners with various performance properties for creating digital images: Lava COS (3M ESPE, Seefeld, Germany, 2006), iTero (Align Technologies, San Jose, CA, 2007), E4D (D4D Technologies, Richardson, TX, 2008), CEREC AC (Sirona, Bensheim, Germany, 2009), TRIOS (3shape, Copenhagen, Denmark, 2010), and CS 3500 (Carestream Health, NY, USA).4
Functional evaluation of the Lava COS and iTero scanners had been performed by several groups.567 However, there are limited studies regarding the accuracy of TRIOS and CS 3500 because the two intraoral scanners were launched more recently into the dental market compared to the other models in this study.
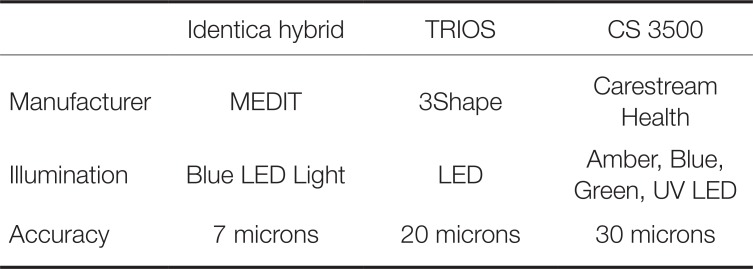
According to the specifications from the manufacturer, the TRIOS scanner is based on confocal laser scanning microscopy with 20 microns accuracy.8 The CS3500 was available with the still image stitching principle with an average precision of 30 microns.9 Comparing these two scanners to the study that evaluated 6 intraoral scanners, the TRIOS and CS 3500 models revealed 6 - 9 µm deviations, whereas the iTero and CEREC Omnicam scanners exhibited 30 - 40 µm deviations, indicating a difference between the intraoral scanners.1011
In a previous study that compared in vivo (intraoral) and in vitro (extraoral) scanning methods, the in vivo method exhibited twice as many 50 µm mean deviations as the in vitro method. This may be due to factors such as intraoral humidity, patient movement, and limited intraoral spaces.6
Few studies have focused on the accuracy of intraoral scanners since intraoral environments were excluded in the in vitro setting. Therefore, the intraoral simulator was required, designed, and developed to assess the accuracy of intraoral scanners by in vitro methods.712 We aimed to evaluate the precision and trueness of TRIOS and CS 3500 scanners and to determine the influence of intraoral environment on scanner accuracy.
Go to : 
MATERIALS AND METHODS
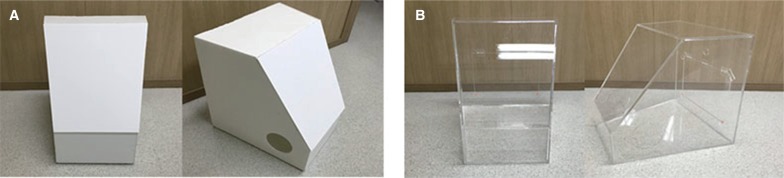
To simulate two environmental conditions, an intraoral simulator was created with an ergonomic design and size (50 × 50 × 50 cm). A pre-production model with 5-mm foam boards was created as a full-scale mock up to determine whether there were issues in simulating the two environmental levels (Fig. 1A). The final intraoral environment simulator was produced with 5-mm acrylic boards (Fig. 1B). In the final structure, the intraoral simulator, unlike the normal boxes, had a narrower front than back, designed to be more comfortable for clinicians who performed scans inside the simulator. A wide front surface would not block the clinician's view during scanning. Through a small door at the backside, experimental objects were passed into the simulator. Also, the access of the clinician's hands to the inside of the device was performed through detachable waterproof sleeve gloves. Additional lids could block unnecessary holes depending on the situation.
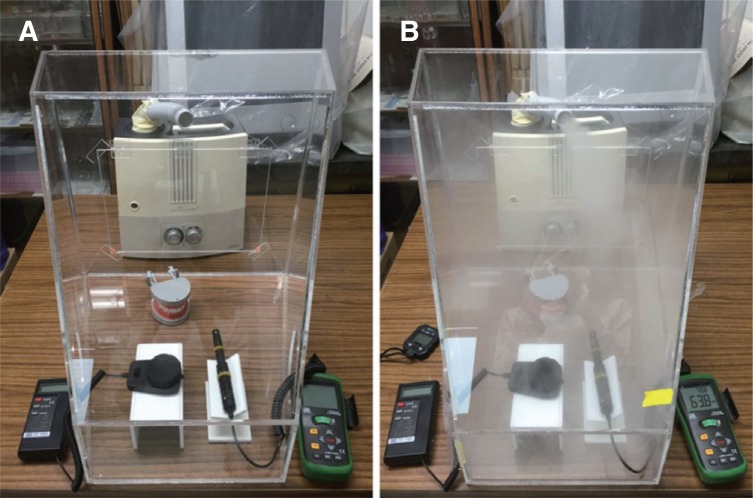
Necessary devices such as a humidifier, an alcohol lamp, a thermos- hygrometer, and an illuminometer were placed in the simulator to create two fixed intraoral environments (Fig. 2A). After that, all of the environmental conditions were established (Fig. 2B).
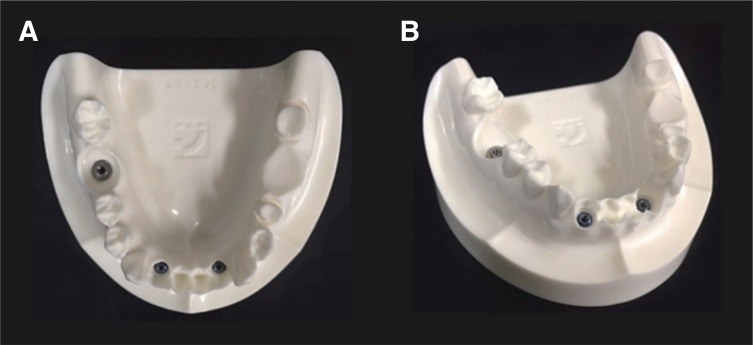
The reference model was used in this study was replicated with two clinical scenarios using a low-viscosity liquid photopolymer (DSM's Somos GP Plus 14.122). The model was produced with water-resistant, durable, and accurate three-dimensional functions. The two clinical scenarios were fabricated with implant abutments and prepared teeth: (1) both lateral incisors (#32, #42) and the right first molar (#46) were placed with US II external fixtures (Osstem Implant Co., Ltd., Seoul, Korea) with a size of 4.0 × 10 mm, (2) the left first premolar and second molar (#35, #37) were used for a fixed bridge (Fig. 3). In this way, all of the five teeth were scanned.
The average intraoral temperature was determined to be between 30 and 35℃, and relative humidity (RH) ranged between 80% and greater than 95% RH in the Yoshida13 and Spierings14 studies, respectively.
In this study, the temperature (℃), relative humidity (%), and illumination (Lux) were chosen as the intraoral environmental factors. The three factors were measured five times per person for five people in order to determine the reference values of the three intraoral factors before scanning.
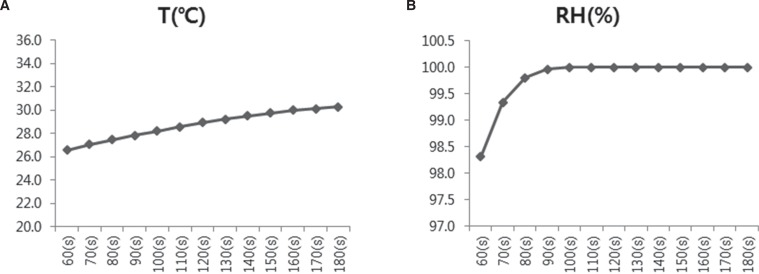
The factors were measured and divided into both anterior and posterior sides. However, the anterior part was excluded because there was no difference with the ambient environmental conditions. A probe from a thermoshygrometer and an illuminometer were inserted inside the center of the oral cavity, and the values were measured over time, 10 seconds each for five times per person. The consistent part of this graph of temperature and humidity was exhibited from 60 to 180 seconds. A maximum temperature greater than 30℃ was achieved at 180 seconds, and the humidity was maintained at a constant value of 100% RH from 90 seconds (Fig. 4). Next, the average values of oral temperature, relative humidity, and illumination were calculated and finally classified into two groups (Table 1).
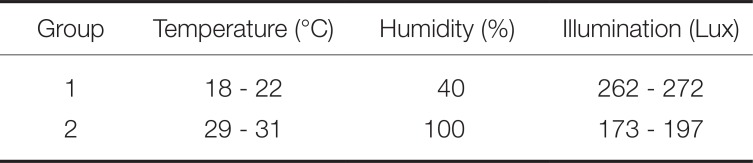
Group 1 was an ambient room condition with 18 - 22℃/40% RH/ 262 - 272 Lux. Group 2 had higher maximum temperature, humidity, and lower illumination than Group 1: 29 - 31℃/100% RH/ 173 - 197 Lux. Group 2 simulated molars with maximum intraoral conditions.
The laboratory reference scanner Identica Hybrid (MEDIT, Seoul, Korea) and two intraoral scanners, TRIOS (3Shape, Copenhagen, Denmark) and CS 3500 (Carestream Health, Rochester, NY, USA), were selected for use in this study (Table 2).
The observer (H.-N.P.) was trained in use of the reference model in order to minimize the difference due to inexperience with the intraoral scanners.
First, the reference cast was scanned 10 times automatically by the Identica hybrid while repeatedly maintaining the ambient laboratory conditions like Group 1 temperature, humidity, and illumination (Table 1). Then, the observer scanned the same cast 10 times using TRIOS and CS 3500 scanners for each of the two simulated groups. After scanning with the Identica, TRIOS, and CS 3500, all data of the virtual 3D models were exported into Standard Tesselation Language (STL; 3D systems, Rock Hill, SC, USA) files.
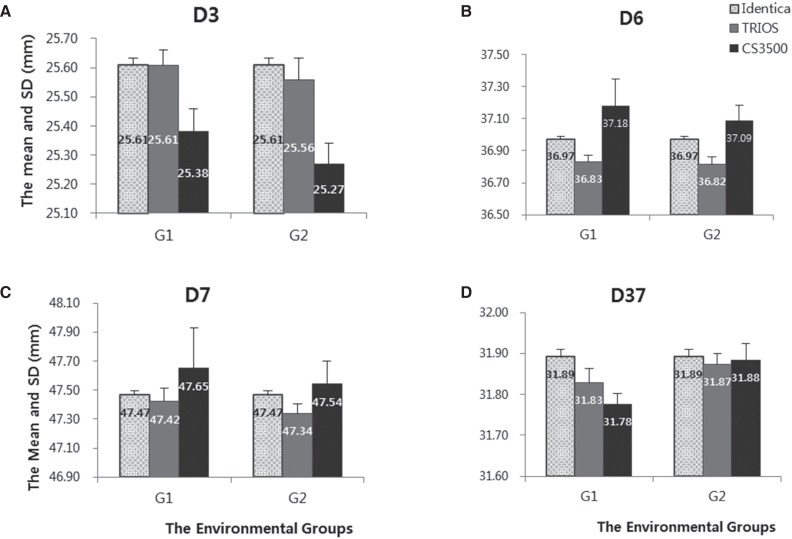
The parameters to objectively compare the 3D models from the different scanners were the measurements of distance between teeth.15 Referring to the parameters, four measurements were chosen in this study: the distances between the canines (D3), between the first molars (D6), between the second molars (D7), and between the right canine and second molar (D37) (Fig. 5).
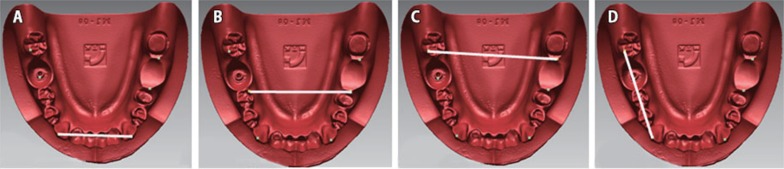
Before measuring the distances between teeth, all 3D models were aligned to the same location using Rapidform 2004 software (INUS Technology, Seoul, Korea). In order to measure the distance, the all reference points of the highest points on the cusp tips were marked on the 3D images by an automatic marking function in Rapidform 2004 program. However, both sides of the first molars (#36, #46) and of the left second molar (#47) were eliminated to simulate the presence of implants. Hence, the reference points were marked on the implants instead of on the cusps. Distances were measured between the reference points.
Statistical analysis was carried out using Statistical Software (IBM SPSS Statistics 23, SPSS Inc., Chicago, IL, USA). The Kruskal-Wallis test was used to compare the two intraoral scanners and environmental groups. P < .05 was considered statistically significant. The mean and standard deviation of the measured distances were calculated to assess the reproducibility of the scan results.
Go to :
RESULTS
The correlations between the accuracy (reproducibility and trueness) of single intraoral scanners and environmental factors were assessed. The differences in Group 1 (G1) and Group 2 (G2) are shown in Table 3. There were no statistically significant differences between the scanners with different environments.

Table 3
The mean and SD of two intraoral scanners following the environmental groups (G1, G2)
![]()
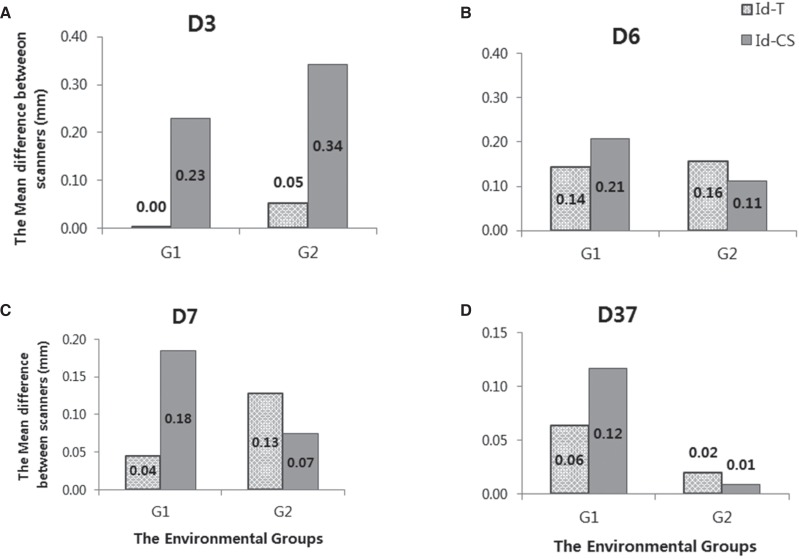
The mean differences between the Identica hybrid and the two intraoral scanners were assessed by a digital measurement of the two highest points to compare the trueness according to scanner. The findings ranged from 0.00 to 0.34 mm for the differences in all distances. There were significant differences between D3 and D6 (Fig. 6). In the standard deviations (SD) of the scanners to assess the reproducibility, the SD of the Identica scanner was the lowest of the scanners. The standard deviations of the TRIOS and CS 3500 scanners followed in order (Fig. 7).
Go to :
DISCUSSION
In this study, the accuracy (reproducibility and trueness) of scanning was determined using intraoral scanners and environmental factors. No studies of the accuracy of intraoral scanners have been conducted with consideration of intraoral environment.
A chamber to simulate intraoral conditions was used in other studies to investigate dentin bond strength16 or microleakage of adhesive systems.17 However, the chamber used in this study was limited to experiments of intraoral scanners. This study has significance for the development of environment simulators that can reproduce environmental variables. Therefore, an intraoral simulator specializing in evaluating accuracy was developed. The simulator had an ergonomic design for increased comfort for the user, portability, and for safety of the intraoral scanners. In addition, the simulator was able to create all degrees of humidity, temperature, and illumination.
In other studies, deviations of scanning were compared with 3D evaluation software that superimposed all scanned digital data18 and measurements of the distance between teeth.19 The experimental method we used to assess the accuracy was to compare intraoral scanners from two different manufacturers.12 CEREC, Lava C.O.S, and iTero scanners were used frequently in most of the previous studies720; however, there have been limited investigations evaluating the accuracy of the two newest intraoral scanners, TRIOS and CS 3500. Therefore, these two intraoral scanners were chosen for measuring teeth distances in simulated intraoral environments in this study.
No statistically significant differences in the reproducibility of the scanners were revealed following exposure to environmental factors. This indicated that the TRIOS and CS 3500 scanners can be classified as intraoral scanners that are not sensitive to different environmental conditions. We assumed that intraoral environmental factors did not greatly affect the reproducibility. The higher deviations were caused by limited intraoral spaces and patient movements versus intraoral environmental factors, as shown in a previous study.6
A comparison of the intraoral scanners showed statistically significant differences. The distances between the right and left canines (D3) and between the right and left first molars (D6) exhibited statistically significant differences. For the differences between the reference value of Identica and the two intraoral scanners, the Identica hybrid was assigned to a reference value because the model scanner had a higher accuracy than the intraoral scanners. Identica was one of the latest products introduced into the dental market and produces the highest accuracy of less than 7 µm for digital scanning. Moreover, this instrument was based on the principle of phase-shifting optical triangulation and a three-camera method with color scanning.21 In the post-hoc test on D3, Identica and TRIOS had similar accuracy findings that were different from those of the CS 3500 scanner. Furthermore, this mean difference might be related to the difference between the reference values of Identica to TRIOS to show the trueness, which ranged from 0.00 to 0.14 mm, and to CS 3500, in the range of 0.01 - 0.34 mm. In a previous study, TRIOS had deviations that ranged from 4.5 - 6.9 µm, whereas CS 3500 had deviations range of 7.2 - 9.8 µm.10 Consequently, it was assumed that the TRIOS scanner was relatively more accurate than the CS 3500 scanner.
One of factors in the difference of the trueness between the TRIOS and CS 3500 scanners could be attributed to scanning principles. TRIOS is a video scanner, while CS 3500 is a still image scanner.8 The result of a prior experiment showed that an intraoral video scanner (CEREC Omnicam) had a lower deviation than an intraoral still image scanner (CEREC Bluecam).22
The SD of each scanner was calculated to determine the reproducibility. The SD of Identica ranged from 0.04 - 0.05 mm, TRIOS from 0.05 - 0.17 mm, and CS 3500 from 0.05 - 0.55 mm. Identica had the highest reproducibility compared to TRIOS and CS 3500. Compared with CS 3500, TRIOS showed better reproducibility. In detail, when the SDs of teeth distance were analyzed, that of CS 3500 was higher from D3, D6 compared to the other scanners. In addition, the result of the post-hoc test on D6 trueness revealed that the trueness of the CS 3500 was similar to that of the Identica, which contrasts with the pattern shown in the D3 post-hoc test. This opposing phenomenon was attributed to the model used in this study, which was made with prosthetic implants.23 Like the experimental models,2324 our reference model was created with implants and prepared teeth. The models were classified into five different scenarios before the experiment assessed the accuracy of TRIOS. Consequently, the parts on commonly prepared teeth or missing teeth were shown with higher deviations. Despite performance by a single experimenter in the study, the movement of the scanner tip between scanning procedures influenced the integration of the 2D pictures.
This experiment evaluated the accuracy (reproducibility and trueness) of the latest scanners of TRIOS and CS 3500 through an environmental simulator. Many manufacturers will develop various types of more accurate intraoral scanners in the future. In summary, the differences in the performance of scanners were higher without taking environmental effects into consideration. Therefore, the final purpose of this study was to accumulate a number of indicators of accuracy using the developed intraoral environment simulator.
Go to :
CONCLUSION
This study investigated the relationships between the accuracy and influence of environmental factors using an intraoral environment simulator. In the comparison between intra-oral scanners, TRIOS had similar accuracy and reproducibility with Identica. Although a subtle difference of trueness based on the type of scanners existed, no significant differences were exhibited from the intraoral environments.
Within the limits of the present study, the intraoral simulator that was developed will assist in developing intraoral scanners with higher accuracy.
Go to :
 XML Download
XML Download