

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since 1965 when Brånemark et al.1 introduced and established the osseointegration concept, dental implant has achieved enormous development and progress. Defined as direct connection between bone and implant surface, osseointegration is formed by the process of bone formation between bone and implant surface. Because the success and failure of implant is determined by osseointegration, it is a precondition for prosthetic repair through implant. Implant stability can be divided into primary stability and secondary stability. The primary stability is obtained by mechanical fixation of the implant with bone, and this is one of the basic conditions for osseointegration.2 Primary stability is related with implant surface area, geometry, length, contact area between implant and bone. Other factors include ratio of spongy bone vs. cortical bone, and implant technique.3 The secondary stability is generated secondarily by bone formation and bone remodeling in the process of osseointegration due to biological fixation in the interface between bone and implant.4 Therefore, we can evaluate the degree of osseointegration through the measurement of changes in the implant stability.5 Meredith et al. reported on the use of the resonance frequency analyzer to evaluate the stability of implant, and demonstrated the ability of the device to evaluate the changes in stiffness of the interface in the early in vitro experiment.6,7 Recently, histomorphologic studies suggested that the resonance frequency value has a high correlation with the level of contact between bone and implant.8-11 This discovery supports the use of resonance frequency analysis to evaluate the changes in the process of osseointegration and bone healing after placement of implant. The resonance frequency analyzer can measure clinically and noninvasively the stability of implant and estimate the degree of osseointegration. In this study, we used a recently developed magnetic resonance frequency analyzer to measure the stability of implant. For measurement unit, implant stability quotient (ISQ) is used which is recorded as a number between 1 and 100 with 100 representing the highest stability.12
This study intends to measure and analyze the changes in implant stability without load during an early healing period of six months after placement of three different types of implants by one stage implant. In this way, this study will provide useful information for prosthetic treatment planning through immediate and early loading after placement of implant as well as the evaluation of long-term prognosis for it.
MATERIAL AND METHODS
A total of 28 patients (25 males and 3 females, mean age: 58.6 ± 9.23) were selected among the patients who visited between March and September 2004 with the main purpose of implant placement.
Inclusion criteria were as follows
Adults aged 18 or older
Patients who understand and agree to this study
Adequate oral hygiene (1 or lower mean modified sulcus bleeding index, 1 or lower mean modified plaque index)
Sufficient bone volume to place the planned implant
One or more edentulous mandible parts which are six months or longer after dental extraction (however, adjacent teeth must be healthy and properly repaired)
Fertile women who received pregnancy test no later than one week before surgery and have been confirmed to be negative
Exclusion criteria were as follows
The three types of 45 implants were divided into 3 groups including Osseospeed® (Group A, Astra Tech, Sweden), Camlog® (Group C, Biotechnologies AG, Switzerland), and Replace® (Group R, NobelBiocare, Sweden) in this study. The numbers of implant systems placed are as follows (Table I).
One assigned operator placed implants by one stage technique in accordance with the surgical protocol suggested by the manufacturer. Bone quality classification followed the criteria proposed by Lekholm & Zarb, and Type 1, 2, 3 or 4 was determined on the basis of the sense of resistance during bone drilling. The implants were placed by manual torque wrench. After placement, ISQ was measured, a healing abutment was connected, and sutured.
For Magnetic Resonance Frequency Analyzer, this study used Osstell™ (Göteborg, Sweden). A special smart peg was connected to the implant body at 4 - 5 N/cm torque, and measurements were made at 2 - 3 mm away so that the probe tip of the analyzer would point to the small magnet above the smart peg (Fig. 1). Measurements were made at two directions to measure the highest and lowest stability directions. Measurements were made three times for each direction to ensure reproducibility. The two directions are buccolingual and mesiodistal directions (Fig. 1). If the probe measures two values simultaneously and the difference between these two values is 3 ISQ or higher, the values must be indicated simultaneously. However, it did not happen in this experiment. ISQ was measured immediately after placement, after 3 weeks, 6 weeks, 8 weeks, 10 weeks, 12 weeks and 24 weeks. In addition, we examined the existence of discomfort at the time of healing abutment removal and the smart peg connection. No implant received immediate or early loads. The data were analyzed by implant type, bone type, healing time, and location.
Statistical Analysi
The data were recorded as implant ISQ over time, and were analyzed by implant type, bone type, healing time, and location. For the analysis by bone type, interaction between time and type with two-factor effect mixed model was used. Here, the comparison between the time points used contrast comparison in the two-factor effect mixed model. For comparison of bone types at different time points, the multi-comparisons of ANOVA and Tukey were used (P = .05). The analysis by mandible location used the time effect with two-factor effect mixed model and the location effect with two-factor effect mixed model.
RESULTS
The surgeries produced no complications in all the patients and the ISQ numbers were obtained without causing inconvenience to the patients. Every ISQ showed high reproducibility. Bone types 2 and 3 were grouped together, because recent papers demonstrated that it was difficult to reliably differentiate the drilling resistance in intermediate bone. 45 implants were placed in total and none of them failed. The placed implants are as follows (Table II).
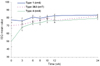
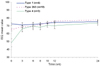
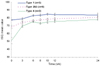
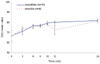
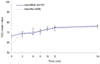
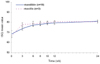
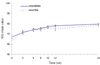
The two-factor mixed model ANOVA was used to determine the existence of interaction between bone type and time in Groups A, C and R (P = .0022, P = .017, P = .0018). In other words, the change patterns of ISQ by time were different by bone type (Figs. 2, 3, 4). Furthermore, the ISQ values of bone types were compared through multi-comparisons of ANOVA and Tukey. In the groups A, C and R, the measurements immediately after placement showed statistical differences in bone types 1, bone types 2 & 3, and bone type 4 (P < .05). The mean ISQ of implants immediately after placement was over 70 in the bone type 1, between 65 and 70 in the bone type 2 & 3, and between 48 and 50 in the bone type 4 (Figs. 5, 6, 7, 8).
In Group A, between week 0 and 6, ISQ increased 4.78% in bone type 1, 8.73% in bone type 2 & 3, and 56.47% in bone type 4. The three bone types showed slow increase between six weeks and six months. The bone type 1 did not show significant change (P = .052), while bone types 2, 3 and 4 showed significant changes (P = .044, P = .0326).
In Group C, between week 0 and 6, ISQ increased 0.52% in bone type 1, 6.38% in bone type 2 & 3, and 49.11% in bone type 4. The bone type 1, 2 & 3 showed slow increase between six weeks and six months. The bone types 1, 2 & 3 showed significant changes (P = .0356, P < .0001), but type 4 did not show significant changes (P = .3715).
In Group R, between week 0 and 6, ISQ increased 7.37% in bone type 1, 11.87% in bone type 2 & 3, and 47.81% in bone type 4. The three bone types showed slow increase between six weeks and six months. The bone types 1 did not show significant changes (P = .6411), but type 4 showed significant changes (P = .0005, P = .0462).
Implant Stability by Location
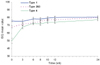
According to the two-factor mixed model, Groups A and C did not show significant differences in stability changes by healing time according to the anatomical location between maxilla and mandible. In Group R, the change of stability by healing time showed significant difference between maxilla and mandible (P = .0238). However, the comparison between maxilla and mandible by the two-sample t-test did not find significant difference among 3 groups (Figs. 9, 10, 11, 12).
DISCUSSION
The need for clinical diagnosis tools with high accuracy to recognize the stability of implant and early healing changes is increasing along with the immediate and early load concept. The resonance frequency device invented by Meredith4 has been used for clinical reference of the stability of implant placed in various bone types.
There are several reports about implant stability influenced by healing time.8,10,11 This study also found through an analysis with the interaction between time and type with two-factor effect mixed model that the interaction of time and bone quality had significant influence on the ISQ values.
The result of implant stability immediately after placement was bone Type 4 < Type 2 & 3 < Type 1 in all implant groups. The implant stability measured immediately after placement is primary stability resulting from the mechanical press-fitting of implant with a greater diameter than the hole in the bone, and is influenced by the stiffness of adjacent bones.3,4 In other words, the higher the stiffness of adjacent bones, the higher the primary stability. Therefore, the stability immediately after placement of bone type I that has a high volume of cortical bone and a small volume of spongy bone is higher. On the other hand, bone types 2 & 3 and type 4 have a less volume of cortical bone and a more volume of spongy bone, which decreases the stiffness of bones and lowers the stability immediately after placement of implant.13
The three bone types experienced great changes in stability between week 0 and week 6. In an experiment with rabbits, Robert14 reasoned that human bone quality would undergo significant changes between week 0 and week 6 by the formation of woven bone and the deposition of lamellar bone. Furthermore, the size of changes between week 0 and week 6 varied by bone type. The ascending order of the size of changes was bone Type 1 > Type 2 & 3 < Type 4. The cortical healing was slow because it only depends on lamella remodeling. However, the cancellous healing showed was fast because in addition to trabecular remodeling, the bone is close to bone marrow that has a rich vascular system and mesenchymal progenitor cells which can be differentiated into osteoblasts. Therefore, it seems that the closer to bone Type 4, the higher implant stability by the fast regeneration of woven bones.15
The slow increase of implant stability between week 6 and six months (plateau effect) has been reported by Cochran et al.16 This phenomenon has a correlation with the strengthened bone formation concept around the implant. Robert14 believed that the later stage of the deposition of the lamellar bone into the grids in human woven bones and the interface remodeling begins at week 6 and continues until week 18, and the deposition of lamellar bone gives sufficient strength to withstand load. He also stated that bone maturity is completed within 54 weeks.
The changes of stability by healing time according to the mandible location were not significantly different between the upper and lower mandible groups. There are many existing studies that found that the lower mandible shows higher stability.17,18 The result of this study was different, which seems to be due to the small number of samples (There were five cases of bone Type 4 in the 13 maxilla cases).
The implant length may be an important factor that influences ISQ value.19 However, this study could not analyze the differences due to the insufficient number of samples by length.
CONCLUSIONS
Within the limitation of this study, we found that the time/bone quality interaction had significant influence on ISQ values through an analysis among implant groups A, C, and R. In other words, in all the implant groups A, C and R, the change patterns of ISQ over time differed by bone type. Implant stability increased greatly between week 0 and week 6 (order of increase: Type 1 < Type 2 & 3 < Type 4), and showed slow increase between week six and six months (plateau effect). However, no significant difference in stability changes by healing time according to locations was found in all the implant groups.
More studies are required about the mechanotransduction effect during the early implant loading in various implant systems, and the effect of this on the magnetic resonance frequency analyzer during the early healing period.






 XML Download
XML Download