

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary stability at the time of implant placement is related to the level of primary bone contact.1 The level of bone contact with implant is affected by many factors such as thread design, surgical procedure and bone quality. The long-term success for implant therapy unfortunately becomes less certain when fixtures are placed into bone of poor quality and/or quantity. The early loss of dental implants is thought to be due to excessive mechanical loads applied too early to the implant coupled with poor primary stability at placement.2
The most popular method of bone quality assessment is what was developed by Leckholm & Zarb (1985), who introduced a scale of 1 - 4, based on both the radiographic assessment and the sensation of resistance experienced by the surgeon when preparing the fixture site.3 Johansson & Strid (1994) described a technique whereby bone quality as a function of density and hardness could be derived from the torque forces needed during the implant insertion.4 The periotest® values as well reveal the increased stiffness of the implant-bone continuum over time.5 The in vivo experimental findings demonstrate that resonance frequency is related to implant stiffness in the surrounding tissues, which means a higher bone-to- implant contact percentage.6 Also, Removal torque is one of the important factors of the initial fixation of implants.7
In case of type IV bone maxilla with thin cortex, engagement into sinus inferior cortical wall will help to gain higher initial stability. For this, accurate drilling just to the cortical wall is necessary unlikely with window technique or osteotome technique.
Implant stability is also related to thread design. It was reported that thread depth, thread thickness, thread face angle, thread pitch and thread helix angle affect the biomechanical load distribution of the implant.8
The purpose of this study was to compare the initial stability in various taper body implants with various design, some of which were engaged to inferior cortical wall of type IV bone and the rest of which were not engaged to inferior cortical wall by measuring the implant stability quotient (ISQ) and the removal torque value (RTV). Also, the effect of under-drilling on ISQ and RTV was experimented.
MATERIAL AND METHODS
1. Selection of taper implants with the various design
6 different implant fixtures with 10 mm length were selected and installed. Thread designs were different depending on the shape of taper, absence or existence of micro- thread and the shape of thread. They were Hexplant (Warantec, Seoul, South Korea), US III® & GS III® (Osstem, Seoul, South Korea), Replace® Select (Nobel Biocare, Göteborg, Sweden), Osseotite NT® (3i, Florida, USA) and Sinus Quick (Neoplant, Seoul, South Korea). The abbreviation of each implant system was W for Hexplant, US and GS for US III® & GS III®, RS for Replace® Select, NT for Osseotite NT®, SQ for Sinus Quick (Table I, Fig. 1).
2. Specimens preparation
To simulate the sinus inferior wall of type IV bone, one side cortical bone of swine rib was removed (Fig. 2). Six different implants were installed in the same bone block (Fig. 3) following to the manufacturers recommended procedures (Fig. 4). Total 20 bone block were made for each implant system. In Group 1 the height of bone block was 10 mm and fixtures were installed with engaging to inferior cortical wall. The fixtures in Group 2 were installed without engaging to inferior wall and the height of bone blocks was 13 mm (Fig. 2).
3. The measurement of ISQ value
The initial stability was measured with ISQ value using Osstell mentor® at the time of placement (Fig. 5). All measurements were made by one dentist. The RFA device (smartpeg; Integration Diagnostics AB., Gemlestadsvagen, Sweden, Fig. 6) was placed by hand tightening 5 - 10 Ncm onto the implant fixture. ISQ values were measured parallel and perpendicular to the bone (Fig. 7). ISQ values for each fixture were taken as the mean of ISQ values which were taken in the two orientations.
4. Measurement of removal torque
A torque gauge (MGT50) was used to unscrew the implants. The removal torque was defined as the minimum torque needed to completely unscrew the implant and remove it. The torque gauge enabled direct readings of the removal torque of the implant (Fig. 8).
5. Under-drilling of NT system
NT system which had the lowest initial stability in this study was chosen to experiment the effect of under drilling on initial stability. For under-drilling the last step drill was skipped (Fig. 9). Five fixtures were engaged to inferior cortical wall and other five fixtures were not engaged.
6. Statistical analysis
Statistical analysis was performed using SAS 9.1.3 (SAS institute, North Carolina, USA). The influence of engaging on ISQ and removal torque value was analyzed by non-paired T-test (N = 60). One way ANOVA was performed to find out the effect of implant type on ISQ and removal torque value (N = 10). And multiple comparisons of estimated means were adjusted with Bonferroni correction. Under-drilling result was analyzed by Mann-Whitney test (N = 5). The level of significance was set at 5% for all analysis.
RESULTS
In group 1 with engagement, the means of ISQ value and removal torque value were 58.7 ± 8.4 and 19.5 ± 7.7. In group 2 without engagement, 62.9 ± 9.8 and 11.3 ± 6.4 were measured for ISQ value and removal torque. There was a significant difference in RTV and ISQ value depending on engagement to inferior cortical wall (P < .05).
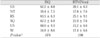
Comparison of ISQ and removal torque value depending on thread designs among Group 1 were shown in Table II and Fig. 10. In group 1 with inferior cortical wall engagement, there was no significant difference in RTV and ISQ value among the six types of implants.
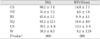
Comparison of ISQ and removal torque depending on thread design among Group 2 were shown in table III and Fig. 11. In group 2 without inferior cortical wall engagement, there was significant difference in RTV and ISQ value among the 6 types of implants (P < .05).
In case of Change of ISQ and removal torque value depending on the reduction of step drilling, ISQ value and removal torque were significantly increased when the last step drilling was skipped in NT system which had the lowest ISQ and removal torque value (P < . 05, Table IV).
DISCUSSION
Threads are used to maximize initial contact, improve initial stability, enlarge implant surface area, and favor dissipation of interfacial stress.9 Thread shapes in dental implant designs include square, V-shaped, and buttress. Under axial loads to a dental implant, a V-thread face is comparable to the buttress thread when the face angle is similar and is usually 30°. The standard V-shaped thread (eg, Paragon/ Calcitek; Centerpulse Dental Inc.; 3i, 3i Implant Innovations Inc.; ITI, The Strauman Co. Waltham, MA; and Nobel Biocare, Nobel Biocare USA Inc.) has 10 times greater shear loads on bone compared with a square thread with parallel major and minor diameters.9
A square thread design has been suggested to reduce the shear component of force by taking the axial load of the prosthesis and transferring a more axial load along the implant body to compress the bone.9 In one study, the overall maxillary success rate is, on average, approximately 3% lower than that of mandible.9 However, the square thread design is the exception with success rates in the maxilla and mandible being equal and also the highest success rates reported.8
A buttress thread shape is optimized for pull-out loads and has parallel major and minor diameter. The reverse butress thread design (eg, Steri-Oss, Steri-Oss Inc. Anaheim, CA) has fewer threads and less thread depth.9
Another recent approach has been the introduction of a rounded thread design that claims to induce "osteocompression".9 A Sinusoidal thread design (eg. LaminOss immediate load implant; Impladent Ltd., Holliswood, NY) has shown, in animal histologic observation, lamellar bone achieved by the function of osteocompression.10
In this study, square thread design did not show higher ISQ value and removal torque value regardless of engagement to inferior cortical wall. It appears because square thread implant is not self-drilling and is supposed to be installed passively into the tapping site. Square thread shape seems to affect positively to long-term success rather than primary stability.
This study also showed statistically higher ISQ value and lower removal torque without engagement. RFA is related mainly to the height of the implant not surrounded by bone, and to the stability of the implant-bone interface.1 Several factors influence on RFA; stiffness of the implant-bone interface, stiffness of the bone itself, stiffness of the implant components.1 ISQ values for successfully osseointegrated implants have been reported to vary from 57 to 82, with a mean of 69 after 1year of loading.11 Some studies show there is correlation between ISQ and implant placement, BIC, thickness of cortical bone, bone quality.12-14 Otherwise, some authors revealed there is no correlation between RFA and loading time, placement torque, morphologic parameters.13,15-17 The RFA does not appear suitable for the evaluation of implant stability when used as a single method.18 In this study there was no correlation between ISQ and removal torque, cortical engagement.
Removal torque value usually is measured to compare degree of osseointegration at several months after installation.19 However, some authors used removal torque value as a parameter of primary stability in human cadaver experiments.2,20,21
This study showed that in group 2 without inferior cortical wall engagement there was a significant difference in ISQ value and removal torque value depending on thread design but not in group 1 with engagement. In group 2 USIII® (trapezoid, without microthread) and GSIII® (V-shape, with microthread) had the highest ISQ value, and NT® (V- shape, without microthread) did the lowest one. As with removal torque value, SQ (buttress, with microthread) and GSIII® (V-shape, with microthread) showed the highest value and NT® (V-shape, without microthread) did the lowest one. It doesn't seem that only one factor such as microthread, or thread shpae, taper shape affects to initial stability. Rather, combination of the above factors is determinant to ISQ and removal torque value. Group 1 with cortical engagement showed that engagement could compensate for difference depending to thread shape.
NT® (V-shape, without micro-thread) showed the lowest value in ISQ value and removal torque value. This system has two step drilling like W system which had the second lowest value. So, when the second step drill was skipped and implant fixture was installed with self tapping effect, ISQ and removal torque value increased significantly. Under-drilling could be helpful to achieve initial stability in poor quality bone.
CONCLUSIONS
1. In group 1 with inferior cortical wall engagement, there was no difference in RTV and ISQ value among the 6 types of implants.
2. In group 2 without inferior cortical wall engagement, there was significant difference in RTV and ISQ value among the 6 types of implants (P < .05).
3. There was significant difference in RTV and ISQ value between group 1 and 2 (P < .05).
4. Under-drilling made RTV and ISQ value increase significantly in case of the implant which had lower RTV and ISQ value without engagement to inferior cortical wall (P < .05).













 XML Download
XML Download