

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Soft tissue esthetics is regarded as a prerequisite for successful implant restorations.1,2 To achieve an esthetic outcome, the level of peri-implant soft tissue should be in harmony with that of adjacent natural teeth as well as the contralateral tooth. Chang and colleagues compared the esthetic outcomes of single implant restoration to those of contralateral natural tooth, and reported that the crowns supported by implants were on the average 1 mm longer than the clinical crown of contralateral natural teeth.3 Fürhauser et al. assessed 7 esthetic variables, which were mesial papilla, distal papilla, soft-tissue level, soft-tissue contour, alveolar process deficiency, soft-tissue color and texture, to evaluate the esthetic outcome of peri-implant soft tissue. The study showed that the soft-tissue level and soft-tissue color variables resulted in poorer esthetic outcome compared to other variables.4
The level of facial gingiva is influenced by several factors such as thickness of labial bony wall, the position of implant shoulder, the orientation of implant, the diameter of implants and the gingival biotypes.1,5-7 The stability of peri-implant soft tissue is also a determinant factor for the level of gingival margin. Grunder investigated the stability of the mucosal topography around single tooth implants. The 1-year results revealed that the soft tissue shrinkage on the buccal side of the implant crown was 0.6 mm on average.8 Small and Tarnow reported that approximately 1 mm of recession occurred on the midbuccal gingiva at 1 year following abutment connection surgery. The major changes took place within the first 3 months.9 Other studies reported that apical displacement of the facial soft tissue margin mainly took place during the first 6 months following insertion of final restorations, with relatively little change afterwards.10,11
Recently, Nozawa and colleagues noticed the width of buccal supra-implant mucosa as a determining factor of the level of buccal marginal gingiva.12 They measured the height and width of the buccal supra-implant mucosa in 14 single implant restorations, and reported that the average biologic height to width ratio was 1 : 1.58. When the width of buccal supra-implant mucosa was less than 1.5 times of the height of mucosa, they recommended horizontal tissue graft to prevent the decrease of mucosal height.
Until now, most of studies about peri-implant mucosal level investigated the level of single implant restorations. No attempt was made to measure the height of buccal supra-implant soft tissue around multiple adjacent implant restorations.
The purpose of current study was to evaluate the width and height of buccal supra-implant soft tissue around single and multiple adjacent implant restorations. The null hypothesis tested was that the number of implants (single or multiple adjacent), as well as the location of the implant (anterior or posterior segment, implant between teeth or the terminal implant) does not influence the width, height and width to height ratio of buccal supra-implant soft tissue.
MATERIAL AND METHODS
Four groups of implant restorations, each group comprised of 6 patients, were randomly chosen from the patients who were treated in Gangnam Severance Dental Hospital, Department of Prosthodontics, from Mar 2005 to Dec 2007. Patients who have any third molar were excluded from this study. All patients were fully understood the treatment procedures and an informed consent was made for each patient.
The 4 groups of patients were as follows.
Group 1: Two adjacent implant restorations, which restored maxillary or mandibular first and second molars. Group 1 was divided into 2 subgroups.
Group 1a: tooth side implant restorations, which replaced the first molars
Group 1b: the terminal implant restorations, which replaced the second molars
Group 2: single implant restorations, which replaced the terminal teeth (second molars)
Group 3: posterior single implant restorations, which were placed between natural teeth.
Group 4: maxillary anterior single implant restorations, which were placed between natural teeth.
Each group was comprised of six implant restorations, therefore, a total of 30 implants were included for the current study. The implant used in current study was Inplant™ (Warantec, Seoul, Korea), which had internal friction fit implant/abutment joint. The diameter of implant platform was 4.3 mm whereas that of implant/abutment junction was 3 mm. The diameter of abutment/restoration junction was 4.5 mm, which was 1.5 mm greater than that of implant/abutment junction. Therefore, the transmucosal abutment had concave profile, which allowed thicker peri-implant soft tissue rather than a divergent abutment (Fig. 1). Two piece ready-made abutments (Top abutment, Warantec, Seoul, Korea) with 2 mm gingival collar height were utilized for every final restoration. To measure the width and height of buccal supra-implant soft tissue, the following procedures were performed. The impression of an implant restoration and surrounding soft tissue was taken at 6-month follow up appointment with medium/low viscosity silicone impression material (Aquasil, Dentsply International, York, PA, USA). The impression was removed from the patient's mouth after its complete set. The implant restoration and its corresponding abutment were retrieved from the patient's mouth and connected to a fixture replica. In case the implant restoration was cement-retained, small amount of temporary cement (Temp-Bond NE, Kerr Dental, Orange, CA, USA) was used to secure the position of the restoration from its abutment. The restoration/abutment/replica assembly was inserted into the impression. Each restoration/ abutment/replica assembly was very stable in its corresponding impression material. Type IV dental stone (Crystal Rock, Maruishi Plaster Co. Ltd, Japan) was mixed following manufacturer's instruction and poured into the impression body. After the stone set, the impression was removed from the model. The implant restoration and the abutment were retrieved from the model. With use of a dental model trimmer and #1200 carbon abrasive papers, each model was cut in bucco-lingual direction at the most apical point of buccal marginal gingiva. Digital photograph of the sections were taken with a DSLR camera (D40, Nikon, Japan). Using a digital imaging software (Adobe Photoshop, Adobe, CA), a horizontal line which passes from the buccal to lingual platform of fixture replica and another, perpendicular to horizontal line, were drawn (Fig. 2). The width and height of buccal supra-implant soft tissue were measured for 30 implant sites. The overall procedures were described from Fig 3a to Fig 3d.
Statistical Analysis
The means and standard deviations of the width, the height, and the width-height ratio were statistically evaluated by statistics software (SPSS 14.0, SPSS, Chicago, Il, USA) One-way Analysis of Variance was utilized to test the differences in means of width, height, and width/height ratio (P < .05). Tukey HSD post hoc test was performed when ANOVA test indicated statistical significance.
RESULTS
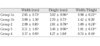
Table I represents means and standard deviations of the width, height and width/height of each group.
There was no significant difference of width among the groups evaluated. The average height of buccal supra-implant soft tissue in Group 4 was greater than that of Group 1b. The width-height ratio of Group 1b was significantly greater than those of Groups 1a, 3, and 4. In addition, Group 1b showed a strong tendency of greater width-height ratio rather than Group 2 (P = 0.051).
DISCUSSION
Esthetic outcomes of implant restorations are influenced by the peri-implant soft tissue as well as the restoration itself.4,13-15 The esthetics of peri-implant soft tissue depends on the level of facial gingiva and the height of interproximal papilla.1 The height of interproximal papilla around implant supported restorations were well documented.13,16 The height of inter-implant papilla is on average 1.5 mm shorter than that of interproximal papilla between implant and natural tooth.17 Until now, less information is available about the characteristics of the facial gingival level. Most of previous studies investigated the change of gingival level around single implant restorations.9-11 No study was performed to measure the level of facial gingiva around multiple adjacent implant restorations.
In natural teeth, the direction of tooth movement and the bucco-lingual thickness of the gingiva are known as the influencing factors determining the position of facial gingival margin.18 Wennstrom reported that there is a ratio of about 1 : 1.5 between its thickness at the most coronal fiber attachment to the root and its height. As like in natural teeth, the position of facial gingival margin of an implant restoration is also influenced by the thickness of buccal supra-implant mucosa. Compared to natural teeth, the average biologic width-height ratio was 1.58 : 1.12 However, the results were measured from single implant restorations with external flat top implant/abutment joints. Rompen and co-workers suggested that abutments with divergent transmucosal profile could create centrifugal pressure at the internal side of the soft tissues and the pressure could result in tendency for recession.19 They evaluated the vertical stability of soft tissue at buccal aspect of implants to which experimental concave, inwardly narrowed transmucosal abutments were connected and concluded that the use of abutments with concave transmucosal profile seems to allow for better and more predictable soft tissue stability than those with divergent profiles.
In the current study, the width, the height and the width-height ratio of buccal supra-implant soft tissue were evaluated not only in single implant restorations but also in multiple adjacent implant restorations. The groups were divided by the number and the position of implant restorations. The results of this study showed that there was no significant difference in the width of buccal supra-implant mucosa between groups whereas the height and the width to height ratio resulted in significant difference between the groups. The width to height ratio of Group 1b was significantly greater than those of Groups 1a, 3 and 4. In addition, Group 1b showed a strong tendency of greater width-height ratio rather than Group 2 (P = 0.051). Compared to other groups, Group 1b comprised of the implant restorations without adjacent natural tooth. Therefore, it is assumed that the width-height ratio of buccal supra-implant soft tissue was influenced by the presence of a natural tooth next to the implant restoration. Based on this result, it is inferred that favorable width-height ratio could result in every single implant restorations whereas unfavorable width-height ratio might be expected in the multiple implant restorations without neighboring natural tooth.
Nozawa and colleagues reported that every single implant restorations showed greater width of buccal supra-implant soft tissue rather than the height.12 However, in the current study, 15 out of 30 implant restorations showed greater height than its corresponding width. Furthermore, the height was always greater than the width of implant restorations in the maxillary anterior segment. These differences could be due to the configuration of transmucosal abutment. Nozawa measured the width to height ratio around transmucosal abutments with divergent profile whereas concave transmucosal abutments were used in the current study.
Impressions were taken 6 months after the delivery of final restorations. It was reported that the majority of the recession occurred within the first 3 months after implant placement surgery for 1 stage implants or abutment connection for 2 stage implants.9 Therefore, 6 months of function was chosen for minimum functional period for the current study.
In this study, soft tissue parameters around single and 2 adjacent implant restorations were evaluated. As three or more adjacent implant restorations were not included in this study, it could not be performed to assess the width/height ratio of buccal supra-implant soft tissue around an implant restoration between the implants. Each group comprised of only 6 implant restorations. Larger sample size and inclusion of more than 3 adjacent implant restorations would be beneficial in gathering more information about the characteristics of peri-implant soft tissue.
CONCLUSION
1. Unfavorable width-height ratio was noted for the second molar in the first and second molar implant-supported restorations.
2. To achieve an esthetic outcome, greater thickness of buccal supra-implant mucosa is required for the implantsupported restorations without any neighboring natural tooth rather than implant-supported restorations next to a natural tooth.



 XML Download
XML Download