

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Surgical conditions account for a significant portion of health problems worldwide and have a substantial impact on public health in low and middle-income countries [1]. Musculoskeletal injury causes disability and suffering and places a heavy burden on society, so such cases are a major source of surgical procedures thus a major concern in public health, globally [2] . This burden on could be considerably lessened by implementation of an affordable and sustainable strategy to accelerate healing in osteotomies and fractures [2]. Osteoporosis (OP) is a disease of the bone common in middle-aged, post-menopausal women. Osteoporotic bones become weak and prone to fracture [3]. In the year 2000, there were an estimated 9.0 million osteoporotic fractures, of which 1.6 million were of the hip; 1.7 million forearm and 1.4 million were clinical vertebral fractures [4]. In 1995, the cost of osteoporotic fractures in the United States in 1995 was estimated at $13.8 billion [5]. The consequences of osteoporotic fracturing include re-fracture, excess mortality and morbidity among patients and burdensome economic cost for the healthcare system [6]. Causes of post-menopausal OP are thought to be multifactorial [7]; however, it is thought that basic pathological events in any type of OP involve an imbalance between bone resorption and formation due to an increase working lifespan or number of osteoclasts and a decline of the working lifespan or numbers of osteoblasts [8]. In postmenopausal OP, estrogen deficiency is thought to promote production of bone-resorbing hormones and cytokines (interleukin-1 [IL-1]), tumor necrosis factor-α [TNF-α], IL-6) with osteoclastogenic action [9]. Conversely, it seems that agents that suppress production of these cytokines could prove helpful in preventing bone loss in postmenopausal OP. In theory, improved bone formation might induce a more adequate recovery of bone mass in osteoporotic patients [10]. This indicates the need to identify agents with osteogenetic potential in order to improve therapeutic efficacy in osteoporotic [10]. A number of in vitro studies have demonstrated that in osteoblastic cells, elevated levels of intracellular cyclic (adenosine monophosphate) AMP develop bone-forming activity [1112]. This is consistent with research reported in Wronsky et al., in that cyclic AMP and cyclic AMP-dependent protein kinase may be the most important initiators of growth response to intermittent pulse of parathyroid hormone (PTH) in rat bone [13]. In addition to the rate of synthesis of cAMP by adenylate cyclase, cAMP levels can be regulated by the rate of hydrolysis to the inactive form of 5' AMP by cyclic nucleotide phosphodiesterases (PDEs). So PDE enzymes degrade intracellular cAMP [1415]. General or non-selective phosphodiesterase inhibitors (1-(5-oxohexyl)-3,7-dimethylxanthine or Pentoxifylline, (PTX)) are effective in elevating intracellular c-AMP levels by inhibiting the breakdown of c-AMP by PDEs [10]. PTX was originally used as a hemorheologic drug to treat intermittent claudication, with minor side effects [16]. Previous studies report positive effects of PTX alone or in combination with other drugs on some pathologic bone diseases including osteoradionecrosis, arthritis; as well as an ability to accelerate osteogensis and fracture healing in both animal models and human patients [1718192021222324252627]. However, only a few studies have elucidated the effects of PTX on osteoporotic cells in vitro or in cases of corticosteroid-induced OP. Robin and Ambrus cultured osteoblast-like cells from calvariae of rats. Tests determined that PTX increased cAMP levels and calcium uptake in these cultures [28]. Robin and Ambrus, reports induced OP in C3H/St (Ha) of female mice after 3 months of treatment by heparin in vitro. Tests determined that PTX prevented OP and increased calcium uptake and cAMP production in osteoblast-like bone cells isolated from fetal rats [29]. Magremanne and Reychler report affirmation that osteonecrosis of the jaw (ONJ) as an important side effect of bisphosphonate (BP) therapy but that was also presented ONJ development after zoledronic acid infusions (3 yearly) for corticosteroid-induced OP. Treatment was successfully managed using conservative treatment with PTX and tocopherol [30]. Recently Takami et al., illustrated that PTX stimulated osteoclast formation in cocultures of mouse bone marrow cells and calvarial osteoblasts. PTX induced expression of osteoclast differentiation factor, TNF-related activation induced cytokine (TRANCE), identical to receptor activator of nuclear factor kappa-B ligand or (RANKL), osteoclastogenesis-inhibitory factor (ODF), and Osteoprotegerin (OPGL)), in calvarial osteoblasts [31].
Alendronate sodium is a nitrogen-containing oral bisphosphonate used for the treatment of osteoporosis [32]. Approximately 50% of patients treated with alendronate show a decrease in the incidence of osteoporotic fractures in the hips and spine as a result of improved bone density and reduced bone resorption. Alendronate makes a continuous decrease in the points of biochemical markers of bone remodeling, recurring them to the premenopausal range. It also increases bone mineral density and declines the risk of osteoporotic fracture in postmenopausal females. Longstanding intervention investigations have revealed that continuous alendronate administration is associated with a sustained therapeutic effect on bone density and remodeling [33].
Latest progresses in imaging technologies for example computerized tomography (CT) scanning have made it possible to evaluate the healing process of the bones by measuring the Hounsfield unit (HU) of bone tissue [3435].
This study aimed to evaluate the effects of PTX administration with 200 mg/kg (which was administered successfully on fracture healing in healthy rats in previous studies [1725] on Hounsfield unit and biomechanical parameters of callus of complete osteotomy of femur in an experimental rat model of ovariectomy induced OP (OVX-D). The remodeling phase of fracture healing (catabolic phase) was evaluated with Hounsfield unit and a biomechanical test [36].
Materials and Methods
Animals and study design
Thirty adult female Wistar rats, 5 months old and weighing about 240 g, were used. Rats were provided with food and water ad libitum and were weighed weekly throughout the study duration. Rats were divided into groups 1 (OVX, control: no treatment); 2 (OVX, sham: daily distilled water, intraperitoneal,IP); 3 (OVX, daily alendronate: 3 mg/kg, subcutaneous, SC, Alborz Darou, Tehran Co, Iran); 4 (OVX, daily PTX: Sigma-Aldrich, St. Louis, MO, USA,IP, 100 mg/kg at 9 a.m. and 100 mg/kg 5 p.m.) and 5 (OVX, PTX+alenderonate). OVX was induced in all rats. A complete standardized osteotomy of right femur was made after 3.5 months. PTX and alendronate treatments were performed for eight weeks. Then, rats were euthanized and the right femur of each rat was submitted to CT scanning and a three point bending test to evaluate callus density and strength of the repaired bone. All procedures were approved by the Medical Ethics Committee at Shahid Beheshti University of Medical Sciences,Tehran,Iran (protocol no 1392-1-115-1159).
Ovariectomy
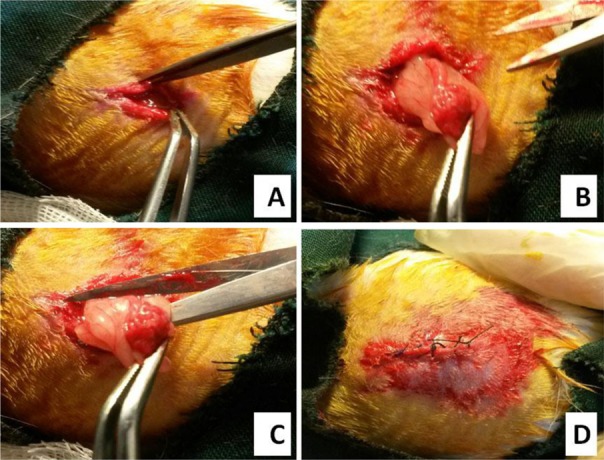
All rats were subjected to total OVX. OVX was carried out on two paravertebral skin incisions while rats were under sterile conditions and general anesthesia. On the day of surgery (day zero), each rat was anesthetized with an intramuscular injection of ketamine (50 mg/kg) and diazepam (5 mg/kg) for relief of postoperative pain rats received 20 mg/kg Ibuprofen (Emaddarmanpars Co, Tehran, Iran) preoperatively and then every 8 to 12 hours for the next 5 days after surgery [37]. The skin of each rat was shaved and sterilized with several scrubs of povidone iodine (betadine) and 50% ethanol. Uterine tubes were ligated and incisions were closed following removal of ovaries (Figure 1) [36]. Antibiotic therapy with Ceftriaxone (Jaber ben Hayan Co, Tehran, Iran) at a dose of 50 mg/kg was injected intramuscularly into the rats immediately before surgery and then 24 and 48 h after surgery. All animals were kept for 3.5 months after surgery in cages in order to develop OP [3138]. At the end of this period, rats were submitted to CT scanning to establish OP. Rats were then subjected to complete osteotomy in the right femur.
CT scanning
OP development of OVX-D and callus densities was evaluated qualitatively by CT using multislides (kV=100, ma=50, sections=2 mm, FOV=240 mm, Toshiba, Aquilion 16, Japan) when compared with healthy rats. Evaluation of femoral bone density of osteoporotic rats was determined under general anesthesia. Moreover 2 months after OVX callus densities of all rats were evaluated by the CT scanning. Callus densities of bone defects were determined immediately after euthanizing. All tests were performed by an expert radiologist and bone density evaluations were recorded in Hounsfield Units (HU) [34]. The radiologist was unaware of the group divisions.
Femoral fracture model (surgical standard complete transverse osteotomy)
Each rat was anesthetized, had its skin sterilized and antibiotic therapy was performed as mentioned before. One incision (1-cm) was made over the lateral aspect of the right thigh to expose the femur. The first step was to make three to five partial transversal standardized osteotomies, circular deep to the central medullary canal at midpoint of the femur. These were made with a low speed drill (terminal, 1.0-mm diameter) (Delab; Dental Fabriktreffurt, Germany), then the osteotomy site was broken manually and bones were divided into two parts. During osteotomy bones were irrigated with saline solution to avoid burning. Intramedullary fixation was performed using stainless wire (diameter, 1.0mm). Fracture fragments were contacted and stabilized. A distance of 3 mm (gap) was maintained between the edges of fractures, constant in the entire population of rats. Wires were cut on the surface of the femur`s intercondylar groove to avoid restricted motion in the knee joint. Muscle tissue was sutured with 04 catgut (Supa, Iran) and skin was sutured with 04 nylon reversed cutting sutures (Figure 2). Unrestricted activity was allowed after recovery from anesthetic [17].
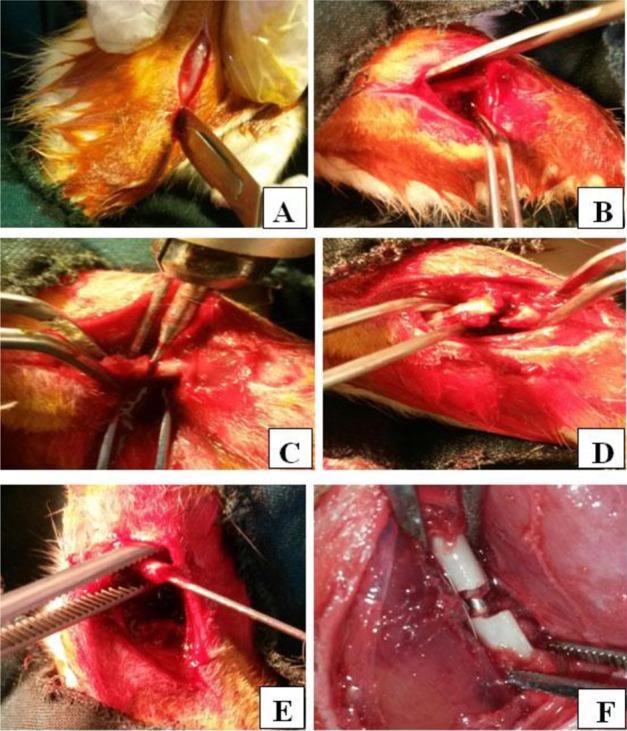 | Figure 2Different steps of complete osteotomy operation. The image shows the incision (A), exposed femur s mid shaft (B), circular partial transversal standardized osteotomies procedure with low speed drill (C), complete fracture in the bone (D), inserting a stainless wire (E). Reduction was maintained with the stainless wire (F)
|
Biomechanical examination
Eight weeks after surgery, all rats were anesthetized in the same way as before. During anesthesia, rats were euthanized via an intracardiac dose (200 mg/kg) of pentobarbital sodium and benzyl alcohol (Dolethal). Right femurs were collected. Biomechanical properties of six bones in each group were examined. Bones were submitted to three-point bending on a material testing device (Zwick/Roell Group Z 2.5 H 15WN, UIm, Germany) until fracture occurred. All bones were oriented similarly in the testing machine. Two loading bars, 19 mm apart were used to mount each bone, and a mobile head was activated to compress the midline of the bone shaft until fracture occurred. The compressive loading speed in the test was 0.08mm/s. Data were automatically recorded by the material testing device from the load-deformation curve and the following values were calculated: bending stiffness (N/mm), maximum force (N), high stress load (N/mm2), and energy absorption (N mm)[17].
Statistical analysis
All data were expressed as mean±standard deviation. Normal distribution of data were analyzed using one sample Kolmogorov-Smirnov test. Differences between treatment groups were tested by one-way analysis of variance (ANOVA). If significant difference was indicated, then difference between the two groups was tested by Least Significant Difference (LSD). First body weight of rats and their last body weights, and Hounsfield units of OVX-D and healthy control groups were analyzed using the student t test. The P value of <0.05 was considered statistically significant.
Go to : 
Results
General observations
There were no adverse effects such as oral hemorrhage, vomiting, diarrhea or dysentery were observed in any of the rats. A total of 7 rats were excluded due to poor fracture healing (non-union) or death after surgery. These 7 rats were replaced. Rats in the alendronate and alenderonate+PTX groups showed a significant decrease in body weight at the end of the study (Table 1).

Hounsfield units analysis
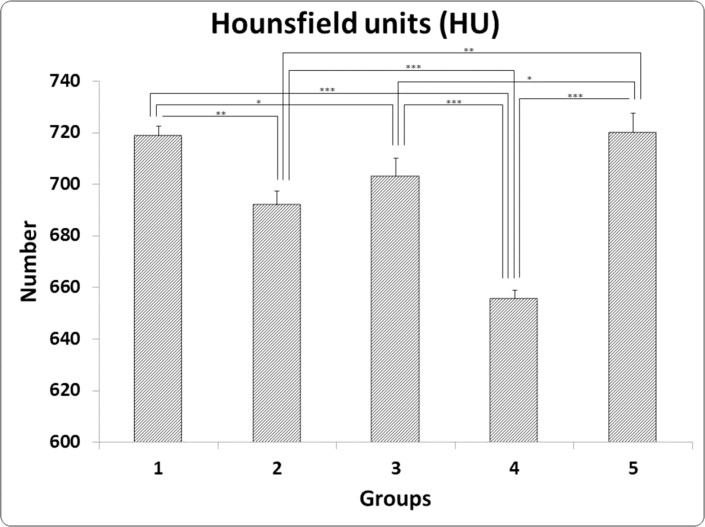
Student t test analysis revealed a significant decrease in femoral bone density of OVX-D (635.8±24.36 HU) compared with the control (healthy group) (787.8±24.8 HU), (P=0.000).
PTX-treated rats showed significant decrease in Hounsfield unit compared to alendronate, and alendronate +PTX groups (LSD test, both P=0.000). There were significant decrease in Hounsfield unit of PTX, sham, and alendronate groups compared to control group (LSD test, P=0.000, 0.002, and P=0.002, respectively). LSD test showed significant differences among sham group, and PTX and alendronate+PTX groups (P=0.000 and P=0.002, respectively). All results were shown in Figure 3.
Three point bending analysis
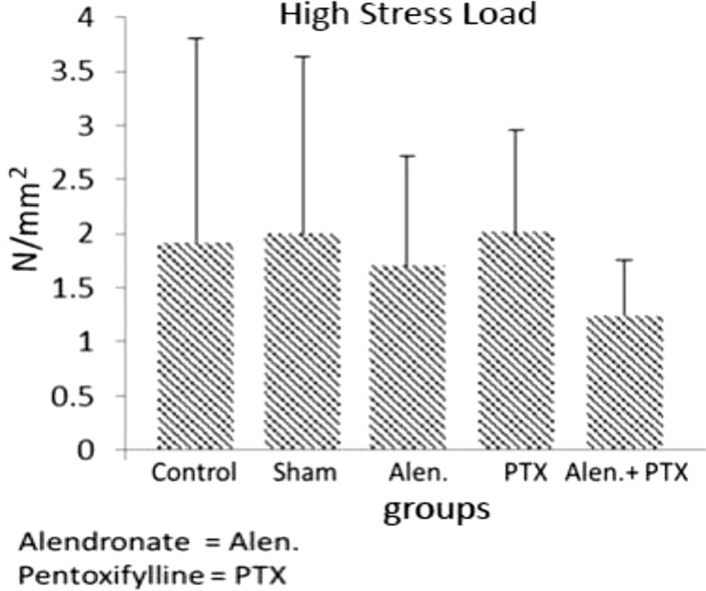
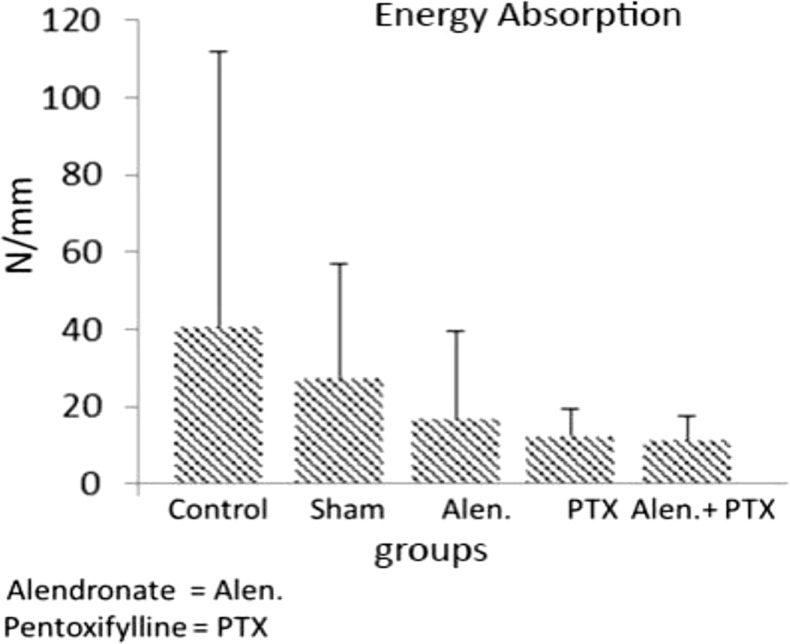
As shown in Figures 4, 5, 6 and 7 administration of PTX and alendronate alone and in combination did not significantly alter biomechanical properties of repairing complete osteotomy of femur compared with the control group.
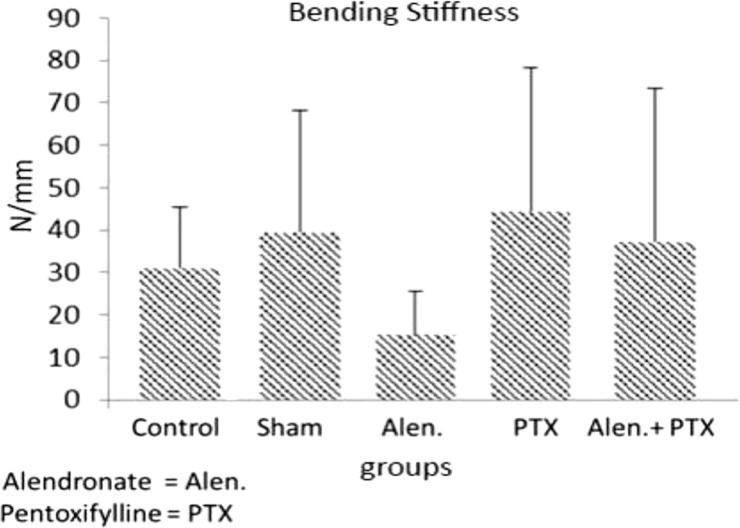 | Figure 4Mean±SD of bending stiffness in the groups compared by the ANOVA and LSD tests. Groups: 1 (OVX, control), 2 (OVX, Sham), 3 (OVX, alendronate), 4 (OVX, PTX), and 5 (OVX, PTX a nd alendronate).)
|
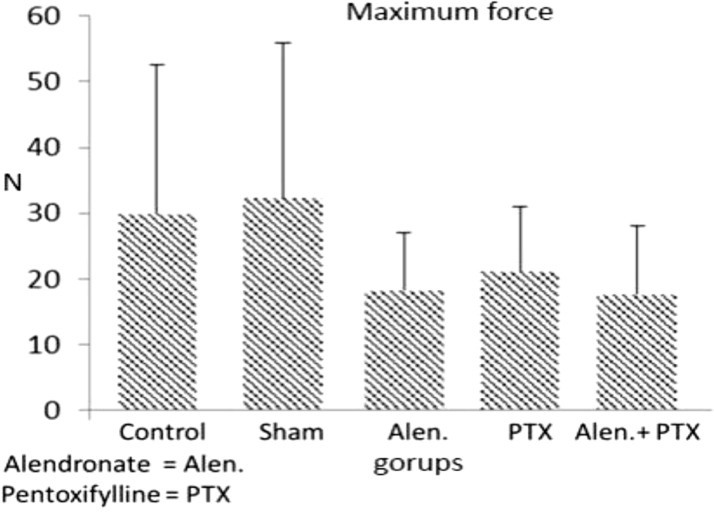 | Figure 5Mean±SD of maximum force in the groups compared by the ANOVA and LSD tests. Groups: 1 (OVX, control), 2 (OVX, Sham), 3 (OVX, alendronate, 4 (OVX, PTX), and 5 (OVX, PTX and alendronate).
|
Bending stiffness (N/mm)
The mean value of PTX group was higher than that of other groups. However the ANOVA evaluation for bending stiffness revealed no significant difference among the studied groups.
Maximum force (N)
The mean value of Sham group was higher than other groups. However the ANOVA for maximum force revealed no significant difference among the studied groups.
Stress high load (N/mm2)
The mean value of PTX was higher than that of other groups. However the ANOVA for stress high load revealed no significant difference among the studied groups.
Energy absorption (N mm)
The mean value of control was higher than that of other groups. However the ANOVA for energy absorption revealed no significant difference among the studied groups.
Go to :
Discussion
Fracture healing is a process in which injured bone recovers in both tissue formation and functional aspects. OP postpones the healing process and contributes to personal suffering and loss of activity. Osteoporotic patients are more prone to lose bone mass at the metaphyseal region which will then require treatment to improve bone mass. Therefore, it is important to investigate treatment with osteogenic potential and the capability to stimulate bone formation and to prevent bone loss [39]. Postmenopausal OP is the most common type of OP to affect women and lead to pathologic fracture. Estrogen Replacement Therapy (ERT), the recommended therapy for postmenopausal OP, is associated with higher risk of breast cancer, ovarian cancer and cardiovascular diseases [40]. According to the public health concern caused by the burden of osteoporotic fractures, it is important that alternative treatment should now be thoroughly explored. Current drug therapy has been determined as inadequate to control incidence of OP and its complications such as fracturing [41]. Therefore, tests are being done for new anti-OP agents to provide more effective options than the current drugs used to control OP. PTX is used to manage vascular diseases such as ischemic heart disease and intermittent claudication. It improves peripheral blood ow by increasing erythrocyte exibility and vasodilatation. It also has an antitumor necrosis effect and may inhibit inammatory reactions and decrease brosis [16]. Studies have shown that PTX has a positive effect administration on different complex skin wound healing models [42434445].
In the current study, we used a biomechanical measurement of the effect of PTX on bone fracture healing, which is essentially the ultimate proof of real alterations in bone repair-the strength of the healed bone [46]. Results of this current work show an increase in bending stiffness and stress high load mean values of repairing complete osteotomy in PTX-treated rats compared to control OVX-D. Results showed a trend toward effectiveness of PTX administration for improving biomechanical parameters of fracture callus in OVX-D. However, no significant difference was determined in the biomechanical parameters between PTX-treated rats and control OVX-D. It can be supposed that in the current study, PTX administration did not increase intracellular cAMP levels.
Bone strength is indirectly estimated by bone mineral density (BMD) by using Dual-Energy X-ray Absorptiometry (DXA). Considering DXA-measured BMD accounts for 60-70% of the variation in bone strength; in addition, the effects of anti-osteoporotic treatment and progression of osteoporosis were not captured by DXA. Geometry and trabecular microarchitecture should also be taken into account indeed. The assessment of the intrinsic mechanical quality of bony tissue should provide a better understanding regarding the role of tissue quality in determining bone strength [4748].
Previous in vitro studies have shown that PTX promoted cellular and molecular pathways of bone formation. PTX promoted differentiation of osteogenic precursor cells toward an osteoblastic phenotype [49]. Consistent with these results are those reported in Rawadi et al., showing a positive effect of PTX on osteoblastic differentiation in vitro by using two mesenchymal cell lines, C3H10T1/2 and C2C12. These two mesenchymal cell lines were able to acquire the osteoblastic phenotype in the presence of bone morphogenetic protein-2 (BMP-2). Results determined that PTX induced the osteoblastic markers, osteocalcin and Osf2/Cbfa1, in these cells and enhanced BMP-2-induced expression of osteocalcin, Osf2/Cbfa1, and alkaline phosphatase [50]. Mcleod et al., reports on presence of radiation-induced fibrosis and suggests that the key event in development and progression of the condition is dysregulation of fibroblastic activity in irradiated areas, which not only damages atrophic tissue by damaging micro vessels but it allows for increased leakage of inflammatory mediators. The existence of inflammatory mediators such as TNF-alpha in the irradiated tissue then triggers further inflammatory response that causes more damage to local tissue. PTX has been found to act against some inflammatory mediators including TNF-alpha. However, Tocopherol is a methylated phenol compound with Vitamin E activity and is a scavenger of reactive oxygen species. Mcleod et al., reports that these two drugs in combination had a positive synergistic effect on the progression of fibrotic and inflammatory lesions that were caused by radiotherapy treatment [51].
Bisphosphonates have been recognized to have a positive effect on bone mineral density (BMD) and fracture incidence in osteoporotic bones. They are considered an effective, safe and are well tolerated; they can increase bone mass and reduce risk of fracture in primary and secondary OP [52]. Results of this study showed that alendronate-treated OVX-D did not reveal an increase in biomechanical parameters of repairing complete bone osteotomy compared to the control OVX rats. This observation is in accordance with results of a previous study [45]. Kolios et al., investigated the prophilactic effects of estrogen and alendronate on rats with OP. After 10 weeks of OVX, standardized T-plate fixation and metaphyseal tibia osteotomy procedures were done. Tests determined that administration of estrogen significantly improved biomechanical properties and resistance to micro fracturing of callus compared to control and sham groups. Alendronate did not accelerate bone healing, which was shown by mechanical tests. Kolios et al., concluded that osteoporotic metaphyseal fracture healing was qualitatively and quantitatively improved by estrogen prophylaxis [53].
The following hypothesis presents an explanation of the lack of stimulatory effect of the PTX administration on osteoporotic rats that it could be due to inadequate or improper dosage. Vashghani Farahani et al., assessed the effects of different dosages of PTX on biomechanical properties that take place during the late phase of the fracture healing process following a complete femoral osteotomy in a rat model. They divided 35 female rats into groups as follows; group 1 received PTX (50 mg/kg, once daily), starting 15 days before surgery, and group 2, group 3, and group 4 received 50, 100, and 200 mg/kg i.p. PTX, respectively, once daily after surgery. All animals received treatment for six weeks (until euthanized). Complete surgical transverse osteotomy procedure was performed in the right femur of each rat. At six weeks after surgery, femurs underwent a three-point bending test. It was determined that daily administration of 50 mg/kg PTX (groups 1 and 2) declined the high stress load in repairing osteotomized femur in comparison to the control group. The highest dose of PTX (200 mg/kg) significantly escalated high stress load in comparison to the control group, and groups 1, 2 and 3, per LSD findings. Vashghani Farahani et al., concluded that treatment with 200 mg/kg PTX accelerated fracture healing compared with the control group [17].
Go to :
Conclusion
It was concluded that PTX administration with 200 mg/kg displayed no significant positive effect on biomechanical parameters of callus strength in OVX-D in the remodeling phase of complete femoral osteotomy. Further to this study it is suggested that different doses of PTX administration be tested on fracture in OP rats.
Go to :
 XML Download
XML Download