

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Intervertebral disk herniation (IVDH) occurs in both the cervical and thoracolumbar vertebral column and is a common cause of spinal cord injury (SCI) in veterinary species [1]. Hansen described two types of IVDH, classified as Hansen type I or chondroid degeneration and Hansen type II or fibroid degeneration, that can result in IVDH and spinal cord compression [2]. Both types of IVDH can occur in any of the vertebral levels. Meanwhile, Griffiths described another type of IVDH that may also occur in the cervical spine [3]. This type of extrusion occurs when non-degenerated nucleus pulposus extrudes during strenuous exercise or trauma causing spinal cord contusion with little or no residual spinal cord compression [4]. The symptoms may differ depending on the severity, but acute traumatic spinal cord injury (SCI) by vertebral disc herniation or degeneration is a devastating clinical condition in human as well as in animals [56].
Among nonhuman primates (NHPs), cynomolgus monkeys of more than 20 years old and with naturally occurring thoracolumbar IVD degeneration are utilized in orthopedic research [7]. Many SCI cases in NHPs are experimentally induced animal models for the understanding of its pathogenesis and an evaluation of therapeutic regimens in human practices [68910111213]. Until now, there has been no report of SCI from IVDH caused by accidental, rather than deliberate, blunt trauma. In this case report, we describe the clinical and magnetic resonance imaging features of compressive cervical SCI with suspected nucleus pulposus extrusion in a cynomolgus monkey.
A 4-year-old male Cambodia-origin cynomolgus macaque weighing 3.4 kg was housed at an AAALAC-accredited Seoul National University Hospital Nonhuman Primate Center (SNUHNPC) and assigned to type 1 diabetes study approved by the SNUH Institutional Animal Care and Use Committee. For pancreatic islet transplantation study, the monkey was induced to have type 1 diabetes by streptozotocin. Measurement of blood glucose level and administration of insulin were performed twice daily with pole and collar method of restraint [14]. Throughout the experimental period this monkey showed an exceptionally consistent resistive behavior against capture and restraint procedure compared with other monkeys. Unfortunately, whenever this monkey was captured with pole and collar, extensive struggling movement was consistently represented, and this behavior did not improve with time.
At 3 months after diabetes induction, the monkey suddenly presented dull and stiff movement in home cage, while a typical fast and agile movement was remarkably reduced. Eventually, the monkey fell down feebly from a perch of the cage and then was unable to stand up by himself. Urinary incontinence was also observed. On physical examination, the monkey showed a loss of voluntary motor function in thoracic and pelvic limbs, even though normal on joint palpation. In addition, there was no grip strength of the hands or feet. Meanwhile, facial movements including of lips, eyelids, and ears were normal. From hematology and serum biochemistry, there were no significant findings. At the onset of clinical symptoms, a hypoglycemic shock, which occurs commonly in diabetes monkeys because of high dose of exogenous insulin or brittle diabetes, was suspected. However, this was ruled out because the blood glucose level was within the normal range at 73 mg/dL.
On neurological examination, loss of voluntary motor function in all four limbs was observed. The upper motor neuron (UMN) signs showed in thoracic and pelvic limbs. However, no sign involving the head was present. Perception of superficial and deep pain as well as proprioception were decreased in thoracic and pelvic limbs. Moderate hyperesthesia was present on palpation of the cervical area. Based on these findings, we localized the lesion to segment C1-C5.
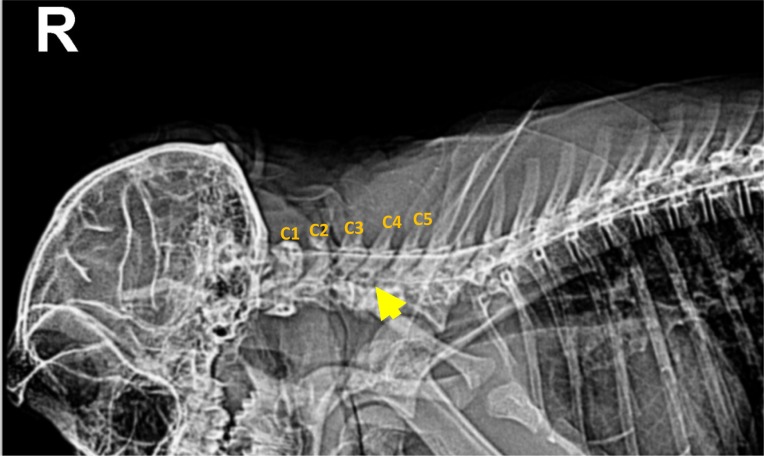
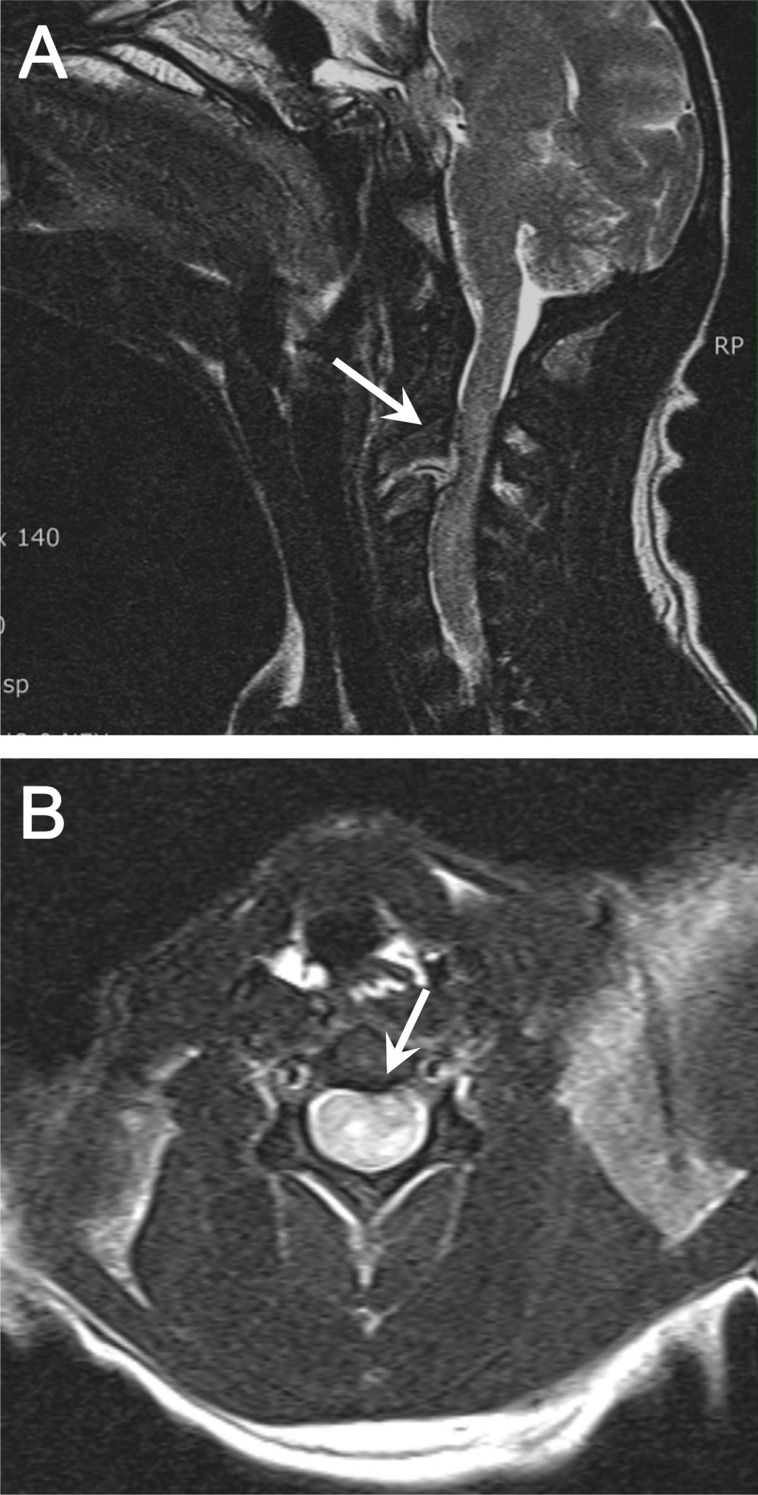
In conventional radiographs, a distinct abnormality was not found in the cervical region or in other vertebral columns or the musculoskeletal system. However, in a lateral cervical myelogram using Iohexol (Omnipaque, GE, Cork, Ireland), a disappearance of the ventral contrast column was distinctly identified between C1 and C4 (Figure 1). On T2 weighted sagittal and transverse MR images, the cervical disc protrusion was clearly defined between C2 and C3 (Figure 2A, B). This protrusion of disc caused dorsal compression of the spinal cord.
Prophylactic and supportive treatment with cefazolin (25 mg/kg, IV, BID; CKD Pharm., Seoul, Republic of Korea) and methylprednisolone (0.5 mg/kg, IV or IM, SID; Pfizer, NV, Belgium) was initiated with an intravenous fluid therapy (normal saline, 10 mL/kg/hr). In spite of this, the neurologic problems of the monkey were not improved despite long-term treatment. Eventually, the monkey was euthanized after 3 months from the onset. In gross findings, degenerative inflammatory lesion was found between the cervical spinal cord and intervertebral dorsal pedicles. In histopathological findings, the cervical spinal cord was compressed with an extensive area of necrotizing granulomatous inflammation in which a large number of neutrophils and lymphocytes were infiltrated (Figure 3A, B).
Discussion
Hansen type I IVDH caused by suspected traumatic injury, as described herein, has not been previously reported in nonhuman primates. This case reports that the affected monkey showed acute neurological problems with tetraplegia, and compressive SCI was defined through myelogram, MRI finding, and histopathology.
The vertebral level at which traumatic or degenerative myelopathies occur is diverse and is important in ambulatory function in human as well as veterinary species. In human, the most common site of SCI is the cervical spinal cord (C1-C7) with approximately 55% of injuries [1115], and the number of injuries at this level is increasing [16]. The critical cause of SCI is blunt trauma such as a motor vehicle collision and falls [12]. In dogs, 83.6% of SCI is associated with IVDH, located in the thoracolumbar region between T10 and L7 [17]. Among all dogs with cervical disc herniation, the most commonly affected IVD spaces are represented at C5-C6 and C6-C7 [1819]. In nonhuman primates, the experimentally induced SCI model has been reported, but acute cervical SCI associated IVDH has not been reported.
The affected monkey was trained by using positive and limited negative reinforcement for pole-and-collar moving to the home cage front [14], where he then was restrained. Given time constraints, there was a failure to habituate, resulting in undesirable behavior (that is, the monkey was forcing his neck from the collar) throughout the training period. It seems that repetition of the resistive movement against a collar increased the possibility that a strong force of collision would be delivered to the cervical vertebral column, which in turn made it more likely that the intervertebral disc would become herniated toward the spinal cord.
Images (e.g., plain view, myelogram, and MRI) of the affected monkey, in which the lesion was clinically localized to the C1-C5 spinal cord segment, were taken to include the C1-C5 spinal cord segments in order to investigate the potential underlying cause of the clinical presentation. On T2 weighted sagittal and transverse MR images, unlike the plain and myelogram images, the cervical disc protrusion was clearly defined between C2 and C3. Moreover, the protruded disc excessively compressed toward the spinal cord.
It has been shown with MRI that more severe abnormalities are associated with a more severe neurological status [20]. In other words, hemorrhage, the number of levels of edema, greater degree of cord compression, greater degree of canal compromise, and the severity of soft tissue injury have been shown to be associated with worse neurological outcome in human [2122232425]. This is because blunt SCI in human is characterized by typical pathologic changes including petechial hemorrhages that coalesce into large hemorrhages with time [26]. In particular, compressive SCI associated with IVDH is believed to result in a complex cascade of secondary mechanisms including vascular disturbance, oxidative stress, excitotoxicity, and inflammation [17].
In the current case, although hemorrhagic or edematous lesion was not found in the histopathologic findings carried out in the several weeks post-injury, a disruptive inflammation was revealed between the spinal cord and the intervertebral disc in the autopsy finding. The extruded disc material probably irritated the spinal cord, resulting in inflammation in that area. In a previous study, it was reported that blood-spinal cord barrier disruption and associated innate inflammatory events occurred within hours of SCI and caused neutrophilic diapedesis and microglial activation [27]. Moreover, in the days and weeks after SCI, adaptive immune responses are initiated because of exposure of self-antigens and may cause lymphocytic and mononuclear cell infiltration within injured parenchyma [27].
In conclusion, the underlying cause of clinical symptoms in this case was confirmed through MR images to be a compressive cervical myelopathy caused by acute IVDH. This neurologic deficit was not restored to normal, although initial neurological symptoms were shown to be slightly improved by supportive medical care. It is probable that blunt trauma due to repetitive collision with a neck collar contributed to cervical IVDH and SCI in an untrained cynomolgus monkey.

 XML Download
XML Download