

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Peptic ulcers are one of the common gastric illnesses in modern societies. Gastric erosions and ulcers are caused by various factors including over-secretion and retention of gastric acid, depletion of protective mucin layers, disturbances in focal blood flow, and local inflammation [1,2,3,4]. Ulcer-inducing agents cover nonsteroidal anti-inflammatory drugs [5,6,7,8,9], alcohols [7,8,10], stresses [4,7,8], gastric retention [7,8], gastric hypermotility and acetic acid accumulation [8,11,12,13,14], and Helicobacter pylori infection [1,2,15,16,17].
Since H. pylori infection is related to inflammations, the bacteria are detected in gastric ulcer (70%), gastritis (50-60%), and duodenal ulcer (90%) patients. It has been confirmed that H. pylori is a key factor for chronic active gastritis as well as development to gastric malignancies [18,19,20]. It is well known that H. pylori exacerbates erosions and ulcers by stimulating gastric secretion and retention [21,22]. Accordingly, it is believed that eradication of H. pylori is the most important for effective ulcer treatment in patients exhibiting chronic and repetitive incidence of gastritis [1,2,15,16,17,23].
In order to eliminate H. pylori and treat gastric ulcers, triple therapies composed of proton-pump inhibitors, such as pantoprazole and omeprazole, and antibiotics, such as clarithromycin, metronidazole, and amoxicillin, have been recommended [2]. However, it was recently confirmed that H. pylori exhibits a high tolerance to the antibiotics [24]. Therefore, in spite of relatively-weak potency compared with the antibiotics, natural products without tolerance during repeated treatments may contribute to the eradication of H. pylori from the stomachs.
Extracts of Laminaria japonica and Cladosiphon okamuranus has been widely used in Oriental medicine. Extensive researches demonstrated that the extracts of L. japonica and C. okamuranus contain fucoidan, a sulfate polysaccharide complex, as an active ingredient, that has anti-oxidative, anti-coagulative, and anti-inflammatory activities [25,26]. In addition, the beneficial effects of fucoidan on inflammatory diseases, ischemia, and immune dysfunction are reported [27,28]. Recently, investigators showed that fucoidan interfere with the attachment of H. pylori to gastric cells in animals and in humans [29,30]. On the other hand, tannins from Oenothera biennis seed also have anti-H. pylori activity [31]. Moreover, L. japonica extract (LJE) was confirmed to inhibit bacterial growth in vitro and to block adhesion and colonization of H. pylori in the gastric walls [32]. We also demonstrated that a combinational treatment with LJE and O. biennis seed extract (OBE) killed H. pylori and eliminated the bacteria from the mouse stomachs in vitro and in vivo [33]. Also, effectiveness of the combinational therapy in reducing H. pylori was confirmed by indirect analytical methods; i.e., urea breath test (UBT) and serum pepsinogen I/II levels, in human patients [34].
In the present study, we investigated the comparative H. pylori-eliminating activities of FEMY-R7, a combinational preparation of LJE and OBE in mice and in humans by directly analyzing the presence of bacteria in feces through a Campylobcter-like organism (CLO)-detection test and bacterial identification.
Materials and Methods
Materials
FEMY-R7 containing LJE and OBE (1:1) was obtained from Misuba RTech Co. (Asan, Korea). After washing, drying and grinding, L. japonica was extracted with a hot water extraction method at 60℃ for 24 hours [33,34]. Subsequently, the extract was filtered through a 0.45 µm membrane, and concentrated in a vacuum evaporator. After sterilization, the extract was spray-dried. The O. biennis seeds were extracted with 60% ethanol, filtered, and concentrated. After sterilization, 67% maltodextran was added to the extract and spray-dried.
H. pylori culture and identification
H. pylori (ATCC49503) was obtained from American Type Culture Collection (Manassas, VA, USA), and cultured on brain heart infusion (BHI) broth in an anaerobic chamber with 10% CO2, 5% O2, and 85% N2 at 37℃ with enough humidity [35].
Animals and treatment
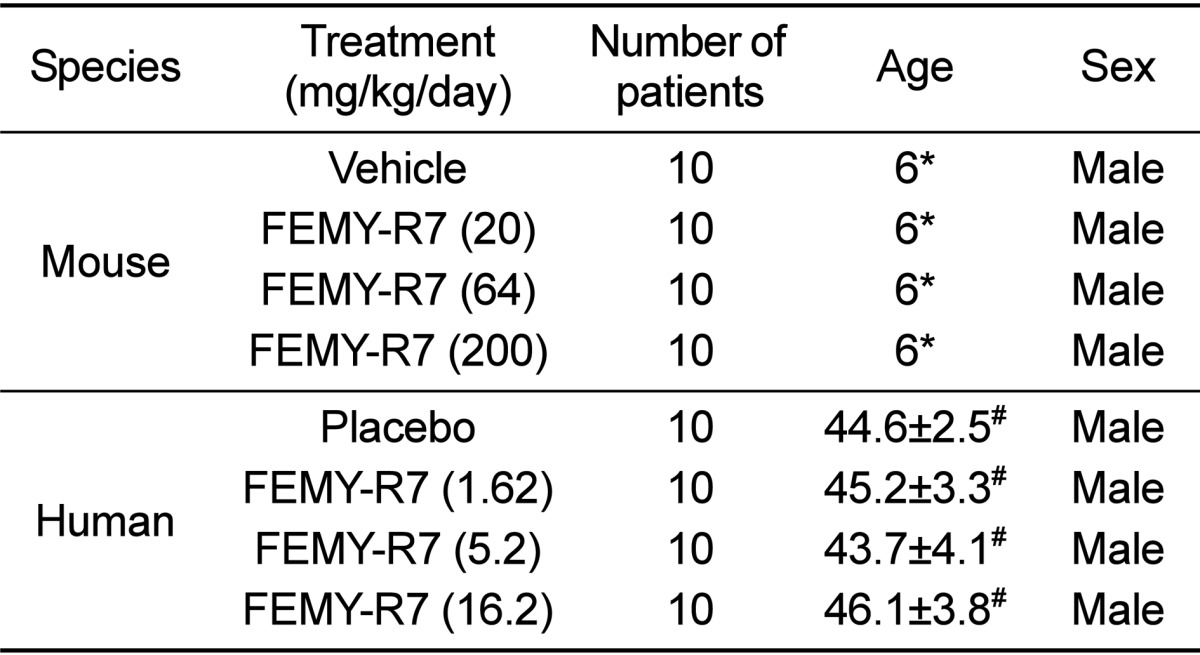
Male C57BL/6 mice (body weights 25-27 g; Table 1) were procured from Daehan Biolink (Eumseong, Korea), and housed in a room with constant environmental conditions (23±2℃; 55±10% relative humidity; 12-hour light-dark cycle; 150-300 lux brightness). Pellet feed and purified water were available ad libitum. All the animal experiments were conducted according to the Standard Operation Procedures (SOP), and approved by the Institutional Animal Care and Use Committee of Chungbuk National University, Korea (Approval No. CBNUR-284-11).
After 12-hour fasting, the mice (n=10/group) were orally inoculated with H. pylori (1×109 CFU/1 mL/mouse) 3 times at 2-day intervals [34], and simultaneously, orally treated twice a day with FEMY-R7 (total 20, 64 or 200 mg/kg/day) for 2 weeks.
Human subjects and treatment
Among total of 58 male patients (30-60 years old) who visited the Gastroenterology Department of the Catholic University Medical Center in Daegu, 40 patients were enrolled in the present study (Table 1). Enrollment criteria included infection of H. pylori which was confirmed by CLO test on the feces of patients without experience of H. pylori treatment with antibiotics within 4 weeks [34]. The study protocol was approved by the Institutional Review Board (IRB) of the Catholic University Medical Center in Daegu (Approval No. CR-10-074-RES-01-R), and written informed consent was obtained from all patients.
We designed a randomized, double-blind, placebo-controlled clinical trial for eradication therapy of H. pylori. The patients in treatment group were given twice a day FEMY-R7 capsules containing 1:1 mixture of LJE and OBE (total 1.62, 5.2 or 16.2 mg/kg/day: 100, 320, and 1,000 mg/man/day) before a meal for 8 weeks [34]. The patients in placebo control group were given only the capsules containing 1,000 mg microcrystalline cellulose. During the treatment period, the patients were requested to keep their own dietary lifestyle.
Bacterial identification
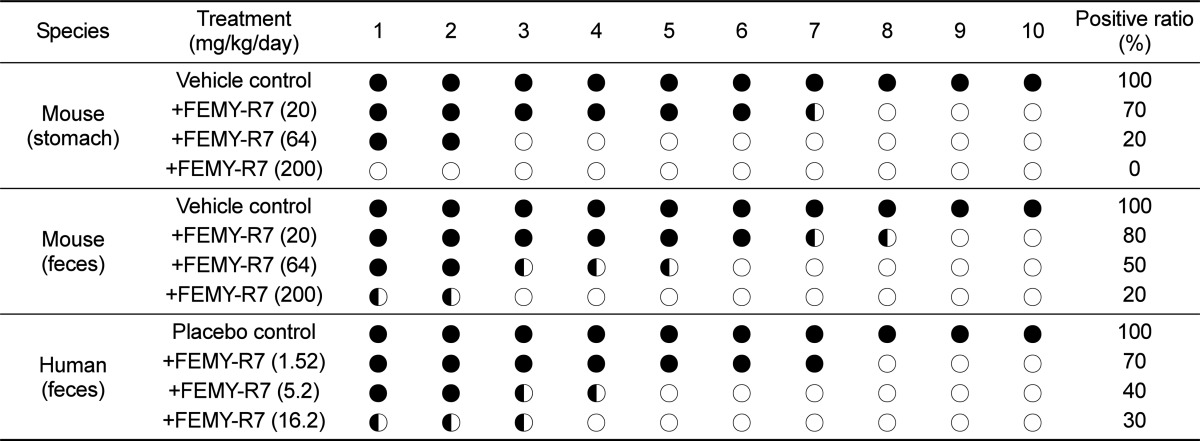
Three hours after the final administration, the mice were sacrificed, and their gastric mucosa (3×3 cm) from the pylorus was biopsied and minced. Additionally, 0.5 g feces of mice (from rectum and colon) and humans (after defecation) were collected, and suspended in the same volume of distilled water and filtered. The gastric mucosal and fecal samples were applied to CLO kits (Kimberly-Clark, Roswell, GA, USA), and incubated at 35℃ for 24 hours to examine urease activity. The reaction (color change) was determined as negative for bright yellow, false (partially) positive for thick yellow, or positive for thick (dark) red [16,17,33,34,35].
Additional feces samples were centrifuged at 500×g for 3 min, and inoculated to a medium containing 20% glycerol for identification of H. pylori as follows [35]:
Oxidase: A colony was collected with a platinumloop, and moved to a filter paper. After dropping p-phenylenediamine dihydrochloride solution, blue change following indolphenol blue production was determined as positive reaction.
Catalase: The colony grown in selective medium was placed on a slide, and bubbling following dropping 3% H2O2 was determined as positive reaction.
Nitrate reduction: Cultured colony was inoculated to nitrate broth, and incubated at 35℃ for 48 hours. Reddish purple change by adding α-naphthylamine and sulfanilic acid was determined as positive reaction.
H2S formation: The central portion of a colony was collected with a platinum-loop, and spread on the slant Triple sugar iron (TSI) medium. Black change following incubation at 37℃ for 24 hours with the lead open was determined as positive reaction producing H2S.
Results
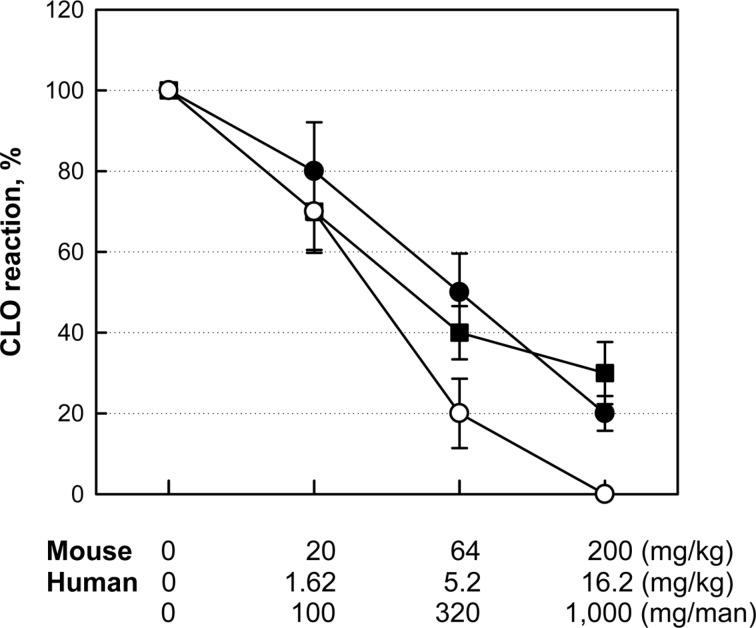
Repeated intragastric inoculation (1×109 CFU/mouse, 3 times) of H. pylori to C57BL/6 mice revealed positive reaction (red color) in CLO test on the gastric mucosa (Table 2). The stomachs of mice orally treated with 20, 64 or 200 mg/kg/day FEMY-R7 for 2 weeks displayed positive reaction in 70% (including partial positivity), 20%, and 0% mice, respectively. By comparison, the CLO positive reactions from feces of the same mice were 80, 50, and 20% with 20, 64 and 200 mg/kg/day FEMY-R7, respectively, although there were several partially-positive mice. On the other hand, treatment of human patients with 1.62, 5.2 or 16.2 mg/kg/day (100, 320 or 1,000 mg/man/day) FEMY-R7 led to 70, 40, and 30% CLO-positive reaction in feces, respectively. Collectively, there was a good dose-response relationship in feces between mice and humans (Figure 1). However, the dose dependency in CLO reaction on mouse gastric mucosa was somewhat different from that of feces.
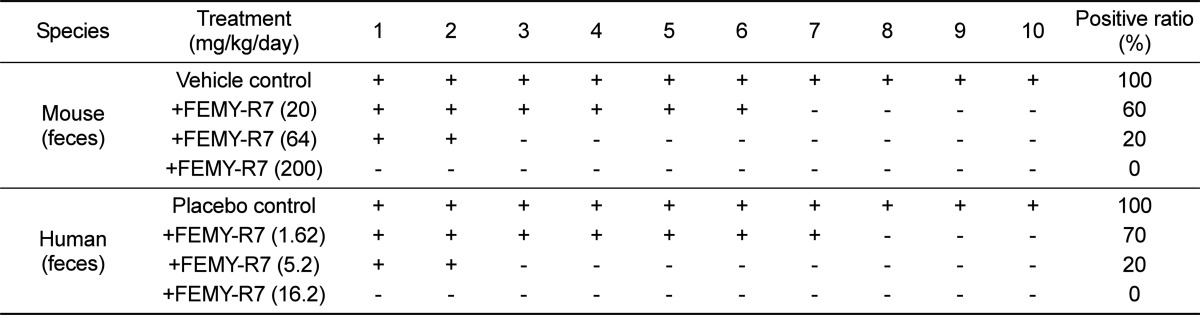
Because of the difference in the CLO test results between stomach and fecal samples of mice, we cultured and identified H. pylori from feces of mice and humans. H. pylori was identified from the stools of all (100%) the mouse and human patients treated with vehicle or placebo preparation (Table 3). However, FEMY-R7 treatment at 20, 64, and 200mg/kg/day decreased the bacterial detection from the mouse feces to 60, 20, and 0%, respectively. Similarly, 1.62, 5.2, and 16.2 mg/kg/day FEMY-R7 in humans reduced the H. pylori-identification ratio to 70, 20, and 0%, respectively.
Discussion
It is well known that H. pylori secretes urease to survive in acidic environment and to invade gastric mucosa, inducing gastritis, ulcers, and sometimes stimulation of gastric cancers. In a previous investigations [33,34], we demonstrated that FEMY-R7 has an anti-bacterial activity against H. pylori. In CLO test, treatment with FEMY-R7 for 2 weeks eliminated H. pylori from the stomach of mice in a dose-dependent manner, displaying a near-full efficacy at 200 mg/kg/day. In the present study, such a bacteria-eradicating efficacy of FEMY-R7 was confirmed again as analyzed with CLO kits on the mouse gastric mucosa. However, the CLO reaction from mouse feces did not match that of gastric mucosa; i.e., there were several partially-positive reactions in feces of mice that displayed negative reaction in the stomach.
We administered FEMY-R7 to naturally-infected human patients at doses of 1.62, 5.2 or 16.2 mg/kg/day (100, 320 and 1,000 mg/man/day for 60 kg men) to match the doses in mice, according to the body surface area-based dose translation (extrapolation) [36]. Notably, the dose dependency in the CLO reaction from human feces was in parallel with that from mouse feces. More interestingly, the bacterial identification ratios exhibited a good correlation between the matching doses in mice and humans. It was also observed that bacteria was not identified from the feces showing partially-positive reaction in CLO test. Therefore, it is inferred that the partially-positive reaction may be due to the urease enzyme released from dead H. pylori remaining in the stools.
In our recent study, the effectiveness of FEMY-R7 was also confirmed in humans; i.e., daily intake of 300 mg/man/day FEMY-R7 for 8 weeks significantly lowered Delta over baseline-value (BOD) in the expiratory breath in UBT [34]. Although treatment with 300-320 mg/man FEMY-R7 for 8 weeks was not enough to fully eliminate the bacteria in our previous and present studies as analyzed by UBT and feces CLO test, it was confirmed that longer periods (>8 weeks) or higher doses (>320 mg/man) should fulfill the requirement for full clearance of H. pylori from the stomach.
Although triple therapies (for example, omeprazole+clarithromycin+amoxicillin or omeprazole+clarithromycin+metronidazole) consisting of two antibiotics had been recommended as a standard treatment for H. pylori [2], it has been recently demonstrated that the widespread use of antibiotics led to a rapidly-increasing bacterial resistance [24,37]. Thus, there is a strong rationale for the development of novel anti-bacterial agents without resistance and adverse-effects. In the present study, we showed the efficacy of FEMY-R7 in eliminating H. pylori from mice and humans by analyzing the correlations between gastric mucosal and fecal samples from mice as well as between fecal samples from mice and humans. In conclusion, it is suggested that FEMY-R7, a combinational regimen composed of LJE and OBE, could be a promising candidate overcoming tolerance of antibiotics or an adjunct to reduce the dosage of antibiotics for the treatment of recurrent H. pylori infection.
 XML Download
XML Download