

 PDF
PDF ePub
ePub Citation
Citation Print
Print


In peptic ulcers, there are mucosal injuries due to the gastric acid and pepsin, causing depletion of mucin secreted from mucus cells [1,2]. However, gastric erosions and ulcers are caused by various factors such as gastric over-secretion and retention, mucin layer-depleting agents, blood flow disturbances, and inflammation [1,2,3,4]. The ulcer-inducing agents include non-steroidal anti-inflammatory drugs (NSAIDs) that block production of prostaglandins (PGs), leading to mucin depletion and focal ischemia [5,6,7,8,9], alcohols [7,8,10], stresses [4,7,8], gastric retention [7,8], gastric hypermotility and acetic acid accumulation [8,11,12,13,14], and bacterial infection such as Helicobacter pylori [1,2,15,16,17].
H. pylori infection has been found in 70%, 50-60%, and 90% of gastric ulcer, gastritis, and duodenal ulcer patients, respectively. It is well known that H. pylori induce chronic active gastritis as a key factor for recurrence and aggravation of ulcers as well as development to gastric malignancies [18,19,20]. It is believed that H. pylori exacerbates erosions and ulcers by continuously stimulating gastric secretion and retention [21,22]. Accordingly, elimination of H. pylori is a key point for ulcer treatment in adults exhibiting a high incidence [1,2,15,16,17,23].
For the treatment of H. pylori-mediated gastritis and ulcers, triple therapies composed of proton-pump inhibitors (pantoprazole, omeprazole, lansoprazole, etc) and antibiotics (clarithromycin, metronidazole, amoxicillin, etc) have been recommended [2]. However, the antibiotics used for triple therapy are displaying a rapidly-increasing tolerance to H. pylori [24]. Therefore, natural products without tolerance during repeated treatments may contribute to the elimination of the bacteria.
Fucoidans, sulfate polysaccharide complex from seaweeds such as Laminaria japonica and Cladosiphon okamuranus, have been widely used as therapeutics in Oriental medicine. In previous studies, it have been demonstrated that fucoidan has anti-oxidative, anti-coagulative, anti-tumor, and anti-inflammatory activities [25,26]. Accordingly, the beneficial effects of fucoidan on inflammatory diseases, ischemia, immune dysfunction, and tumors are attracting investigators' attention [27,28]. Recently, fucoidan was demonstrated to inhibit the attachment of H. pylori to gastric cells in Mongolian gerbils and in humans [29,30].
It was reported that evening primrose tannins have anti-bacterial activity against H. pylori [31]. In addition, evening primrose extract was demonstrated to inhibit bacterial growth in vitro and blocks adhesion and colonization of H. pylori in the gastric walls [32].
On the basis of anti-H. pylori and anti-inflammatory activities, we investigated the effects of FEMY-R7, a combinational preparation of fucoidan and evening primrose extract, on the in vitro bacterial growth, in vivo bacterial infection, and gastric secretion in comparison with a proton-pump inhibitor pantoprazole.
Materials and Methods
Materials
FEMY-R7 containing fucoidan and evening primrose seed extract (1:1) was obtained from Misuba RTech Co. (Asan, Korea). Fucoidan was extracted with an acid-hot water extraction method at pH 2.0 and 60℃ for 2 hours from Laminaria japonica. The extraction supernatant was neutralized with 10 N NaOH and filtered. After precipitation with ethanol, the filtrate was centrifuged and dried. Evening primrose seeds were defatted and extracted with 60% ethanol. The extract was filtered, concentrated, and dried. The 1:1 (v/v) mixture of fucoidan and evening primrose seed extract, named FEMY-R7, was stored at 2℃ until use.
H. pylori culture and anti-bacterial activity
H. pylori SS1 (ATCC49503) was obtained from American Type Culture Collection (Manassas, VA, USA), and cultured on brain heart infusion (BHI) broth in an anaerobic chamber with 10% CO2, 5% O2, and 85% N2 at 37℃ with enough humidity
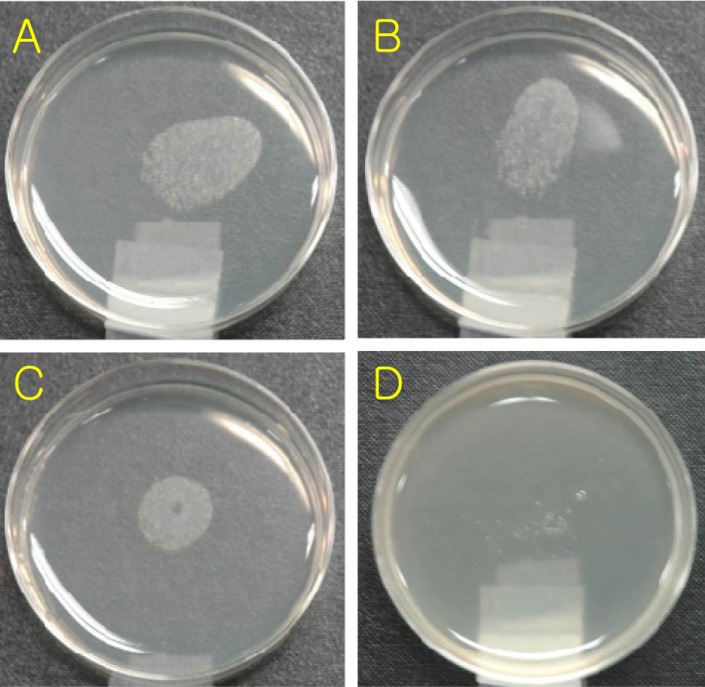
The inhibitory capacity of FEMY-R7 against the growth of H. pylori was assessed using agar-dilution method [33]. In brief, serially-diluted FEMY-R7 (10-100 µg/mL) was added to Mueller Hinton agar containing 10% fetal bovine serum (FBS), and H. pylori was inoculated on the agar. After 3-day incubation at 37℃, the FEMY-R7 concentration fully inhibiting the bacterial growth was determined to be minimal inhibitory concentration (MIC).
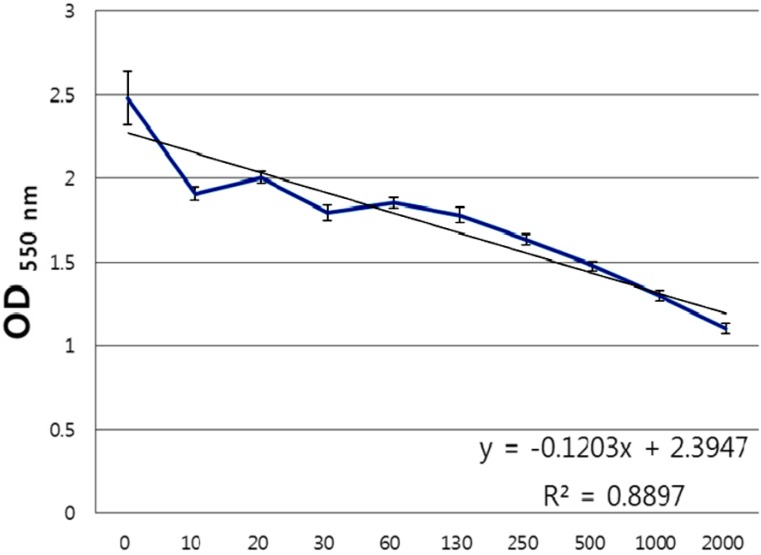
In order to assess in vitro urease inhibition, H. pylori (1×108 CFU/mL) were incubated with FEMY-R7 (10-2,000 µg/mL) at 37℃ under stirring at 50 rpm for 6 hours, and then 50 µL of urea base (2% urea and 0.03% phenol red) was added and allowed to react for 30 min. Urease activity was quantified by measuring the optical density at 550 nm, and was presented as median inhibitory concentration (IC50).
Animals
Male C57BL/6 mice (body weights 25-27 g) and male SD rats (200-220 g) were procured from Daehan Biolink (Eumseong, Korea), and housed in a room with constant environmental conditions (23±2℃; 55±10% relative humidity; 12-hour light-dark cycle; 150-300 lux brightness). Pellet feed and purified water were available ad libitum. All the animal experiments were conducted according to the Standard Operation Procedures (SOP), and approved by the Institutional Animal Care and Use Committee of Chungbuk National University, Korea. For biosafety, the investigators were fully protected with sterilized clothes, masks, and gloves on SOP.
In vivo H. pylori-elimination activity
After 12-hour fasting, the mice (n=10/group) were orally inoculated with H. pylori SS1 (5×109 CFU/1 mL/mouse) 3 times at 2-day intervals, and simultaneously, orally treated twice a day with 10, 30 or 100 mg/kg FEMY-R7 for 7 days.
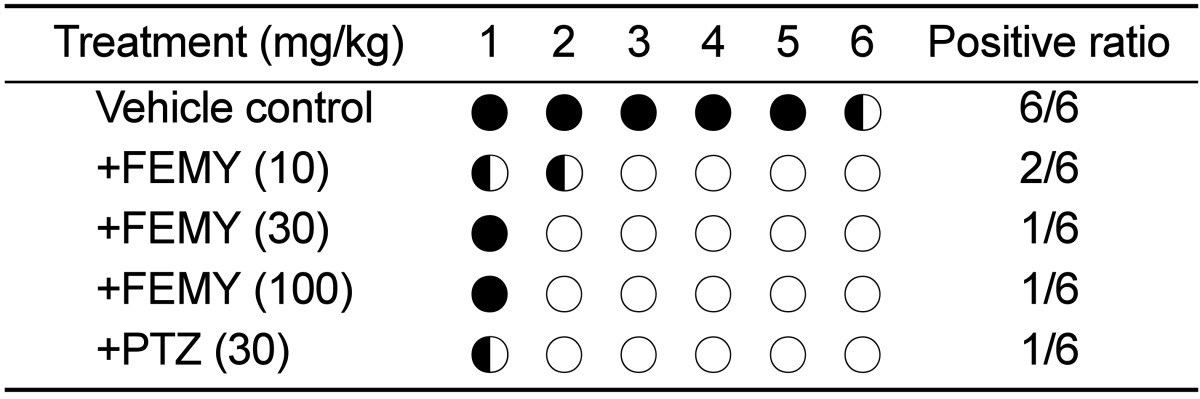
Three hours after the final administration, the mice were sacrificed and their gastric mucosa was biopsied for the detection of H. pylori. The biopsy samples (3×3 cm) from gastric pylorus were minced, applied to Campylobacter-like organism (CLO)-detection kits (Kimberly-Clark, Roswell, GA, USA), and incubated at 35℃ for 24 hours to examine urease activity. The reaction (color change) was determined as negative for bright yellow, false (partially) positive for thick yellow, or positive for thick (dark) red [16,17,33].
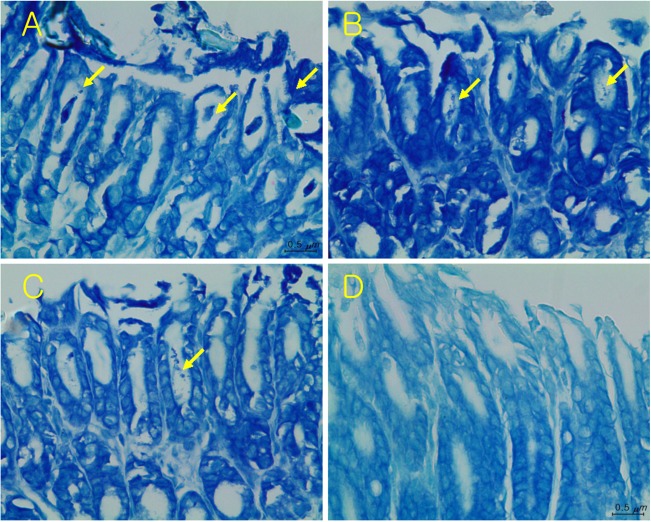
The stomach of mice was removed and fixed in neutral formalin solution. Paraffin-embedded tissue slides were stained with Giemsa, and examined under a light microscope for the observation of bacteria and tissue injury in the gastric mucosa.
In vivo gastric secretion-inhibitory activity
After 48-hour fasting, the rats were orally administrated FEMY-R7 (10, 30 or 100 mg/kg) or pantoprazole (30 mg/kg) in 1% carboxymethylcellulose (CMC), and their pylorus was ligated with a 4-0 silk after median incision of abdomen from xiphoid process under anesthesia with ether [34]. Six hours after pylorus ligation, the rats were sacrificed under deep anesthesia with ether, and their stomach was removed after clamping the esophagus. Gastric fluid was collected and centrifuged at 3,000 rpm for 10 min. The volume and pH of the fluid were measured. Into aliquots (500 µL) of the fluid, Töpfel reagent (1% dimethylaminoazobenzene) or 1% phenolphthalein (10 µL each) were added, and titrated with 0.1 N NaOH solution to measure free HCl and total acidity, respectively [34].
Statistical analysis
Data were expressed as the mean±SEM. Statistical analysis was performed using an analysis of variance (ANOVA) followed by the Dunnett's multiple-range test correction with the aid of SPSS for Windows v.10.0 (Chicago, IL, USA). A P value <0.05 was considered statistically significant.
Go to : 
Results
In vitro anti-bacterial test, 100 µg/mL FEMY-R7 completely inhibited the growth of H. pylori following 3-day incubation with the bacteria (1×108 CFU/mL) with a serially-diluted FEMY-R7, while 30 µg/mL FEMY-R7 slightly decrease the bacterial counts (Figure 1). Therefore, an MIC of FEMY-R7 was determined to be 100 µg/mL. In vitro urease-inhibition assay, FEMY-R7 inhibited urease activity in a dose-dependent manner (Figure 2), in which an IC50 of FEMY-R7 was determined to be 1,500 µg/mL.
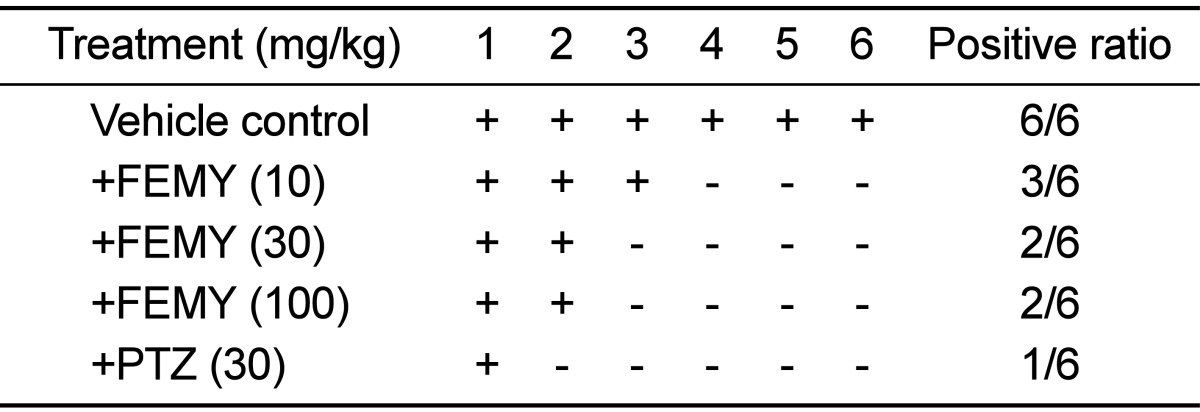
Repeated intragastric inoculation (5×109 CFU/mouse, 3 times) of H. pylori to C57BL/6 mice revealed positive reaction (red color) in CLO test. The mice orally treated with 10, 30 or 100 mg/kg FEMY-R7 twice a day for 7 days displayed positive reaction in 33.3% (2/6), 16.7% (1/6) and 16.7% (1/6) mice, respectively, in comparison with 100% (6/6) positivity in control (vehicle) group (Table 1). On the other hand, 16.7% (1/6) positive reaction was achieved following treatment with pantoprazole (30 mg/kg).
In the gastric mucosa of mice treated only with vehicle, several bacteria were detected in the area of mucosal injury (Figure 3A). In comparison, the detection ratio of bacteria and tissue injury were decreased and attenuated by treatment with FEMY-R7 and pantoprazole (Figure 3B-3D). Quantitatively, treatment with 10, 30 or 100 mg/kg FEMY-R7 displayed the presence of H. pylori in 50.0% (3/6), 33.3% (2/6) and 33.3% (2/6) mice, respectively, in comparison with 100% (6/6) detection in control group (Table 2). By comparison, pantoprazole (30 mg/kg), exhibiting 16.7% (1/6) positivity, was a little bit superior to FEMY-R7 (30-100mg/kg) in the elimination of the bacteria.
After 6-hour pylorus ligation, the gastric juice volume in control (vehicle) group was 11.43 mL/rat (Table 3). The gastric fluid volume was significantly decreased to 8.70 mL following treatment with a low dose (10 mg/kg) of FEMY-R7, while higher doses (30-100 mg/kg) of FEMY-R7 and pantoprazole (30mg/kg) did not significantly affect the gastric secretion. FEMY-R7 lowered total acidity and free HCl at only medium (30 mg/kg) and high (100 mg/kg) doses, respectively. By comparison, pantoprazole significantly increased gastric pH, and reduced both the free HCl and total acidity, indicative of a strong proton pump-inhibitory activity.

Go to :
Discussion
H. pylori is known to secrete urease to survive in acidic environment and invade gastric mucosa, causing gastritis, ulcers, and sometimes development of gastric cancer. In the present research, we demonstrated that FEMY-R7 has anti-bacterial activity against H. pylori with 100 µg/mL of MIC. Also, FEMY-R7 inhibited bacterial urease, in which the IC50 value was about 1,500 µg/mL. These results indicate that the urease-inhibitory activity of FEMY-R7 may not significantly contribute to anti-bacterial effect for inhibition of the bacterial growth.
In CLO test, treatment with FEMY-R7 for 7 days eliminated H. pylori from the stomach of mice, reaching efficacy over 50% at all doses used (10, 30, and 100 mg/kg). It is of interest to note that the effectiveness of FEMY-R7 at 30 or 100 mg/kg was comparable to that of 30 mg/kg pantoprazole, since it is well known that proton-pump inhibitors such as pantoprazole inhibit gastric secretion [35,36], protect parietal cells [7,37,38], and suppress H. pylori growth [39,40,41]. Compared with the results using CLO kits that detect urease activity, the bacterial cells were detected in more mice (Tables 1 and 2); i.e., the partially-positive stomachs in CLO test revealed H. pylori bacteria in Giemsa-stained mucosa (Figure 3). Therefore, it is assumed that some bacteria inactivated or killed not to produce urease may be stained by Giemsa.
The gastric secretion was inhibited at relatively-low doses (10-30 mg/kg) of FEMY-R7, whereas a high dose (100 mg/kg) of FEMY and pantoprazole (30 mg/kg) were ineffective. Notably, pH, free HCl, and total acidity of the gastric juice decreased at different dose ranges of FEMY-R7, but the effects of FEMY were negligible when compared to the excellent antacid activity of pantoprazole (Table 3). These results indicate that FEMY-R7 blocks the adhesion and invasion of H. pylori to mucosal walls by directly killing the bacteria as inferred from the relatively-low MIC. In spite of the high IC50 value in the inhibition of urease, it is believed that the enzyme-inhibitory activity of FEMY may also contributed to the bacterial clearance, because H. pylori is known to neutralize the gastric acid using the enzyme to survive there [42]. Such results and assumption were inferred from previous observations showed that fucoidan and evening primrose extract inhibited the adhesion and colonization of H. pylori to gastric cells [29,30,32].
In fact, in our follow-up studies to assess the effects of FEMY-R7 on the gastric mucosal injury, FEMY-R7 did not considerably attenuate the ulcer lesions induced by water-immersion restraint stress (WIRS), ethanol or indomethacin (an NSAID) (unpublished results). Such results support the conclusion that FEMY-R7 eliminates H. pylori from the gastric walls by killing the bacteria and inhibiting their invasion, but not by preserving or strengthening the mucosal layer including mucus content.
Effective treatment of H. pylori has been provided with triple therapies, for example, omeprazole + clarithromycin + amoxicillin or omeprazole +clarithromycin+metronidazole consisting of two antibiotics, which are still the most effective [2]. However, widespread use of antibiotics has often resulted in the development of resistance [24,43]. These problems indicate the need for the development of novel improved anti-bacterial agents with minimal or without resistance. In the present study, it was found that FEMY-R7 not only inhibited the growth of H. pylori
in vitro, but also eliminated the bacteria from the stomach walls in vivo. Notably, the effect of crude extract of FEMY-R7 was comparable to that of pantoprazole, a purified drug. The results indicate that FEMY-R7 could be a good candidate overcoming tolerance of antibiotics for the treatment of recurrent H. pylori infection.
Go to :
 XML Download
XML Download