

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Exposure and sensitization to indoor and outdoor aeroallergens are consistently associated with the development and persistence of asthma.123 Although the contribution of common aeroallergens, such as house dust mite (HDM), pollen, animal dander and cockroach have been explored in asthmatic patients, relatively few studies have focused on relationships between mold allergen sensitization and asthma morbidity.
Current evidence demonstrates a close association between sensitization to mold and severe symptoms in patients with asthma.456 Exposure to mold is strongly related to severe respiratory symptoms in patients with asthma, and sensitization has been described as a risk factor for life-threatening conditions.78 Previous studies79 have shown that sensitization to mold, particularly Alternaria, is linked to more persistence and severity of asthma. In a previous report,8 20 of 37 (54%) patients admitted to the intensive care unit (ICU) for asthma and had positive skin test results to 1 or more mold allergens compared with 30% of patients not admitted to ICU. However, patients admitted to ICU were no more likely than other patients to have positive results in skin tests for HDM, animal dander, or pollen. A previous study involving children with moderate-to-severe persistent asthma have reported that Alternaria and Aspergillus are allergens most closely associated with development of asthma.5 Sensitization to Alternaria has also been implicated as one of the important risk factors for current symptoms or sudden respiratory arrest in adolescents and young adults with asthma.10
Some studies have demonstrated lower lung function in a small number of mold-sensitized adults11 or patients with asthma.1213 Recently, the greater risk for airway hyper-responsiveness (AHR) was demonstrated in adult Korean asthmatics with a higher response to Alternaria.14 A few studies have indicated that mold sensitization is positively correlated with asthma severity in terms of decreased lung function in pediatric patients.515 Thus, the effect of mold sensitization on airway inflammation and lung function in asthma is unclear in pediatric asthma.
The identification of factors associated with airflow limitation in children with asthma is necessary for proper management and prevention of asthma exacerbation. We hypothesized that the clinical feature and lung function may be different among asthmatic children, who are sensitized to mold, compared to those who are sensitized to other aeroallergens. The aims of this study were to determine the prevalence of allergic sensitization to mold and to assess its relationship to lung function and AHR among asthmatic children.
Go to : 
MATERIALS AND METHODS
Study subjects
We retrospectively reviewed clinical data from asthmatic subjects who attended the Allergy Clinic of Korea University Anam Hospital, Seoul, between July 2005 and June 2015. We selected subjects who met clinical diagnostic criteria of asthma. When the subjects visited our clinic, they underwent spirometry, blood test, methacholine test, and skin prick testing (SPT) as a routine practice. If subjects met clinical diagnostic criteria of asthma, we included them in the study. Subjects who had typical symptoms suggestive of asthma, such as a history of episodic wheezing and/or dyspnea and reversible airflow obstruction (an increase in forced expiratory volume in 1 second [FEV1] ≥12% after bronchodilator administration) and/or methacholine PC20 <16 mg/mL were included. Subjects with a history of near-fatal asthma, major exacerbations necessitating the use of systemic corticosteroids, or other respiratory diseases were excluded from the study. In cases where testing had been conducted on multiple occasions, the earliest results were used. Finally, 551 subjects' medical records were reviewed. The subjects were divided into 3 groups according to the SPT results: 1) those who did not show positive results to any aeroallergens (group 1, non-sensitized), 2) those who were sensitized to aeroallergens other than mold (group 2, other allergen-sensitized), and 3) those who were sensitized to mold (group 3, mold-sensitized). The study protocol was approved by the Institutional Review Board of the Korea University Anam Hospital (No. AN16013-001).
Data collection
The following clinical data were collected: sex, age, body mass index (BMI), and blood test results, such as serum total immunoglobulin E (IgE), eosinophil cationic proteins (ECP), and blood eosinophil counts. Serum total IgE levels measured using a Coat-A-Count Total IgE IRMA (Diagnostic Products Co., Los Angeles, CA, USA) according to the manufacturer's instructions. The number of peripheral blood eosinophils was counted using an automated hematology analyzer (Coulter Counter STKS; Beckman Coulter, Fullerton, CA, USA). Serum ECP levels were measured using a commercially available immunoCAP system (ThermoFisher, Uppsala, Sweden). The prevalence of comorbid atopic dermatitis, rhinitis, and sinusitis were determined by the subject's symptoms and the physician's assessment. The diagnosis of atopic dermatitis was based on the criteria of Hanifin and Rajka.16 The diagnosis of rhinitis was made based on the subject' history and rhinologic examination. They had recurrent symptoms of sneezing, rhinorrhea, and nasal stuffiness or itching apart from common cold during the previous year. Sinusitis was diagnosed by the presence of 2 or more following symptoms lasting at least 10 days; anterior and/or posterior mucopurulent drainage, nasal congestion/blockage, cough, facial pain/pressure/dullness, or a reduced/absent sense of smell.
Pulmonary function tests
Spirometry data were collected as part of routine practice for all asthmatic subjects, using a computerized 1022 digital spirometer (VIASYS, Palm Springs, CA, USA). Pulmonary function data, such as FEV1, forced vital capacity (FVC), and their ratio (FEV1/FVC) were collected which were measured in accordance with the recommendation of the American Thoracic Society.17 The best of 3 technically acceptable readings was used for analysis.
Methacholine challenge tests
Bronchial challenge test data were collected, which were carried out using a modification of the method described by Chai et al.18 Methacholine challenge was done only when subject's baseline FEV1 ≥70% predicted value due to the ethical problem. Fresh solutions of methacholine were diluted with saline at concentrations ranging from 0.075 to 50 mg/mL. Solutions were delivered using a nebulizer (model 646; Devilbiss Healthcare, Somerset, PA, USA) with air pressurized using a dosimeter (KoKo DigiDoser; nSpire Health, Louisville, CO, USA). Each subject inhaled five inspiratory capacity breaths of saline diluted solution and increasing concentrations of methacholine at 5-minute intervals. FEV1 was measured 90 seconds after inhalation at each concentration of methacholine. Methacholine PC20 was calculated by interpolating between 2 adjacent data points when a subject's FEV1 decreased by >20% from baseline. Methacholine challenge test was performed within 4 weeks after first visit when the subject was free from acute respiratory tract infection and asthma exacerbation. Inhalation of short-acting β2-agonists was discontinued for at least 8 hours, and inhaled corticosteroid, long-acting β2-agonists and leukotriene modifier were discontinued for at least 3 days before tests. Administration of antihistamines and systemic steroids was also prohibited 7 days prior to the tests.
Measurement of fractional exhaled nitric oxide (FeNO) concentrations
The FeNO data were also collected which were measured using a NIOX MINO analyzer (Aerocrine AB, Solna, Sweden). The sampling flow rate was 50 mL/sec. To measure FeNO, subject inhaled fully to total lung capacity and then immediately exhaled slowly to residual volume into a wide-bore analyzer. The pressure during expiration was kept constant using pressure and volume sensors in the analyzer.
Skin prick testing
Allergen sensitization was assessed by using SPT for common aeroallergens, including HDM (Dermatophagoides pteronyssinus, Dermatophagoides farinae), animal dander (cat, dog), pollen (oak, alder, ragweed, mugwort, rye grass), cockroach, and mold (Alternaria alternata, Aspergillus fumigatus). Briefly, tests were performed on the volar surface of the forearm, and wheal size was recorded at 15 minutes as the biggest diameter. The result was considered positive if the mean of 2 perpendicular diameters across the wheal was at least 3 mm and greater than that of the negative control. Sensitization was defined as the presence of at least 1 positive reaction to these allergens.
Statistical analysis
Data are presented as mean±standard deviation (SD). Serum total IgE levels, serum ECP levels, blood eosinophil counts, FeNO and methacholine PC20 were log transformed before statistical analysis. Differences between the 3 sets of data were tested using one-way analysis of variance (ANOVA). If the one-way ANOVA result was found to be statistically significant, then bivariate comparisons between 2 of the 3 groups were also reported using the Tukey test. Statistical analysis was performed with SPSS 20 for Windows (SPSS Inc., Chicago, IL, USA). A P value of <0.05 was considered significant.
Go to :
RESULTS
Allergen sensitization results
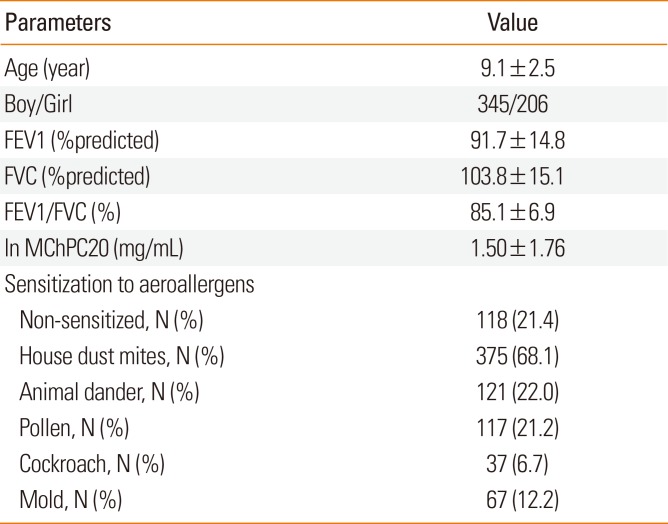
Table 1 shows clinical characteristics and sensitization rates of the study subjects. Mean (±SD) age was 9.1±2.5 and boys were 62.6%. Among the 551 asthmatic subjects, 433 (78.6%) showed a positive response to at least 1 aeroallergen and 118 (21.4%) were found to be non-sensitized. The most commonly sensitized aeroallergen was HDM (n=375, 68.1%) and followed by animal dander (n=121, 22.0%), pollen (n=117, 21.2%), and cockroach (n=37, 6.7%). Sixty-seven subjects (12.2%) were sensitized to mold. Among them sensitization to Alternaria (n=63, 94.0%) were much higher than to Aspergillus (n=19, 28.4%). The prevalence of mold allergen sensitization appeared to be increased with age but statistical significance was not reached (Fig. 1A and 1B).
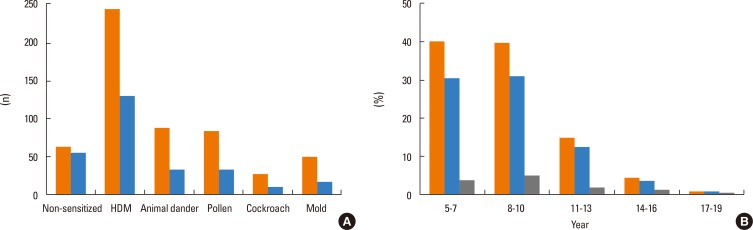 | Fig. 1Sensitization profiles in asthmatic subjects by sex (left bar: boy, right bar: girl) (A). The prevalence of sensitization to any aeroallergen (center bar) and mold (right bar) by age group among the total asthmatic children (left bar) (B).
|
Table 1
Clinical characteristics and sensitization rates of study subjects
![]()
Clinical characteristics
The clinical characteristics of the 3 groups are listed in Table 2. There was no significant difference in terms of age, sex, or body mass index (BMI) between the 3 groups. The log mean serum total IgE levels were higher in groups 2 (5.96±1.14 IU/mL) and 3 (5.81±0.97 IU/mL) than in group 1 (3.88±1.68 IU/mL). The log blood eosinophils were significantly higher in groups 2 (1.43%±0.97%) and 3 (1.49%±0.75%) than in group 1 (0.70%±0.94%), but the difference was not statistically significant between the groups 2 and 3. The serum ECP levels showed similar results. The concentrations of FeNO were significantly higher in groups 2 (3.12±0.40 ppb) and 3 (3.22±0.38 ppb) than in group 1 (2.85±0.44 ppb) (P<0.001 for each), but the difference was not statistically significant between groups 2 and 3.
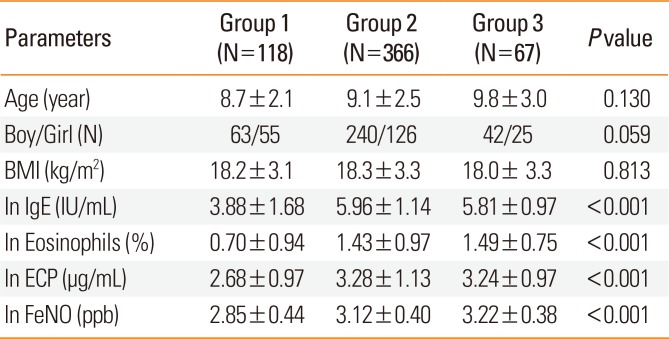
Table 2
Clinical characteristics of the 3 groups classified according to the sensitization profile
![]()
Pulmonary function parameters and AHR
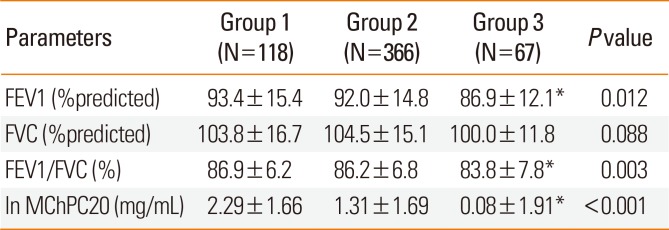
The mean±SD of FEV1 levels were significantly lower in group 3 (86.9±12.1%pred) than in groups 2 (92.0±14.8%pred, P=0.015) and 1 (93.4±15.4%pred, P=0.010) (Table 3, Fig. 2A). The mean ±SD of FVC levels were not significantly different between the 3 groups (P=0.088) (Fig. 2B). Whereas the mean ± SD of FEV1/FVC was significantly lower in group 3 (83.8%±7.8%) than in groups 2 (86.2%±6.8%, P=0.022) and 1 (86.9%±6.2%, P=0.003) (Fig. 3A). Group 3 had a significantly lower log mean ± SD of methacholine PC20 (0.08±1.91 mg/mL) than groups 2 (1.31±1.69 mg/mL, P=0.007) and 1 (2.29±1.66 mg/mL, P=0.001) (Fig. 3B). Differences in FEV1, FEV1/FVC, and methacholine PC20 remained significant when comparing group 2 to group 3.
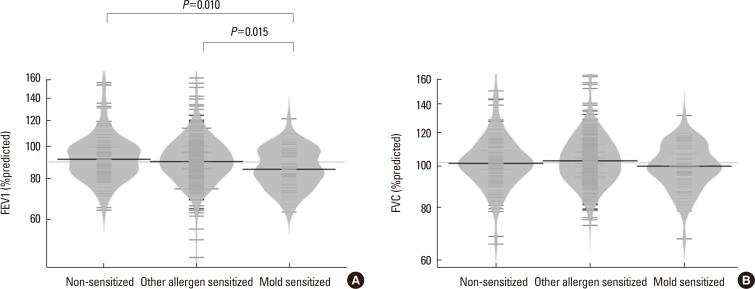 | Fig. 2The FEV1 %predicted values (A) and FVC %predicted values (B) of asthmatic subjects with non-sensitized, other allergen-sensitized and mold-sensitized.FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
|
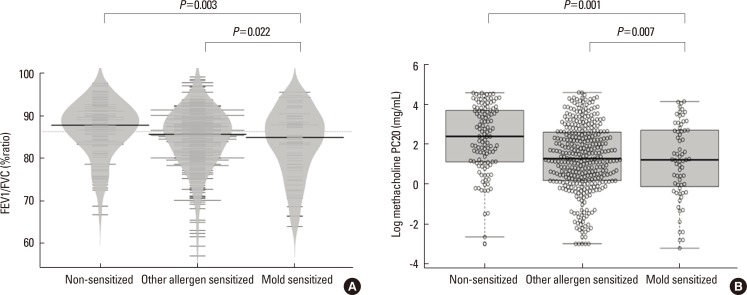 | Fig. 3The FEV1/FVC ratio (A) and log methacholine PC20 levels (B) of asthmatic subjects with non-sensitized, other allergen-sensitized, and mold-sensitized.FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity.
|
Table 3
Pulmonary function parameters of the 3 groups
Data are expressed as mean±SD. Group 1, non-sensitized; Group 2, other allergen-sensitized; Group 3, mold-sensitized.
FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; MChPC20, provocative concentration of methacholine causing a 20% decline in FEV1. *P<0.05 compared to Group 2 by the post-hoc test.
![]()
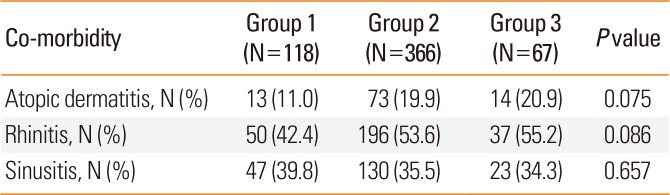
Comorbidities
The prevalence of comorbid allergic diseases in the asthmatic subjects was also analyzed. The most common allergic disease in all 3 groups was rhinitis (Table 4). In the comparative analyses of the prevalence of comorbidities between the groups, the prevalence of atopic dermatitis and rhinitis appears higher in groups 2 and 3 compared to group 1, but the difference was not statistically significant among the 3 groups. There was no significant difference in the prevalence of atopic dermatitis and rhinitis between groups 2 and 3. The prevalence of sinusitis did not differ between the 3 groups.
Go to :
DISCUSSION
This is the first study that shows the prevalence of sensitization to mold and its relation to lung function in a large number of Korean children with asthma. In the present study, we found that asthmatic children with sensitization to mold more likely have lower lung function than those without. Furthermore, mold-sensitized asthmatic children showed increased AHR than the other groups of children. Our results suggest that sensitization to mold may be associated with lower lung function and increased AHR in children with asthma.
In the present study, almost three-fourths of asthmatic subjects were sensitized to aeroallergens. Boys had more sensitization to aeroallergens including mold than girls. Of the asthmatic subjects, 12.2% were sensitized to mold allergens. The precise prevalence of mold sensitization in patients with asthma is difficult to establish due to the use of unstandardized extracts and different methodologies. The rates of sensitization in individuals attending allergy clinics range from 5% to 20%.19 In our asthmatic subjects, the prevalence of mold sensitization is comparable with that of a European study with a large population which showed that 19% of the respiratory allergic patients, aged 3–80 years, reacted to at least 1 mold extract by SPT.20 Bartra et al.21 revealed an 18.3% of positive SPT responses to Alternaria species among the children and adults with allergic rhinitis and asthma. Our data were also comparable to the prevalence of mold sensitization in Korean children with allergic rhinitis22 which was 12.4% and that was much higher in general Korean pediatric population (6.1%).23 In the present study, most of the mold SPT-positive subjects had Alternaria sensitization (94.0%), and fewer subjects were sensitized to Aspergillus (28.4%). In a recent study, conducted in the New York area, similar climatic characteristics as Seoul, most commonly implicated species in mold-sensitized patients were found to be Aspergillus (84%) and Alternaria (72%).5 It has been demonstrated that Alternaria, Aspergillus, and Cladosporium are the most commonly sensitized species in asthmatic patients; however, exact estimation of the relative importance of individual mold might be difficult.81120
Previous studies have shown that exposure to mold increases the development and exacerbation of asthma in mold-sensitized patients.2425 Positive SPT results to mold allergens have been found to be a significant risk factor of asthma, and asthma predisposes to sensitization to inhaled mold spores. Exposure to mold is not always consistent with the sensitization rate. Molds may generally have a lower sensitization rate than other aeroallergens, though indoor molds are present through the year.26 Sensitization to mold occurs in a small proportion of cases only, even in people who have been exposed to mold at workplaces.27 This may indicate that commercially available mold skin testing panels cannot cover all mold species exposed in the environment and that unknown mechanisms other than the IgE-mediated process are involved in mold sensitization.27
Although many previous studies and our study revealed HDM to be a major allergen associated with asthma, relatively little attention has been paid to sensitization to mold, which may be associated with severe and chronic asthma. Thus far, the role of mold as a primary exogenous driver of severe asthma has been incompletely explored. Halonen et al.28 have documented that severity of asthma is strongly linked to Alternaria skin test positivity. Recently, mold sensitization has also been linked to asthma morbidity in inner-city children.9 Given inner-city housing conditions, such as poor ventilation, leaks, unsunny days that might potentiate problems related to indoor allergens, mold could be particularly important determinant of asthma morbidity for children living in these areas.9 In the present study, asthmatic subjects who were sensitized to mold had significantly lower lung function compared to those who were not. Although we could not show a causal-effect relationship between mold sensitization and the severity of asthma in the present study, our findings are comparable with those of the previous study which demonstrated that sensitization to mold may be associated asthma severity and chronicity in children and adults. Stern et al.29 reported that sensitization to Alternaria at the age of 6 years correlated with persistent asthma at the age of 22 years. The European community respiratory health survey26 on the relative importance of sensitization to individual allergens in asthma severity showed significantly increased asthma severity in mold-sensitized asthmatic patients, but not in other allergen-sensitized, such as cats or pollens. Nearly 10% of near fatal asthma patients were reported to be sensitized to Alternaria and they were relatively young and less responsive to bronchodilator treatment.7 In the present study, since we did not explored how sensitization to individual mold correlates with low lung function, we could not show the association of asthma severity with individual mold allergen. However, it is clear that sensitization to mold related to severity in asthma regardless of the species.30
Sensitization to mold is associated with severe asthma; however, a few studies in which the severity of asthma related to mold sensitization has been defined by airflow limitation in children have been conducted so far. It would be interest to investigate mold-associated asthma with respect to asthma severity based on airflow obstruction or increased AHR. Our findings of a positive association between sensitization to mold and lower lung function/increased AHR in pediatric asthmatic subjects were comparable to those of Jo et al.'s study14 in adult asthmatics. In that study, they found an increased risk for AHR in patients with higher responses to Alternaria on SPT.
Mold is very common in the environment, and respiratory exposure to airborne spores is almost constant. It is not known why certain mold allergens would produce more severe airway disease than other common aeroallergens. One plausible explanation for this may be that other aeroallergens, such as HDM, pollen, or animal dander are the sources of allergenic protein, whereas mold has additional ability to actively germinate and colonize in the respiratory tract.31 Thus, it is possible that mold has a much greater impact on an individual in triggering host defense against pathogens and producing enzymes that may play an accessory role in triggering allergy.31 Allergen proteins produced by mold are typical ones that might be generated in large amounts during germination on the respiratory epithelium. Particle size is also important to induce airway inflammation and constriction.26 Possibly, since the small fragments of mold spores are of respirable size, they can reach the lower airways to induce airway inflammation and obstruction.26 Exposure to mold allergens in the sensitized patients may exacerbate asthma symptoms by promoting airway inflammation, airflow limitation, and AHR.323334 A recent study in Korea has shown that sensitization to aeroallergens induce the development of AHR, but not through airway eosinophilic inflammation in mold-sensitized adult asthmatics.14 In the present study, the findings that eosinophilic inflammatory markers in the mold-sensitized subjects were not different from the other aeroallergen-sensitized subjects, could explain that another pathway rather than eosinophilic inflammation induce airflow limitation and AHR in mold-sensitized asthmatics. In a previous study with adult asthmatic patients, Aspergillus sensitized asthmatics showed reduced lung function and increased neutrophilic airway inflammation compared to the Aspergillus non-sensitized asthmatics.12 However, sputum eosinophils were not different between the 2 asthma groups, suggesting a Th1- or Th17-mediated immune response might be involved. In addition, blood eosinophil markers in the present study rather than airway eosinophils may not exactly reflect the presence of airway inflammation.
We observed a differential association between mold/other aeroallergens and severity of asthma. Since, clinical data in the present study were collected consecutively rather than in a randomized fashion, decreasing the possibility of the selection bias risk in asthmatic children sensitized to mold with poor lung function compared to in those not sensitized to mold with high lung function. In addition, evaluation of sensitization status by SPT rather than measurement of serum IgE levels in all asthmatic subjects raised the possibility of reflecting actual responses to allergens.
Several limitations of our study have to be discussed. Firstly, we did not examine any association between exposure and sensitization to mold. Since this study is of retrospective design, we failed to find exact individual exposure to mold allergen. Secondly, some of our subjects in the mold-sensitized group were sensitized to other aeroallergens simultaneously. Thus, we could not exclude the effect of common aeroallergens other than mold in this study. Finally, we had no data on the effects of sensitization to individual mold species, and we had SPT results only for Alternaria and Aspergillus, though they are the most prevalent mold allergens in Korea.
We observed current sensitization status to common aeroallergens, including mold, and showed airflow limitation and increased AHR in pediatric subjects with asthma. Our data from large number of asthmatic children living in inner-city demonstrated that the severity of asthma assessed by lung function and AHR were associated with sensitization to mold, but not to eosinophilic inflammation. Long-term prospective studies of the relationship between personal exposure, sensitization and asthma severity are warranted. Our results suggest that sensitization to mold in asthmatic children may be associated with a decrease in lung function and an increase in AHR. Thus, analy-sis of mold sensitization may become important in the evaluation and management of children with persistent and severe asthma. Targeted environmental intervention should be considered for selected children in avoiding of severe and persistent asthma.
Go to :
 XML Download
XML Download