

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cow's milk allergy (CMA) is the most common food allergy among infants in Europe, with prevalence rates estimated in the range of 2% and 3%.1 Although previous reports stated a good prognosis with a high rate of spontaneous resolution,23 recent studies suggest varying results (13%-37%) to the rate of resolution during childhood.14
The accepted management of CMA is the total avoidance of milk to prevent adverse reactions, which can be life-threatening.56 Nevertheless, milk exclusion involves a wide dietary restriction, which leads to negative nutritional, social, psychological, and economic consequences.7 Moreover, because of cow's milk (CM) ubiquity, avoidance cannot be always guaranteed, and accidental reactions may occur.8 For this reason, CM oral immunotherapy (OIT) appears as a promising approach for CMA treatment.9 As in any other food OIT protocol, CM-OIT starts with administration of milk at very low doses, which are increased up to the usual intake (around 200 mL). Thereafter, it is given daily in a maintenance dosage.10 The main goal of CM-OIT is to increase the threshold dose which triggers symptoms, protecting patients against reactions on accidental exposure. In addition, it allows the inclusion of milk in the patient's diet, with the subsequent benefit in nutrition and quality of life.
Previous studies on CM-OIT have shown desensitization rates of 36%-92% after a wide array of protocols.11 However, there is still a lack of sufficient evidence regarding long-term efficacy, safety, impact on quality of life, and cost-effectiveness of these procedures. Thus, CM-OIT is considered nowadays an experimental treatment not ready yet for clinical practice.1213
Currently, there is little knowledge regarding immunological changes and mechanisms subjacent to CM-OIT. So far, the different studies performed have highlighted an increase in the levels of allergen-specific IgG4 after successful CM-desensitization.14151617 Nevertheless, in cases of the allergen-specific IgE response, the results are somehow controversial.17181920 Although these observations clearly indicate immune-deviation, to the best of our knowledge, there is only 1 report available characterizing the T-cell response of milk allergic patients before and after a CM-OIT protocol.21
The objective of this study was to evaluate the safety and efficacy to induce clinical desensitization to CM of an OIT protocol in a pediatric population with CMA. In addition, with the aim of adding some insights into the immunological mechanisms subjacent to CM-OIT, the immune responses against β-casein, one of the main milk allergens, of Peripheral Blood Mononuclear Cells (PBMCs) from CMA patients before and after the protocol were evaluated. For that purpose, a panel of cytokines covering Th1, Th2, and Treg responses, together with allergen-specific IgE and IgG4 levels were assessed. For comparison, a population of nonallergic donors from the same age-range was included in the study.
MATERIALS AND METHODS
Ethics statement
All human samples/procedures were obtained/performed with written consent from the next of kin, caretakers, or guardians on behalf of the minors/children involved in the study. The Bioethics Committees from Consejo Superior de Investigaciones Científicas and Hospital Universitario La Paz (Madrid, Spain) approved all experiments.
Patient selection
Subjects were recruited from the Allergology Service at Infanta Sofia Hospital (Madrid, Spain). All the children enrolled in the CMA group were patients diagnosed through a compatible clinical history, positive skin prick test (≥3 mm of negative control) and positive CM-, casein- (CN), α-lactalbumin (α-La)-, and/or β-lactoglobulin (β-Lg)-specific IgE. In addition, all the subjects had experienced a positive reaction during a single blind food challenge (SBFC) with commercial semi-skimmed ultra-high temperature-treated (UHT) pasteurized CM (3.3% protein) the month before the beginning of the study. A group of nonallergic children, with no detectable IgE against a broad panel of the most common allergens, was also included in the study.
CM-OIT protocol
The protocol was carried out at the Allergology Day Unit of the Infanta Sofía Hospital, under the direct supervision of the medical and nursing staff, and with all the equipment and material required for the treatment of possible allergic reactions that could occur during the procedure. The CM-OIT protocol was performed with commercial semi-skimmed UHT CM, as described in Table 1. The starting dose of the protocol was the previous one to the highest tolerated dose during the SBFC. Once the patients were able to tolerate 4 mL of undiluted CM without symptoms, an open challenge with baked goods containing milk was performed. Similarly, after tolerating 10 mL, patients were challenged with milk-containing cold meat, with milk chocolate after 15 mL, liquid fermented milk (Actimel®) after 60 mL, yogurt after 100 mL, cow's cream cheese after 120 mL, and finally with goat and ewe's milk cheeses after 200-240 mL. Between visits, patients were advised to daily ingest at home the maximum dose tolerated during their last visit to the unit. When needed, premedication with oral antihistamines was given to patients who developed adverse reactions during the protocol, in order to control the symptoms. Reaction severity was assessed according to Clark and Ewan.22 In cases of moderate reactions, these were pharmacologically treated and the protocol was restarted in the following week at the previously tolerated dose. Hence, the length of the protocol was increased stepwise depending on the severity of the reactions experienced by each patient. In cases of repeated severe reactions (anaphylaxis), the desensitization protocol was interrupted. Patients were considered to have successfully completed the protocol if they were able to tolerate a minimum of 200 mL of CM in less than 24 months.
Once the patients completed the OIT protocol, they maintained, during 1 year, a daily ingestion of 200 mL of commercial semi-skimmed UHT CM. If after 1 year the clinical desensitization was sustained, the patients were authorized to have a non-restricted diet.
Measurement of serum allergen-specific IgE and IgG4
Blood samples were withdrawn from the control subjects included in the study and from the allergic patients before and after the OIT protocol was finished, and sera were analyzed for specific-IgE to CM, CN, α-La, and β-Lg, and CN-specific IgG4 using the Phadia ImmunoCAP-System FEIA (Thermo Fisher Scientific, Barcelona, Spain).
In vitro stimulation of PBMCs
PBMCs were isolated by density-gradient separation (Ficoll-Paque PLUS; GE Healthcare, Barcelona, Spain) from heparinized venous blood. PBMCs (2×106 cells/mL) were cultured in vitro for 7 days at 37℃ in 5% CO2 with medium alone (AIM-V, Biowest, Nuaillé, France), as negative control, or 200 µg/mL of β-casein (Sigma, St. Louis, MO, USA), with a lipopolysaccharide (LPS) level <0.4 ng/mg, as quantified by the Pierce LAL Chromogenic Endotoxin Quantitation Kit (Thermo Scientific, Waltham, MA, USA). Phytohemagglutinin (PHA) (4 µg/mL; Sigma) was used as positive control.
Cytokine profile analyses
After 7 days of culture, levels of IL-5, IL-13, IL-10, IFN-γ, and TNF-α in supernatants were analyzed by a multiplex bead assay (BD cytometric bead array; BD Biosciences, San Diego, CA, USA), according to the manufacturer's instructions. Cytokine secretion was correlated to the standard of each of the human cytokines (0-2,500 pg/mL). The Gallios™ flow cytometer (Beckman Coulter, Barcelona, Spain) was used to acquire data, which were analyzed by Beckman Coulter Kaluza and FCAP Array v3 (BD Biosciences) Software. Results are expressed as the amount of each cytokine detected after the stimulation with β-casein minus the amount detected after stimulation with the negative control.
Quantitative real-time PCR
Total RNA from the PBMCs cultured for 7 days was extracted using the Total RNA Isolation NucleoSpin® RNA II Kit according to the manufacturer's instructions (Macherey-Nagel, Duren, Germany). The RNA template was qualitatively assessed and quantified using an Agilent 2100 Bioanalyzer (Agilent Technologies, Palo Alto, CA, USA) and a NanoDrop ND1000 instrument (Thermo Fisher Scientific), respectively. Reverse transcription reactions were performed following the manufacturer's instructions with the Transcriptor First Strand cDNA Synthesis Kit (Roche, Manheim, Germany). RT-qPCR was performed in a ViiA™ 7 Real-Time PCR System (Applied Biosytems, Foster City, CA, USA) using a total of 6 ng of transcribed cDNA and TaqMan® Gene Expression Assay for the transcription factors: GATA3 (Human Assay ID Hs00231122m1), T-bet (ID Hs 00203436m1), and FoxP3 (ID Hs01085834m1), according to the manufacturer's recommendations. The hypoxanthine guanine phosphoribosyl transferase (HPRT) ID Hs02800695m1 was used as a reference gene. The amplification program used was: 1 cycle of 10 minutes at 95℃, 40 cycles of 15 seconds at 95℃, and finally 1 cycle of 1 minutes at 60℃. All reactions were performed in triplicate. The mean value of the replicates for each sample was expressed as the quantification cycle (Ct). The relative gene expression values (RQ) were calculated using the delta delta CT method. RQ of more than 2 or less than 0.5 was established to be considered relevant.
Statistical analysis
Statistical analyses were performed using the GraphPad Prism 5 software (San Diego, CA, USA). The nonparametric Mann-Whitney test was used to compare between the groups, and the Wilcoxon t test was used to analyze differences between variables during OIT protocol. Results are presented as mean±standard error of the mean (SEM) unless indicated. Differences were considered significant at the 95% confidence level.
RESULTS
Study population and CM-SBFC
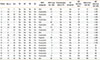
Twenty allergic children (7 females and 13 males) aged between 1.5 and 11 years (mean 4.3 years) and 15 nonallergic children (8 females and 7 males) aged between 5 and 14 years (mean 8.7 years) were enrolled in the study (Table 2). There were not statistically significant differences regarding sex or age between any of the groups. Fifty-five percent of the CMA patients were allergic to other foods. Also, 45% of them had a past or current history of atopic dermatitis, 40% of asthma, and 30% of allergic rhinitis (Table 2). The baseline average specific IgE levels of the allergic group were 27.38 kU/L [0.4-100 kU/L] for CM, 26.45 kU/L [0.1-100 kU/L] for CN, 20.53 kU/L [0.1-94.1 kU/L] for α-La, and 14.18 kU/L [0.5-82.3 kU/L] for β-Lg.
During the SBFC, the median threshold dose resulting in an allergic reaction was 4.0 mL (0.1-120 mL), with 60% of the patients developing anaphylaxis and 30% skin-related reactions (Table 2).
OIT protocol
Among the 20 patients included in the study, 14 (patients 1 to 14 in Table 2) tolerated more than 200 mL of CM, as well as goat's and ewe's milk cheeses, in an average period of 18.9 months (interval: 6-24 months), with 27.8 visits to the clinic of (interval 10-46 times). Fifty-seven percent of them experienced mild dermatologic reactions during the desensitization protocol, with the most common symptoms being mouth itching and perioral erythema. Immunological changes associated with the OIT protocol were only assessed in these patients.
Four patients (patients 15 to 18 in Table 2) tolerated between 35 and 80 mL of CM after 24 months of treatment and 40 visits (interval 32-48 times) to the clinic, on average. At the end of the 24 months period, established as a time limit, this group was able to consume bakery, cold meat, and milk chocolate without developing adverse reactions. The reactions during desensitization of this particular group of patients were more severe, reporting strong abdominal pain and anaphylactic reactions. Two patients (patients 19 and 20) discontinued the study due to parental decision.
Immunological changes after the OIT protocol
As depicted in Fig. 1A, in patients that successfully completed the CM-OIT protocol (n=14) a significant (at least 4-fold), drop in their CM, α-La, β-Lg, and CN-specific IgE levels was detected once the protocol was finished. Moreover, a significant increase from baseline was reached in the serum casein-specific IgG4 concentration after the CM-OIT treatment (Fig. 1B).
Regarding the cellular response, a marked decrease in IL-13, IL-5 and IL-10 (statistically significant for IL-13 and IL-10) production by PBMCs upon β-CN stimulation was observed when comparing initial and post-OIT levels (Fig. 2). Th1 cytokines, IFN-γ, and TNF-α were not detected. Interestingly, the baseline significant differences observed between allergic and nonallergic children in IL-13 and IL-5 levels were no longer found once the protocol had finished (Fig. 2A and B). IL-10 production by β-CN-primed PBMCs from nonallergic donors was significantly higher (P<0.01) than that from CMA patients at the end of the protocol (Fig. 2C).
Analysis of the expression levels of the transcription factors Foxp3, GATA3, and T-bet in the successful patients (n=14), before and after the CM-OIT protocol, did not show any changes, with RQ values of 1.25 for FoxP3, 1.48 for GATA3, and 1.92 for T-bet.
DISCUSSION
In the present study, CM-desensitization (corresponding to tolerance to at least 200 mL of CM) was achieved by 70% of the children with IgE-mediated CM allergy initially included in the CM-OIT protocol. The desensitization rate was in the range of previous reports by González-Jiménez et al.,23 Vázquez-Ortiz et al.24, and Meglio et al.,25 where 72%, 71.6%, and 71.4%, respectively, of the children enrolled were desensitized to CM. A distinct feature of the reported protocol is the progressive introduction of milk-containing foods into patients, diet: this allowed food diversification and helped improve their quality of life while reducing the withdrawals from the therapy as they felt confident with the results of the intervention. It should be mentioned that children seemed to be not only desensitized to CM, but also to goat's and ewe's milk proteins. Several case reports on allergy to goat and sheep milk proteins in individuals previously desensitized to CM can be found in the literature.2627 In fact, Rodríguez del Río et al.28 found, in patients who tolerated CM after CM-OIT, that 26% of them were still allergic to goat's milk and ewe's milk, with 47% of the positive oral food challenges graded as anaphylactic reactions.
Adverse reactions were usually controllable with a rate of occurrences lower than those reported in other CM-OIT protocols.293031 In any case, the side effects encountered during the treatment considerably lengthened the duration of the protocol, compared to what was originally planned, highlighting the importance of adapting the dosing regimen to the patient's response to the therapy. Similar results have recently been observed in the course of an egg-OIT protocol, which had to be increased in approximately 9 months in relation to the original desensitization schedule.32 It is worthwhile to mention that some studies have documented that prolonged OIT treatments enhance the desensitization effect, suggesting that longer treatment courses are more effective and possibly safer.313334
Due to the length of the protocol and the strong familiar commitment required for CM-OIT, the study was open-label and uncontrolled. However, the high baseline specific-IgE levels, as well as the adverse reactions observed during the therapy, suggested that spontaneous CMA resolution was very unlikely in the population under study.353637 The absence of a placebo group is justified by the results obtained in the placebo-controlled trials performed by Skripak et al.17 and Longo et al.,18 in which none of the children included in the placebo group achieved even partial tolerance once the study had ended. In cases where the treatment applied had altered the natural course of CM-oral tolerance achievement, the authors would have either anticipated it or increased the threshold dose for patients that did not successfully complete the therapy.3138 While the current protocol setting cannot confirm whether patients were tolerant as CM was not withdrawn for ethical reasons, it should be noted that all the patients considered successfully desensitized were on a free diet 1 year after the OIT protocol had ended.
Baseline specific-IgG4 levels increased after the therapy, as previously observed by a number of authors in other CM-OIT protocols,11141517 as well as in patients who spontaneously recovered from CMA,1639 confirming the important role of this immunoglobulin in oral tolerance establishment. Concomitant with the increase in specific-IgG4, significantly reduced antigen-specific-IgE production was found. Although a decrease in allergen-specific IgE production is commonly reported in most of the CM-OIT protocols described,1924303840 other studies have reported no changes,172025 which according to the authors, might be explained due to the shorter duration of their treatments.
In accordance with previous publications,4142 β-CN-primed PBMCs from CM allergic patients presented a significant Th2-biased phenotype when compared to nonallergic individuals. In fact, enumeration of CN-specific IL-4- and IL-13-secreting T cells has been proposed as a promising tool to improve diagnosis of CMA.43 β-CN (27% of the total milk proteins) was chosen for PBMC stimulation as it represents a serious health risk in patients with CMA, since 75% of sera from patients with IgE-mediated CMA against whole bovine CN have IgE directed against it.44 Furthermore, it is known that PBMCs from clinically reactive IgE-mediated CMA patients proliferate in response to LPS-free αS-, β-, and κ-CN, but not β-Lg.45 Importantly, significant differences in baseline IL-5 and IL-13 levels between CMA and nonallergic children were no longer found once the treatment had finished, demonstrating a transition toward a nonallergic phenotype in the patients able to ingest ≥200 mL of milk without developing symptoms. To the best of our knowledge, there is only 1 other publication dealing with changes in the cytokine response in milk allergic individuals subjected to CM-OIT. Bedoret et al.21 found a shift from IL-4 and IL13 to IFN-production in patients desensitized to milk. However, in our protocol, detectable levels of β-casein-specific IFN- were not found.
In contrast to other OIT protocols toward egg3246 or peanut,47 IL-10 production by β-CN-stimulated PBMCs decreased, suggesting not only Th2- and Treg cell impairment, as IL-10 production is considered one of the main effectors responsible for the suppressive effect of Treg.48 Interestingly, Bedoret et al.21 ruled out a role of allergen-specific FoxP3+ regulatory T cells in oral desensitization to CMA, suggesting that even when high doses of antigen are administered, the mechanism lies in anergy or deletion, rather than suppression, of allergen-specific T cells. However, according to Shreffler et al.,49 allergen-specific and functionally suppressive Treg cells play a role in the resolution of milk allergy and could be important targets for immune monitoring. The authors reported that introduction of milk into the diet causes a decline in the frequency of Treg present in the peripheral blood, in parallel with an increase in the IgG4/IgE ratio and a reduced basophile response, which is attributed to Treg cells being recruited to the gastrointestinal tract by allergen ingestion.49 Similarly, Varsheny et al.50 claimed that decreased Th2-cytokine and increased IgG4/Treg cell productions are the main immunologic changes that accompany the clinical efficacy of peanut OIT, even if they do not detect significant changes in blood IL-10, which raises the hypothesis that blood cytokine levels do not reflect mucosal production of Treg or that mucosal and periphery Treg exert different functions. A further possibility is that induction of Treg is transient. Thus, Jones et al.47 found, in the course of peanut OIT, early generation of Treg and associated increased production of IL-10 by PBMCs eventually decreased after 12 months. In this respect, it should be noted that in our study, a long period of time required for a successful outcome of the treatment (average 18.9 months) might have masked certain immunological events. On the other hand, in accordance with our results, Tiemessen et al.42 reported that CM-specific IL-10 production was significantly higher in T-cell clones derived from children with persistent CMA than from nonallergic children.
The lack of treatment-related changes in the expression of Treg (Foxp3), Th1 (Tbet), or Th2 (GATA3) transcription factors, despite the existence of measurable variations in cytokine production, was already reported by Jones et al.47 and Perezábad et al.32 in their studies with peanut and egg OIT, respectively.
In conclusion, this report presents an efficient and safe milk-OIT protocol characterized by the progressive introduction of milk-containing foods that may substantially improve the patient's quality of life along the treatment course. Successful OIT was accompanied by an immune alteration characterized by a significant increase in antigen-specific IgG4 levels, a significant reduction in antigen-specific IgE concentration, and IL-5, and decreased IL-13 production by β-CN-stimulated PBMCs toward a nonallergic phenotype. More research needs to be done in order to understand the role of IL-10 in CM-OIT.



 XML Download
XML Download