

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Quinolones are the synthetic broad spectrum antimicrobial agents which are frequently used for various gram positive and gram negative bacterial infections.1 The most frequently used quinolones are classified into 4 generations according to their main antibacterial activity and chemical structures. For example, nalidixic acid is in the first generation, ofloxacin (OFX), norfloxacin, and ciprofloxacin (CFX) are in the second generation, levofloxacin (LFX) is in the third generation and gemifloxacin (GFX) and moxifloxacin (MFX) belong to the fourth generation. As a result of their structural diversity, the frequency of adverse reactions with specific agents varies.23
The incidence of adverse events is 2%-10% involving gastrointestinal and central nervous system complaints, as well as hypersensitivity and phototoxicity, and less than 2% of these reactions are immunologic.3 In parallel to the increased quinolone consumption, the frequency of hypersensitivity reactions has significantly increased over the past decade and quinolones represent the most frequent reason for hypersensitivity reactions among non beta-lactam antibiotics.4 Quinolones induce hypersensitivity reactions primarily by immunoglobulin E (IgE) and T cell-mediated mechanisms.567 The most common hypersensitivity reaction types are urticaria and anaphylaxis.5678 Nonimmediate hypersensitivity reactions to quinolones including maculopapular exanthemas, fixed drug eruptions, acute generalized exanthematic pustulosis, Stevens-Johnson syndrome, and toxic epidermal necrolysis are less often seen.7
The diagnosis of hypersensitivity reactions to quinolones poses an important challenge since no standardized and reliable test method has been identified. Although various methods including skin test (ST), detection of drug specific IgE, basophil activation test (BAT), and lymphocyte transformation test (LTT) have been used for diagnostic purposes, contradictory results regarding the sensitivity and reliability of these tests had been reported.7 While some studies reported ST are useful69101112 others revealed that it can give unreliable results.1314151617 Similarly, studies evaluating the value of BAT revealed contradictory results.7 One study, using CD203c as the activation marker, reported positive results in all patients who had experienced anaphylaxis.19 A recent study also found BAT positivity in 69% of severe reactions.13 However, in 2 studies CD63 was negative in patients who had experienced anaphylaxis during drug provocation tests (DPTs).1214 Some authors proposed that LTT could confirm quinolone hypersensitivity and detect some degree of cross-reactivity.2021 However, due to some technical difficulties many laboratories do not obtain sufficient sensitivity with this test and only a few groups routinely use it.20 Because of the lack of reliability of diagnostic STs and in vitro tests, DPT which has the risk of severe reaction seems to be the best method for detecting quinolone hypersensitivity.79
The predictive pattern and the rate of cross reactivity between different quinolones are not well defined. Some previous studies reported a high degree of cross-reactivity between the first and second generation quinolones and the authors suggested avoidance of all quinolones in these patients.162223 However, recent studies evaluating newer quinolones including CFX, LFX, and MFX reported lower cross-reactivity.101224 Furthermore, these studies showed that the pattern of cross-reactivity between different quinolones is complex and cannot be predicted.9
The aim of this study was to detect the importance of in vivo and in vitro diagnostic tests (BAT and LTT) in the diagnosis of hypersensitivity reactions to quinolones, to assess the potential factors influencing the severity of reactions, and to evaluate the cross reactivity between different quinolones including the newest quinolone GFX.
Go to : 
MATERIALS AND METHODS
This cross sectional study was conducted in the adult allergy clinic of Istanbul University, Istanbul Faculty of Medicine between December 2013 and June 2015.
The study group was comprised of 54 patients with a history of 57 hypersensitivity reactions due to quinolones up to 24 hours after drug intake, and 10 healthy controls who were known to tolerate the quinolones. The following categories of patients were excluded from the study: those who had experienced hypersensitivity reactions more than 24 hours after drug ingestion, had a reaction that did not resolve after cessation of the drug, had used additional drugs concomitantly, had experienced severe drug reactions such as vasculitis, Stevens-Johnson syndrome, toxic epidermal necrolysis, and drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome, had comorbid diseases such as uncontrolled asthma, uncontrolled diabetes, uncontrolled hypertension, cardiac diseases, and malignancy as well as those who did not give informed consent.
Drug hypersensitivity reactions (DHRs) were classified as immediate DHRs which occurred within 1 hour after the last drug ingestion and nonimmediate DHRs which occurred 1 hour after the drug ingestion.25 Anaphylaxis was defined according to the presence of 1 of the clinical criteria: 1) Acute onset of an illness (minutes to several hours) with involvement of the skin, mucosal tissue, or both and respiratory compromise or reduced blood pressure or associated symptoms of end-organ dysfunction or both; 2) Two or more of the clinical findings that occur rapidly after exposure to a likely allergen including involvement of the skin-mucosal tissue, respiratory compromise, reduced blood pressure or associated symptoms, and persistent gastrointestinal symptoms; and 3) Reduced blood pressure after exposure to known allergen (for adults systolic blood pressure of less than 90 mmHg or greater than 30% decrease from that person's baseline).26
Allergy workup
Demographic data and clinical features were assessed with a detailed history. All the patients were first undergone skin prick tests (undiluted) with both the culprit and alternative quinolones on the volar side of forearm. Tests were considered as positive if a wheal greater than 3 mm in diameter was present after 20 minutes. If the results were negative, intradermal tests were performed with both the culprit and alternative quinolones in 2 incremental dilutions (1/1,000 and 1/100).27 Intradermal tests were applied and interpreted as previously suggested.672728 For patients who experienced nonimmediate type hypersensitivity reactions, drug patch tests were performed when the delayed reading of intradermal tests was negative. For the patch tests, the commercialized forms of the culprit and alternative drugs were diluted in petrolatum with the drug being 30% of the mixture. The tests were read on the second and forth days after the application.29 Single-blind placebo-controlled drug provocation tests (SBPCDPT) were performed with the culprit and alternative quinolones as suggested (Table 1).730 A DPT was considered positive if any signs or symptoms of a hypersensitivity reaction occurred up to 24 hours after the last dose. Since there is no report regarding skin prick and DPTs with GFX in the literature, test doses were determined according to previously accepted test doses for other quinolones (Table 1). Patients with a history of anaphylaxis and those who did not want the re-exposure were not provoked with the culprit drug.
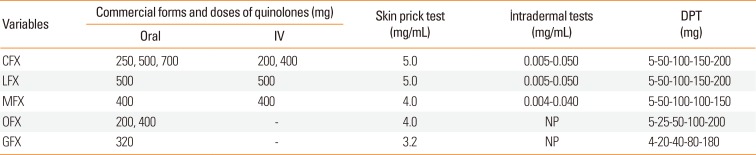
Table 1
Commercial forms and doses of quinolones used in skin prick tests, intradermal tests, and DPTs
![]()
STs were not performed in healthy controls. Results of the STs performed in patients who did not react during DPTs with alternatives were accepted as the controls of the STs. Their results were used to calculate specificity and negative predictive value of the STs as the same method which was used in a similar previous study.18
Atopy, confirmed additional drug allergies, and the serum total IgE (tIgE) levels were evaluated as potential contributing factors in all patients. Atopy was described as a positive skin prick test for at least 1 common inhalant allergen. The serum tIgE was measured using the ImmunoCAP System (Phadia AB, Uppsala, Sweden).
Blood samples for the BAT and LTT were collected from patients with a history of hypersensitivity reactions to quinolones and from nonatopic individuals who were known to tolerate quinolones.
BAT
Flow cytometric analysis of in vitro activated basophils was performed with Flow2Cast technique, which uses CCR3 as the basophil identification marker and CD63 as the marker of basophil activation (Bühlmann Laboratories AG, Schönenbuch, Switzerland). We used 8 test tubes containing 50 µL of whole blood (The blood was collected into K-EDTA venipuncture tubes, up to the dedicated volume). We performed cell stimulation immediately after collection of the blood and we did not store the blood samples. The first sample was mixed with 50 µL of stimulation buffer as a negative control. The next 2 samples were mixed with 50 µL solution of anti-FcεRI (a highly specific monoclonal antibody for the IgE receptor) and 50 µL solution of FMLP (an unspecific cell activator- the chemotactic peptide N-Formyl-Met-Leu), as positive controls. A positive control higher than 10% basophils indicates that the patient is not a nonresponder and excludes CCR3 downregulation. In the remaining 5 test tubes, 50 µL of Quinolones (22.5 µg/mL CFX, 28.4 µg/mL MFX, 182 µg/mL LFX all of which were from Bühlmann Laboratories AG, 100 µg/mL GFX from Abdi Ibrahim, Istanbul, Turkey, and 4 µg/mL OFX from Sanofi Aventis, Istanbul, Turkey) solution was added. Subsequently, 20 µL staining reagent with 2 monoclonal antibodies, anti-CCR3-PE (human chemokine receptor labelled with phycoerythrin) and anti-CD63-FITC (or Gp53, a glycoprotein expressed on activated basophils), were added in each tube. The samples were incubated for 15 minutes at 37℃ in a water bath. A prewarmed lysing solution of 2 mL was added to each tube and incubated for 10 minutes at room temperature. After centrifuging (500×g, 5 minutes) and washing, the cells were suspended in 300 µL wash buffer. Our laboratory limit of basophilic cells analyzed for allergies was set to 500. On our histogram defined by forward scatter and side scatter, several populations of cells are identified: CCR3-positive cells (basophils and eosinophils, the main effector cells in allergic inflammation) and CCR3-negative cells (lymphocytes, monocytes, and granulocytes). Basophils are characterized as being the brightest cells (showing high-density fluorescence with anti-CCR3-PE label) and having low side-scatter. The up-regulation of CD63 marker on the basophils was measured using Cell Quest programme (FACSCalibur Becton Dickinson, San Jose, CA, USA). Results were considered positive when the percentage of CD63 was 5% above the negative control (baseline CD63 expression of each patient).8
LTT
Assesment of quinolone specific CD4+ T cell proliferation
Peripheral blood mononuclear cells (PBMC) were obtained by Ficoll-Hypaque (1.074 g/mL density; Sigma Chemical Co., St. Louis, MO, USA) density gradient centrifugation. Cells were re-suspended in phosphate buffered saline (PBS) and stained with the green fluorescent dye, carboxy-fluorescein-succimidyl-ester (CFSE) (Fluka BioChemika, Buchs, Switzerland) at the final concentration of 5 µM and then incubated for 6 minutes at 4℃. Cells were washed and adjusted to a final concentration of 1×106 cells/mL in a complete RPMI1640 medium (Sigma Chemical Co.). PBMC were seeded in 1,000 µL of complete medium in 48-wells plates with LFX (182 µg/mL) MFX (28.4 µg/mL), CFX (22.5 µg/mL), and OFX (4 µg/mL) for 5 days at 37℃ in a humidified 5% CO2 atmosphere. Phytohemagglutinin (PHA; Gibco, Langley, OK, USA) (10 µg/mL) served as a positive control while wells without stimulation (RPMI1640 only) served as a negative control. Each condition was performed in duplicate. After 5 days of culture, cells were washed in PBS, and labeled with anti-human-CD4-PE monoclonal antibody (BD Bioscience, San Jose, CA, USA). The cells were fixed in paraformaldehyde (2%) for 15 minutes at room stemperature and analyzed on a FACSCalibur instrument using a CELL Quest software (BD Bioscience) flow cytometer. A stimulation index of quinolones-specific CD4+ T cell proliferation greater than 2× proliferation of unstimulated cells was accepted as positive. Data were analyzed using FlowJo (version 8.7.1; TreeStar, San Carlos, CA, USA) (Fig. 1).
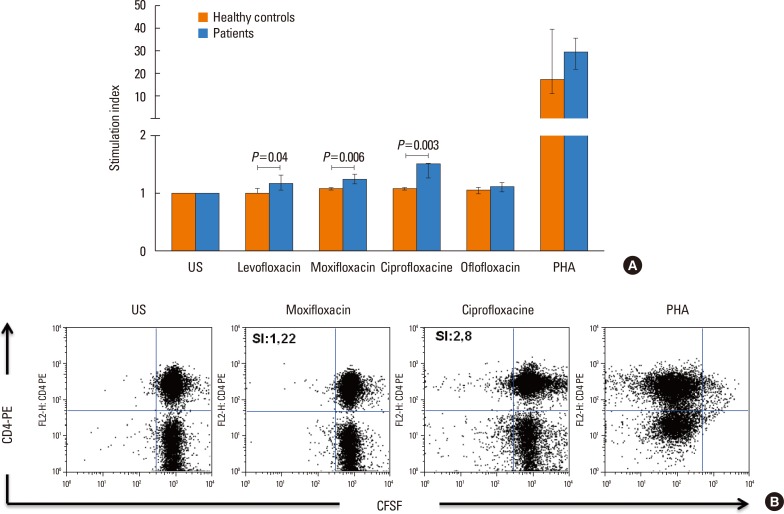 | Fig. 1LTT results of quinolone specific CD4+ T cells. Graphic represents the comparison of the mean stimulation index in healthy controls and the patients. Although SI values of LTT performed with LFX, MFX, and CFX were less than 2, these were significantly higher in patients than in healthy controls (Mann-Whitney U test was used to determine significance between groups. P<0.05 was accepted as statistical significance level) (A). FlowJo program imagesare representative dot plots of patient number 11. The expansion of CD4+ T cells during culture with MFX and CFX was shown and SI values were also indicated (B). LTT, lymphocyte transformation test; SI, International System of Units; LFX, levofloxacin; MFX, moxifloxacin; CFX, ciprofloxacin.
|
This study was approved by the ethical committee of Istanbul University and informed consent was received from all patients and control subjects.
Statistical analysis
Descriptive statistics were used to evaluate the demographic and clinical characteristics. Categorical data were assessed by χ2 tests and quantitative variables without normal distribution were analyzed by the Mann-Whitney test. P values less than 0.05 were considered statistically significant. All data analyses were performed with SPSS version 21.0 (SPSS Inc., Chicago, IL, USA).
Go to :
RESULTS
Patient characteristics
We evaluated 57 patients with a history of hypersensitivity reactions to different quinolones. Three patients experienced hypersensitivity reactions with 2 different quinolones (1 patient with CFX and MFX, 2 patients with CFX and OFX). Three patients (culprit drugs: CFX, OFX, and LFX) discontinued the study due to anxiety caused by positive STs. Overall the study included 54 patients with a history of 57 hypersensitivity reactions. Forty-seven patients (87.0%) were women and the mean age was 42.31±10.39 years. The frequency of atopy was 44.4% and the most common atopic agents were house dust mites and pollen (25.9%). Almost half of the patients (46.3%) had an additional drug allergy. The most common cause of additional drug allergy was beta-lactams (37.1%) and was followed by nonsteroidal anti-inflammatory drugs (NSAIDs) (18.5%). The median interval between the reaction and the evaluation was 9.5 months (Table 2). The frequency of immediate type hypersensitivity reactions was 75.4%. The most common culprit drug was CFX (n=30, 52.6%), the most common reaction type was urticaria (n=15, 26.3%) and the frequency of anaphylaxis was 19.3% (Table 3). The leading causes of anaphylaxis were MFX (45.5%) followed by CFX (27.3%).
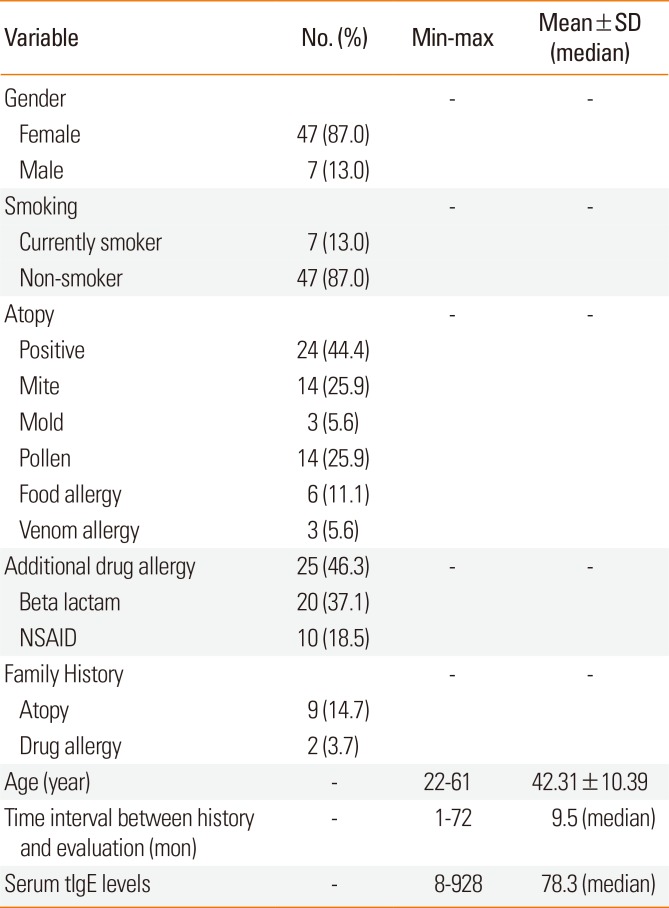
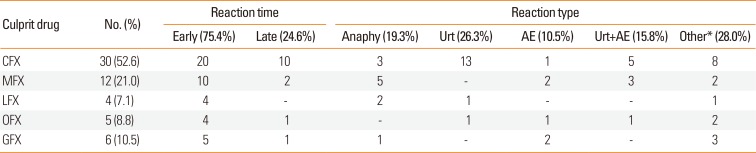
Table 2
Demographic and clinical features of patients
![]()
Table 3
Features of hypersensitivity reactions to quinolones in history
![]()
A total of 270 skin prick and intradermal tests with the culprit and alternative quinolones (57 of them were with the culprit drugs, whereas 213 of them with alternative quinolones) were performed and 7.8% of them were considered positive. Sixty drug patch tests were performed and only one positivity was observed (with MFX). A total of 89 BATs were performed in 18 patients with the culprit and alternative drugs and 50 BATs were performed in 10 control subjects who tolerate quinolones. In 9 patients 14 BATs revealed positive results (16%). A total of 67 LTTs were performed in 21 patients with the culprit and alternative drugs. LTTs were not performed with GFX because the cells died when they were incubated with GFX during the first attempt. Forty LTTs were performed with 10 control subjects who tolerate quinolones. In 4 patients, 4 LTTs all of which were with CFX revealed positive results (5%). However,International System of Units (SI) values were significantly higher in patients with the LFX, MFX, and CFX than in healthy controls (P=0.040; P=0.006; P=0.003, respectively) (Fig. 1). Out of 225 SBPCDPTs, 26.2% (n=59) were positive.
Evaluation of in vivo tests with the culprit drugs
Eleven of 57 STs with the culprit drugs were positive (19.3%) (5 positivity with CFX, 6 with MFX and 1 with LFX, whereas none of them had positive response to GFX and OFX). STs were positive in 10 patients who experienced immediate type reactions whereas late reading of intradermal tests were negative and only one of the patch tests was positive with non-immediate reactions. Two ST positive patients (1 with CFX and the other with MFX) were orally provoked and one of them developed late onset urticaria and the other one developed anaphylaxis. Out of 46 patients whose STs were negative 23 were provoked and 18 patients experienced a reaction (Table 4 and Fig. 2). DPTs were negative in 5 patients (21.7%). Interestingly, all the patients who had a reaction were female and most of these reactions were nonimmediate (Table 4).
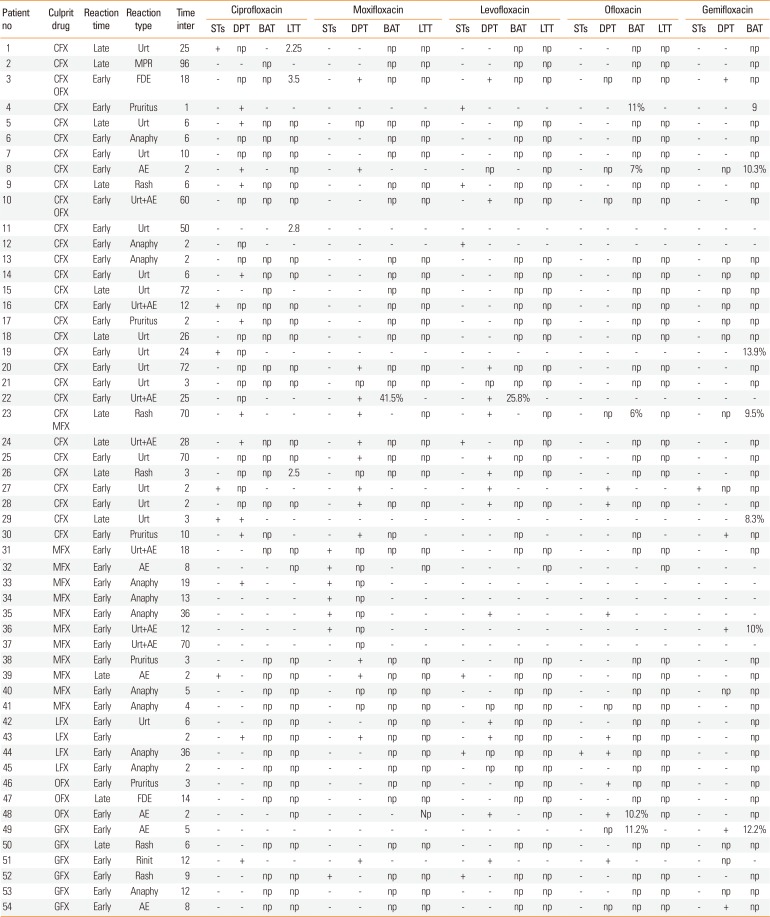
 | Fig. 2Results of the in vivo and in vitro test with the culprit drugs. CFX, ciprofloxacin; MFX, moxifloxacin; LFX, levofloxacin; OFX, ofloxacin; GFX, gemifloxacin; DPT, drug provocation test; BAT, basophil activation test; LTT, lymphocyte transformation test; Ptn, patient; NP, not performed.
|
Table 4
Results of diagnostic tests in the patients with the history of hypersensitivity reactions to quinolones
![]()
Evaluation of in vivo tests with the alternative drugs
In 5 of the 30 CFX-hypersensitive patients STs were found positive with LFX (n=4) and GFX (n=1). DPTs with the same drugs were negative in 4 LFX ST positive patients. However, it was not performed in the GFX ST positive patient. In 9 LFX ST negative, 10 MFX ST negative, 2 OFX ST negative and 2 GFX ST negative patients, DPTs with each drug were positive. In 2 of the 11 MFX-hypersensitive patients, STs were positive with CFX and LFX and both patients did not react in the DPTs. In 1 MFX hypersensitive patient skin test with CFX was positive but she did not want to be provocated. In 4 patients although STs were negative, DPTs were positive with 5 of the alternative drugs. Among LFX-hypersensitive patients, 1 patient had a ST positivity and DPT was positive. In 3 patients STs with CFX, MFX, and OFX were negative but DPTs were positive. In 1 OFX-hypersensitive patient, ST with LFX was negative whereas DPT was positive. In a GFX-hypersensitive patient ST with MFX was positive but DPT was negative. In 3 ST negative patients DPTs were positive.
Comparison of STs and DPTs
According to the results of the 223 tests (both skin and provocation tests performed together), the sensitivity of all STs was 3.6% (confidence interval [CI],0.44-12.31), specificity was 95.2% (CI, 0.90-0.97), the positive predictive value was 20% (CI,2.52-55.61), the negative predictive value was 74.6% (CI,68.25-80.34), false positive results were 8% and false negative results were 25%.
Evaluation of BATs and LTTs with both the culprit and alternative quinolones
Considering the BAT performed patients, the reactions of 7 patients out of 10 with a history of a hypersensitivity reaction to CFX and of all other patients (6 with MFX, 1 with OFX, and 2 with GFX) were immediate. BATs with the culprit drugs were positive in 2 patients (10%) who experienced immediate type reactions (1 with GFX and 1 with OFX). With the alternative drugs BAT positivity was 17% (n=12).
The analysis of the results of the LTTs with the culprit drugs revealed 5% (n=4) positivity. LTTs with the culprit drugs were positive in 2 patients with non-immediate reactions to CFX and in 2 patients with immediate reactions to CFX (Table 4). Interestingly, in 1 patient with a history of early onset urticaria due to CFX which had occurred 50 months prior, DPT and BAT were negative but the LTT was positive (Table 4, 11th patient). The LTTs with alternative quinolones revealed no positive result.
Evaluation of cross-reactivity between different quinolones
The results of SBPCDPTs with alternative quinolones were demonstrated in Fig. 3. As shown in the Fig. 3, MFX hypersensitive patients showed the lowest level of cross-reactivity to other quinolones (equally 8.3%).
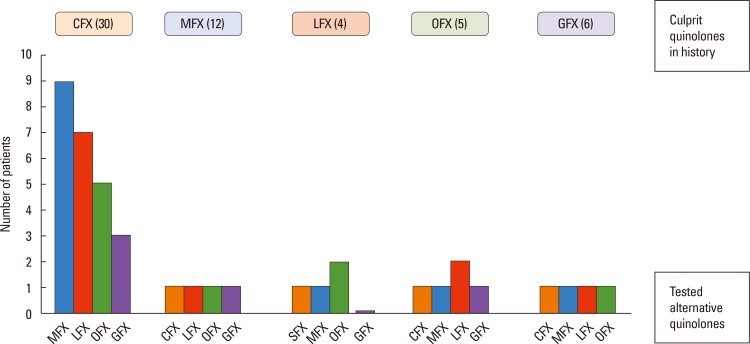 | Fig. 3Evaluation of cross-reactivity between quinolones. Each box represents the quinolone responsible for the reaction in the history and the colorful bars in the graphs stand for positive DPT results with alternative quinolones indicating the cross-reactivity. For example; The orange box at the top of the first column shows the patients with CFX hypersensitivity. The blue bar in this graph shows the number of positive results in DPT performed with MFX. In CFX hypersensitive patients, cross-reactivity with MFX is 30% (9/30). CFX, ciprofloxacin; MFX, moxifloxacin; LFX, levofloxacin; OFX, ofloxacin; GFX, gemifloxacin; DPT, drug provocation test.
|
Evaluation of potential risk factors in severe quinolone hypersensitivity (anaphylaxis)
Factors including age, gender, smoking, atopy, additional drug allergy, comorbid diseases, and serum tIgE levels were assessed in the context of risk factors influencing the severity of hypersensitivity reactions to quinolones. The univariate analyses revealed that being female and having higher serum tIgE levels were associated with anaphylaxis (Table 5).
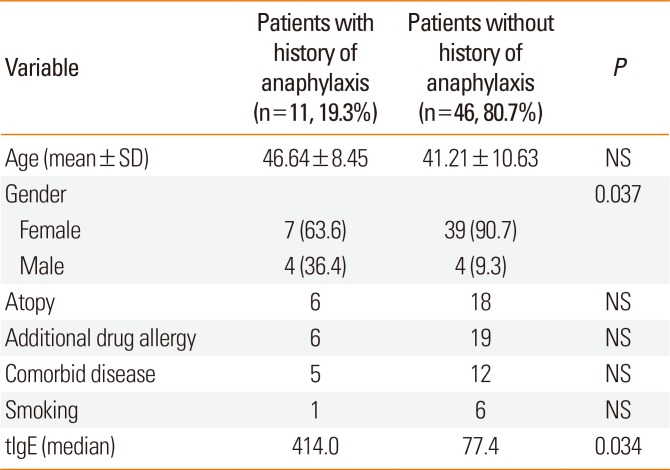
Table 5
Assessment of potential factors associated with development of anaphylaxis
![]()
Healthy controls
Ten healthy controls included in the study. Six of them were female and the mean age was 34.6±4.2 years. The mean SI values of LTT with CFX, LFX, MFX, and OFX were 1.05±0.04, 1.04±0.08, 1.05±0.03, and 1.04±0.40 respectively. The mean percentage of BAT with CFX,LFX, MFX, OFX, and GFX were 2.20±0.64, 1.26±0.77, 1.66±0.95, 2.20±0.60, and 1.58±1.08, respectively.
Go to :
DISCUSSION
To our knowledge, this is the most comprehensive study regarding quinolone allergy and it is the first and sole study which evaluates GFX hypersensitivity and cross-reactivity with other quinolones using in vivo diagnostic tests as well as BAT and LTT.
In the analysis of demographic data, we observed that quinolone hypersensitivity is more common in female and elderly patients as was shown before.63132 Quinolones are preferred especially for infections that do not respond well to beta-lactams, such as prostatitis, acute exacerbations of chronic obstructive lung disease, pneumonia, and gram negative osteomyelitis.33 These types of infections are more commonly seen in elderly patients which may explain the reason for higher frequency of quinolone hypersensitivity in this age group. Some studies reported atopy as a risk factor for beta lactam and NSAID allergy,3435 however there is no data regarding the association between atopy and quinolone hypersensitivity. In the present study, atopy was present in 44.4% of patients and it was not a risk factor for severe reactions. Previously Blanca-López et al.32 reported that quinolone hypersensitivity was significantly higher in beta-lactam hypersensitive patients. Similarly, in our study, the frequency of an additional drug allergy was 46.3% and the most common culprit groups were beta-lactams (37.1%) followed by NSAIDs (18.5%).
In our study, immediate type reactions were more common among quinolone hypersensitive patients (75.4%) and the most frequent reaction types were urticaria (26.4%) and anaphylaxis (19.3%) in accordance with previously reported studies.816 However, some authors found anaphylaxis as the most common hypersensitivity reaction.7932 MFX, which was the most commonly reported drug for anaphylaxis before57932 was similarly found to be the most common causative drug leading to anaphylaxis in our series.
Correctly diagnosing quinolone hypersensitivity is a challenge for allergists. Although some studies reported that skin testing was useful,610111213 controversial results have also been published.91418 Our study revealed that the sensitivity of STs with quinolones was very low as confirmed with SBPCDPTs. BAT was reported as useful in the diagnosis of quinolone hypersensitivity919 whereas some authors demonstrated contradictory results.14 BAT could be a useful option in the conditions that skin testing is not suitable for the drugs or for the hypersensitivity reactions like anaphylaxis.36 In addition, it is known that the usage of BAT is limited to some qualified and specialized centers.37 In this current study, BAT was not found useful as similar with a study published by Seitz et al. and Lobera et al.1214 Different factors including 1) types of reaction, 2) technical issues such as usage of systemic steroids and cyclosporine A, 3) photodegradation effect, 4) culprit drug, 5) time interval between the reaction and BAT, and 6) type of activation markers used can lead to the diversities in the BAT results of the studies.38 In a recent study, the authors reported that depending on the type and severity of the reaction MXF and CFX induced the specific activation markers.38 They found that MFX induced upregulation of CD203c whereas CFX leaded to favourably CD63 activation.38 Moreover, they reported that severity of the reaction affected the BAT result such as in anaphylactic shock CD203c and CD63, and in anaphylactic reactions CD63 seemed to be more accurate.38 Mangodt et al.39 reviewed the literatures to assess the diagnostic utility of BAT in their study and they observed the distinctive results. Because of these various problems BAT does not seem to be a practical and useful diagnostic method in quinolone hypersensitivity and it is needed to be optimized by larger, multicenter studies.
LTT is a promising in vitro test in drug hypersensitivity which has been used for the last 2 decades. In general, stimulation index (SI) greater than 2 is considered as positive in studies evaluating the proliferation capacities of the T cells.20 In our study, only in 4 patients in 4 LTTs SIs were greater than 2. However, we found that SIs were significantly higher in patients with the LFX, MFX, and CFX than in healthy controls (P=0.040; P=0.006; P=0.003, respectively) (Fig. 1). Moreover, we observed that in patients with a confirmed non-immediate hypersensitivity to quinolones, SI could be lower than 2. This occurred in patient number 8 (maculopapular eruption with MFX, SI=1.5) and 29 (late onset urticaria with CFX, intradermal ST lately positive, and SI=1.48). Depending on the SI>2, our study showed that LTT did not seem to be useful in quinolone hypersensitivity. Optimization of the technique of the LTT is necessary as well.
Cross-reactivity is another problem related to quinolone hypersensitivity which has not yet been solved. Can we prescribe a different quinolone to patients who had a history of hypersensitivity reactions to one quinolone? Do we have to forbid the usage of all quinolones in these patients? Some publications, primarily case reports or series including a few different quinolones, indicated a high level of cross-reactivity.16212223 These studies banned all subsequent quinolones. On the other hand, studies involving a larger number of patients and types of quinolones showed lower levels of cross-reactivity101221 indicating that different type or types of quinolone can be used in a patient sensitive to 1 quinolone. In our study, cross reactivity ranged from 0% to 50% (Fig. 3). The highest levels were detected between LFX and OFX (50%) and also between OFX and LFX (33%). Hypersensitivity to OFX in LFX hypersensitive patients who tolerated another quinolone such as CFX or MFX was previously reported.2340 Apart from having a common bicyclic ring structure, LFX is the active L-isomer form of OFX. This structural similarity can lead to a higher level of cross-reactivity. In the context of this result OFX should not be prescribed to LFX hypersensitive patients and vice versa.
GFX, which was approved by the Food and Drug Administration (FDA, United States) in April 2003, is 1 of the newest quinolones. This drug has some advantages, such as enhanced activity against anaerobes and gram-positive organisms and less adverse events than earlier generations.41 Although GFX has an increased risk of skin rash (3%), especially in women younger than 40 who receive >7 days of therapy,42 it has shown to rarely cause more serious immunological phenomena, such as erythema multiforme and Stevens-Johnson syndrome.43 To date, only 1 case of an immediate hypersensitivity reaction, a biphasic anaphylaxis, was reported.44 The present study is the first which assesses GFX in the context of hypersensitivity reactions, in vivo and in vitro diagnostic tests, and cross-reactivity level between other quinolones. Six patients (5 females, 1 male) with a history of hypersensitivity to GFX were evaluated in the study. One of the females (age 23) experienced a rash after the 9th dose, which is similar to the literature.42 The remaining 5 patients had a history of immediate type hypersensitivity reactions including 1 anaphylaxis (male), 2 angioedema, 1 exacerbation of chronic rhinosinusitis, 1 pruritic rash. Because there was no injectable form of the drug, skin prick tests (undiluted) in all patients and patch test in 1 patient were performed and all of them were found negative. LTT could not be performed because this drug led to T cells' death. BAT was performed in 2 patients. In 1 patient with a history of laryngeal angioedema confirmed by SBPCDPT, BAT was found positive (12.2%), while it was negative in the other patient with a history of rhinitis. Cross-reactivity was detected in 2 patients. The patient with a history of nonimmediate type hypersensitivity with GFX experienced pruritus and erythema with MFX. The patient with a history of exacerbation of chronic rhinosinusitis experienced the same reaction after the ingestion of the other 4 quinolones. Moreover, the cross-reactivity level between GFX and the others was evaluated in other patients who had a history of hypersensitivity to quinolones other than GFX. In the present study LFX hypersensitive patients did not react to GFX and in GFX hypersensitive patients the degree of cross-reactivity to other quinolones was 16.7% indicating that it was a safe alternative. In the FDA Advisory Committee Meeting in 2003,45 it was reported that 10% of CFX hypersensitive patients reacted to GFX, which is in accordance with our study.
We analyzed the potential risk factors influencing the occurrence of anaphylaxis with quinolone. Anaphylaxis was significantly more common among female patients and tIgE levels were higher in the patients with the history of anaphylaxis in univariate analyses. To our knowledge, there is no data so far about the risk factors for severe hypersensitivity reactions to quinolones.
The absence of in vitro and in vivo tests together in all patients is a limitation of our study. Since in vivo and in vitro tests were performed in different visits, some patients could not attend to every part of the studydue to special reasons such as living in another city or being afraid of donating blood.
In conclusion, STs, LTT, and BAT are not supportive in the diagnosis of quinolone hypersensitivity and in the prediction of cross reactivity. Therefore DPT is necessary for diagnosis. The frequency of cross-reactivity between all 5 quinolones was approximately 5%. Cross-reactivity depends on the individual quinolone and ranges from 0 to 50%. Although MFX was the most common cause of anaphylaxis, its cross-reactivity level was the lowest with other quinolones. Therefore, in a quinolone hypersensitive patient another quinolone can be prescribed only after cautious interpretation of results. The suggestions as indicated Fig. 4 arisen from our experiences with quinolone hypersensitivity may help for this contradictory matter.
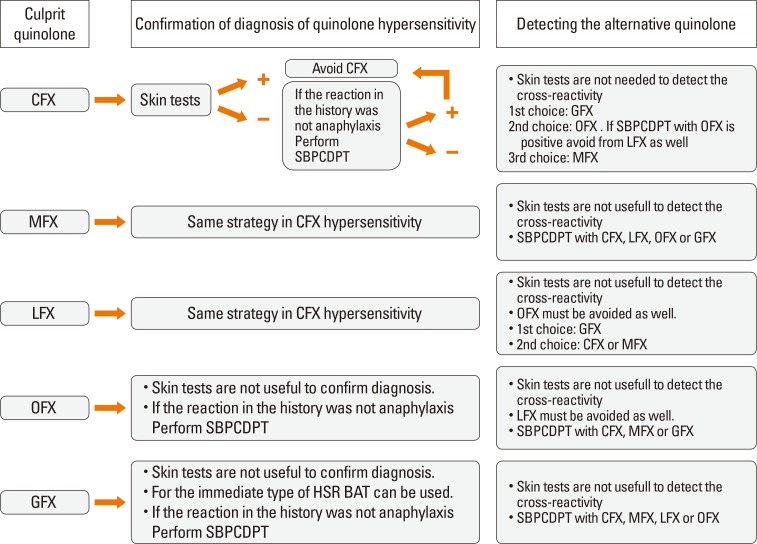 | Fig. 4Suggestions which were extrapolated from the study for choosing alternative quinolone in a quinolone hypersensitive patient. CFX, ciprofloxacin; MFX, moxifloxacin; LFX, levofloxacin; OFX, ofloxacin; GFX, gemifloxacin; BAT, basophil activation test; SBPCDPT, single blind placebo controlled drug provocation test.
|
Go to :
 XML Download
XML Download