

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Antibiotics may be classified as β-lactams (BLs) or non-β-lactams (NBLs). BL antibiotics contain a 4-member β-lactam ring and can be classified into several groups: penicillins, cephalosporins, carbapenems, monobactams, oxacephems, and clavams. NBL antibiotics include macrolides, sulfonamides, quinolones, and aminoglyclosides, which present very different chemical structures and immunogenicity profiles.1
Reaction patterns have been changing in accordance with consumption trends.2 Nowadays, BLs are the most highly consumed antibiotics worldwide, followed by macrolides and quinolones.3 Allergic drug reactions are immunologically mediated and, according to patient reports, allergy to antibiotics appears to be very common, possibly with prevalence as high as 5% to 10%.4 However, many individuals labeled as drug allergic are not truly allergic, and it has been estimated that only 10%-30% of suspected allergic reactions can be confirmed.5 It has been reported that 18% of patients with confirmed reactions to drugs are allergic to BLs, 7% to quinolones, 2% to macrolides, 1.8% to metronidazole, and less than 1% to other antibiotics, such as clindamycin and sulfonamides.5
The diagnostic approach usually includes a detailed clinical history, followed by appropriate in vivo tests (skin and/or drug provocation tests). However, these tests are not always useful due to: 1) potential risks for life threatening and severe reactions, and 2) high rate of false positive skin test results, especially for some NBLs. In vitro tests offer a complementary approach to diagnose allergy to antibiotics. Moreover, in vitro tests are the only alternative method when in vivo tests are not recommended. This review describes current in vitro tests for diagnosing allergy to different antibiotics. The majority of studies have been made for BLs and quinolones, so that they receive the largest amount of attention here.
Classification of allergic reactions to antibiotics
Allergic reactions have been classified by the European Network of Drug Allergy Group into 2 groups based on the time interval between administration and symptom onset: immediate and non-immediate reactions (IR and NIR, respectively). Either can occur following administration of antibiotics. IR usually occur within 1 hour after drug intake6, NIR appear later than 1 hour.7 Allergic reactions to antibiotics can also be classified according to different mechanisms involved, into 4 categories7: 1) Type I, mediated by drug-specific immunoglobulin E (IgE) antibodies, occur less than 1 hour after drug administration. Typical clinical manifestations are urticaria and anaphylaxis, 2) Type II, cytolytic or cytotoxic, mediated by drug-specific immunoglobulin G (IgG) or immunoglobulin M (IgM) antibodies, 3) Type III, mediated by immunecomplex formed by complement-fixing drug-specific IgG or IgM antibodies. Typical symptoms are hemolytic anemia and serum sickness, 4) Type IV or delayed type, mediated by drug-specific T cells. These reactions can be further subclassified into 4 subtypes according to the mechanism involved.8 Onset can occur after 1 hour of drug intake, though reactions usually occur within an interval of 24 to 48 hours. Maculopapular exanthema (MPE) is the most frequent reaction. The most frequent allergic reactions to antibiotics are type I and IV reactions, which correspond to IR and NIR, respectively.
Antibiotics involved in allergic reactions
Betalactams (BLs)
BLs are the most widely used antibiotic family and the compounds most frequently involved in drug allergic reactions5 in all age-groups, with a prevalence rate of 5% to 10%.4 Variations in BL prescription patterns and the introduction of new compounds from this family have modified the allergic determinants that induce the reactions, leading to changes in the patterns of sensitization. Benzylpenicillin (BP) has gradually been replaced by amoxicillin (AX) as the main culprit of allergic reactions.9 Nowadays, allergy to new cephalosporins are also being reported.1011 Reactions to clavulanic acid (CLV) have emerged in the last few years and are progressively increasing,12 though AX is still the most frequent inducer of reactions.210
Quinolones
Both the use and incidence of allergy to quinolones are increasing, being nowadays in Spain the third leading cause of confirmed allergic reactions to drugs, after anti-inflammatory drugs and BL.5 An increase in the incidence of reactions to quinolones has been reported, from 0.53% in 2005 to 5.96% in 2009.5 IR have been reported to all quinolones, with the highest reaction rates for moxifloxacin (63.2%) followed by ciprofloxacin (28.9%) and levofloxacin (7.9%)13; however, ciprofloxacin remains the most frequent quinolone inducing NIR, followed by moxifloxacin and levofloxacin.14 Reactions induced by moxifloxacin are more severe, with 75% of reactions comprising anaphylaxis or anaphylactic shock, vs 54% in those induced by ciprofloxacin.13 It has been described that previous allergy to BL (odd ratio [OR]: 4.571), IR (OR: 17.33) and reactions induced by moxifloxacin (OR: 3.091) were significantly associated with confirmed diagnosis of IR to quinolone.15
Sulfonamides
Allergic reactions to sulfonamide antibiotics in the general population have decreased over time, in line with their reduced consumption. In fact, nowadays the percentage of confirmed reactions to this drug is lower than 1%.5 However, in those patients suffering hematologic malignancies and AIDS, who consume higher rates of this drug, allergic reactions affect as many as 12%-40% and 50%-60%, respectively.1617 Sulfonamide antibiotics rarely cause IR, whereas NIR, such as MPE, fixed drug eruptions (FDE), Stevens Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), and drug rash with eosinophilia and systemic symptoms (DRESS), are more frequently reported.1617
Glycopeptides
Vancomycin is mainly associated with mild reactions including red man syndrome, which is believed to be due to nonspecific mast cell degranulation characterized by flushing, warmth, pruritus, and hypotension. Rarely, IR can be caused by vancomycin.18 NIR, including severe reactions such as SJS, TEN, and DRESS, have been reported.19
Aminoglycosides
Aminoglycoside allergy is relatively uncommon, but important for some risk groups, such as patients with cystic fibrosis. IR and NIR often occur due to contact with neomycin. Other aminoglycosides, such as streptomycin, gentamicin, and tobramycin, have been reported to trigger allergy via topical and/or systemic use and cases of anaphylaxis have been occasionally reported.2021
Macrolides
Allergy to these antibiotics is relatively uncommon (0.4%-3.0% of treatments). IR and NIR have been reported and are generally mild; severe reactions have seldom been reported.22
Diagnostic approach
The diagnosis of antibiotic allergy is complex and usually overestimated.5 This has led to decreased use of broad-spectrum antibiotics resulting in the administration of alternative drugs that may be less appropriate, less effective, or more toxic, potentially leading to a suboptimal or failed therapeutic outcome. Alternative antibiotics may also be more expensive and lead to increased bacterial resistance.26 Therefore, the appropriate diagnosis and management of patients with reported antibiotic allergy is essential in achieving good medical care. The workup of a suspected drug allergy requires the appropriate use of diagnostic tests, if available, including clinical history, physical examination,27 skin tests, and drug provocation testing.28 A detailed history is the most essential step toward an accurate diagnosis of allergic reactions. In addition to the clinical history, a careful physical examination can help better classify possible mechanisms underlying the reaction and guide further investigation.
Skin tests have been used for the diagnosis of both IR and NIR. Although they are considered the most well-validated in vivo method for diagnosing IR to BLs,29 they are not standardized for all antibiotics.110 Many tests for NBLs have low sensitivity and require high concentrations that can result in false-positive reactions due to irritative properties of the drug. Moreover, some NBLs are not available in injectable form, and hence intradermal tests are not possible.1 In the case of quinolones, the value of skin testing is controversial, with most studies showing that fluoroquinolones (FQs) induce false-positive results probably because of their capacity to directly induce histamine release.30 Since clinical history can be unreliable and the sensitivity of skin tests is not optimal, assuming they are even available, the definitive diagnosis of allergy to antibiotics frequently relies upon drug provocation tests.31 The provocation tests are considered the “gold standard” to establish or exclude the diagnosis of allergy to a certain substance.31 However, they are procedures that consume time and resources and not free of risk. They should not be performed in patients at increased risk due to comorbidities like acute infections or underlying diseases, or in patients who have experienced severe lifethreatening reactions, such as SJS, TEN, and DRESS.31 In this sense, in vitro tests are essential to clarify drug allergy status.
In vitro test
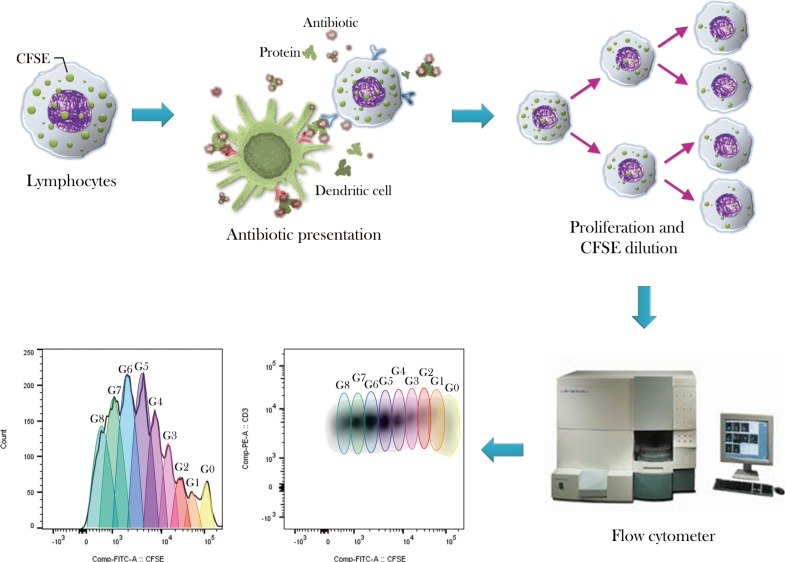
Although less sensitive, in vitro tests yield results that are complementary to in vivo tests. Moreover, in vitro assays are the only alternative to in vivo tests and are recommended to be performed before them in high-risk patients, such as patients with a history of life-threatening reactions.29 In general, in vitro tests are selected depending on the type of reaction or mechanism (IR or NIR) and their sensitivity and specificity values differ in function of the antibiotic tested (Table).
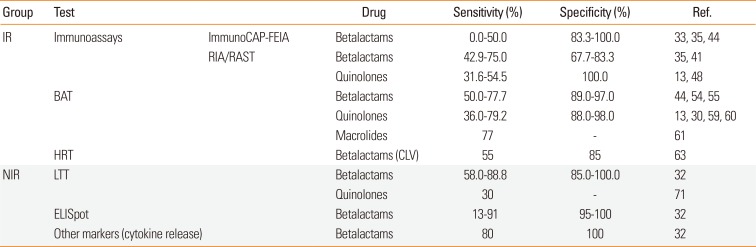
Table 1
Sensitivity and specificity of in vitro tests for specific antibiotic classes
| Group | Test | Drug | Sensitivity (%) | Specificity (%) | Ref. | |
|---|---|---|---|---|---|---|
| IR | Immunoassays | ImmunoCAP-FEIA | Betalactams | 0.0–50.0 | 83.3–100.0 | 33, 35, 44 |
| RIA/RAST | Betalactams | 42.9–75.0 | 67.7–83.3 | 35, 41 | ||
| Quinolones | 31.6–54.5 | 100.0 | 13, 48 | |||
| BAT | Betalactams | 50.0–77.7 | 89.0–97.0 | 44, 54, 55 | ||
| Quinolones | 36.0–79.2 | 88.0–98.0 | 13, 30, 59, 60 | |||
| Macrolides | 77 | - | 61 | |||
| HRT | Betalactams (CLV) | 55 | 85 | 63 | ||
| NIR | LTT | Betalactams | 58.0–88.8 | 85.0–100.0 | 32 | |
| Quinolones | 30 | - | 71 | |||
| ELISpot | Betalactams | 13–91 | 95–100 | 32 | ||
| Other markers (cytokine release) | Betalactams | 80 | 100 | 32 |
![]()
In vitro test for IR
Immunoassay
Quantification of drug specific IgE (sIgE) in serum is based on the detection of a drug (hapten)-carrier-antibody complex. In general, immunoassays use drug (hapten)-carrier conjugates coupled to a solid phase. These solid phases are incubated with patient serum and bound sIgE is detected using anti-IgE antibodies labeled with either a radioisotope (RIA), colorimetric enzyme (enzyme-linked immunosorbent assay [ELISA]), or a fluorescent enzyme (FEIA)32 (Fig. 1). The most readily available commercial method is ImmunoCAP-FEIA, which uses a hydrophilic cellulose polymer configured into a small capsule to which the drug-poly-L-lysine (PLL) conjugates are covalently bound.33 In addition, in-house RIA, especially radioallergosorbent test (RAST), has assessed sIgE antibodies, employing different carriers, solid phases, and activation chemistry. Carrier molecules have included proteins (human serum albumin [HSA]), simpler molecules (amino-aliphatic spacers), polydisperse polymers (PLL) and monodisperse polymers or nanostructures (dendrimers).343536 Although HSA has been used for many years, polymers are preferred nowadays due to their higher capacity for hapten conjugation and sIgE exposition.34 In fact, PLL is the carrier most commonly employed for RIA.35 In recent years, researchers have started to use dendrimers which allow pinpoint control over hapten-carrier conjugate structures, allowing precisely defined chemical conjugates which can be recognized by sIgE.363738 However, comparative studies with PLL are needed to establish whether dendrimers lead to an improvement in sensitivity. The solid phase employed for RAST to BLs is cellulose paper activated with cyanogen bromide, though other activations have been shown to increase hapten fixation.343940 Alternative solid phases used for RIA to BLs and/or quinolones have involved epoxy-activated sepharose beads,1341 as well as zeolites and silica particles.3740 The latter have a high surface area/material weight ratio, allowing efficient functionalization and subsequent sIgE recognition.38 Other innovative research methods to determine sIgE to drugs have been reported. Of note are gold nanodiscs solid phases, functionalized with amoxicilloyl dendrons, that allow nanoplasmonic detection using label-free anti-IgE. Results obtained show a high correlation with ImmunoCAP.42 Besides minimizing patient risk, key advantages of immunoassays are that serum samples can be stored and transported easily and that analysis can be automated. However, they can show low sensitivity due to various factors: 1) drug binding to the solid phase, 2) the carrier forming part of the antigenic determinant, 3) the density of haptens in the conjugate, 4) the metabolites involved in the reaction, 5) time interval (between reaction occurrence and assay), and 6) the lack of positive controls for many drugs.32 Therefore, assays with enhanced sensitivity are still needed to improve in vitro testing. A key consideration is that the solid phase should expose the complete antigenic determinant. This can be difficult to achieve because for most antibiotics the carrier protein moiety involved in the antigenic determinant is unknown. In fact, we only know the antigenic determinant structures for penicillins, but not for quinolones, cephalosporins, CLV, or other BLs. One technical issue that must be taken into account for all in vitro assays is the time interval between reaction occurrence and the performance of the test. Levels of IgE in the sera decrease over time if the patient is not re-exposed to the drug. Therefore, it is recommended that the sample be taken within 2 years following the reaction.43 As described above, many methods have been reported to perform immunoassays for the diagnosis of patients with IR to drugs; however, few approaches have been standardized and evaluated in detail. We will now focus on those methods that have been more comprehensively studied.
 | Fig. 1Schematic representation of the determination of sIgE by immunoassays. During incubation with the patient's serum, antibiotic-PLL conjugate (coupled to a solid phase) is recognized by serum sIgE. The amount of bound sIgE is subsequently quantified using a secondary anti-human IgE antibody labeled with a detectable property, i.e., radioactivity (RAST) or fluorescence (ImmunoCAP). IgE, immunoglobulin E; sIgE, specific IgE; PLL, poly-L-lysine; RAST, radioallergosorbent test.
|
In case of BLs, commercial immunoCAP-FEIA is available for several penicillins (BP, penicillin V, AX, and ampicillin) and for 1 cephalosporin (cefaclor). Its sensitivity depends on the BL involved, but is rather low and variable (0%-50%),333544 although specificity is high (83.3%-100%).35 False allergy diagnoses with ImmunoCAP have been described for cases where the hapten is penicillin V (26%),45 and in patients with high total IgE levels.46 Lowering the threshold from 0.35 to 0.1 kUA/L increases the sensitivity, though it also reduces specificity, particularly for cases with total IgE>200 kU/L.4647 Taking the ratio of sIgE to total IgE into account can increase specificity.47 The limited availability of ImmunoCAP for only a few BLs has led to the use of in-house immunoassays, such as Sepharose-RIA and RAST.32 The latter generally shows higher sensitivity than ImmunoCAP-FEIA, though it is still suboptimal. These methods use isotopic reagents and thus have the additional inconvenience of needing to manipulate radioactive materials. In-house RAST has shown sensitivity ranging from 42.9% to 75.0% and specificity from 67.7% to 83.3% for both penicillins and cephalosporins.35 For these antibiotics, the sensitivity of immunoassays (Immuno-CAP and RAST) generally correlates with the severity of clinical symptoms.3235 The diagnostic value of Sepharose-RIA has been demonstrated in subjects with IR to cephalosporins with good sensitivity (74.3%).41
In case of quinolones, due to the lack of ImmunoCAP availability, in-house assays have become the only alternative immunoassay. In-house Sepharose-RIA has shown low sensitivity for FQs, varying from 31.6% to 54.5%,1348 and high specificity. Differences in sensitivity may be due to the quinolone involved in each study and the severity of the reactions, with better results found in groups where the main FQ involved was ciprofloxacin and the reactions were less severe, such as urticaria. Other factors, such as total IgE levels as well as the time interval between the reaction and the performance of the test, can also influence the results: significantly higher sIgE levels were found in patients evaluated within a few months after the reaction, while patients showing negative results were generally evaluated after a longer time period.48
Basophil activation test (BAT)
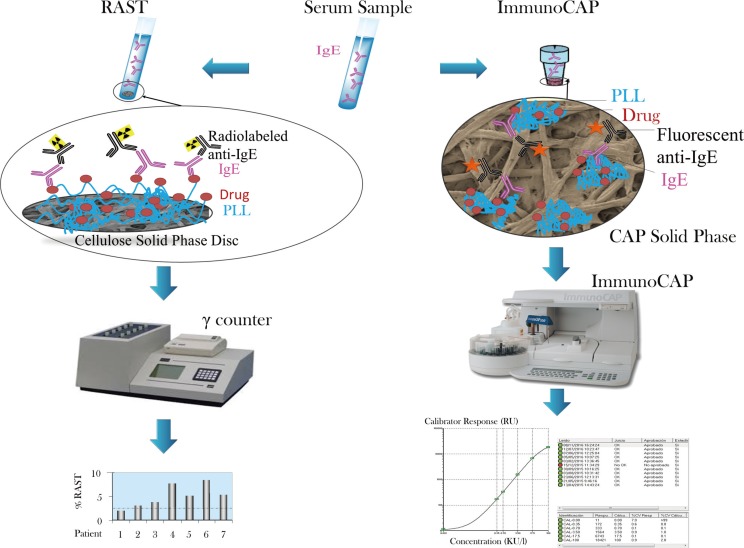
This test is based on the determination of basophil activation using flow cytometry (Fig. 2).49 Commercially available tests exist; however, there is a lack of standardized protocols related to markers, procedures, and drug concentrations,50 leading to the use of in-house protocols in most cases. Basophils can be detected using a single cell marker or a combination (anti-IgE, CCR3, CRTH2, and CD203c). Once basophils have been selected, the most common molecules used to determine basophil activation are CD63 and CD203c. CD63 is highly expressed on the basophil surface after degranulation; however, other cellular types, such as macrophages and platelets, can also express this marker.51 CD203c is constitutively expressed exclusively in basophils and mast cells, and therefore permits a more specific selection of basophils.52 Nevertheless, differences have been found in the up-regulation of both markers depending on the drug tested,53 and it is important to take into account that up to 10% of patients can be ‘nonresponders,’ in which, BAT results cannot be interpreted.50
 | Fig. 2Schematic representation of the basophil activation test. The antibiotic is recognized via IgE on the cellular surface. This process leads to the release of allergy mediators followed by the exposure of activation markers, which can be recognized by fluorochrome-labeled specific antibodies. This activation can be quantified using a flow cytometer. IgE, immunoglobulin E.
|
Regarding BLs, several studies have been carried out to analyze the performance of BAT for BL allergy, with sensitivity ranging from 50% to 77.7% and specificity from 89% to 97%.445455 The differences are due in part to the characteristics of the patients. A sensitivity of 59% was found for patients with positive skin test to at least one BL, 60% for patients with negative skin test and positive in vitro IgE detected by immunoassay, and 77.7% for cephalosporin allergic patients.5455 The results were similar among different studies and in agreement with those obtained by immunoassays (CAP/RAST), showing that the inclusion of BP, AX, and cephalosporin at a minimum of 2 concentrations is very important in obtaining optimal results in BAT to BLs.54555657 BAT has recently been shown to be useful for analyzing CLV reactions, and it has been demonstrated that 30% of reactions in patients taking AX-CLV were CLV selective.12 Given this finding, we recommend the inclusion of CLV for the evaluation of reactions induced by AX-CLV, especially when skin tests with BP and AX are negative.
A decrease in serum IgE can affect the results of both BAT and RAST. Both tests can be affected by time, with BAT in AX allergic patients becoming negative after a shorter period than RAST. Survival analysis showed a loss of positivity of more than 50% in tests performed over 18 months after the reaction.43 Nevertheless, BAT is recommended for diagnosing IR to BLs and can be complementary to in vivo testing and even to other in vitro tests.3249
Regarding quinolones, BAT has been shown to be useful for the in vitro evaluation of quinolone allergy, especially for FQ.13305859 It has been reported to have sensitivity ranging from 36% to 71%, depending on the drug tested,1359 with a higher rate of positive cases for severe reactions (69%).13 Importantly, this technique has shown a good negative predictive value and can therefore help decide whether to perform DPT in suspected FQ-allergic patients.58 The drugs included in the test can affect BAT results, increasing sensitivity in particular cases. For example, the inclusion of moxifloxacin and ciprofloxacin in the evaluation of moxifloxacin-allergic patients increased BAT sensitivity from 41.7% to 79.2% compared with the results obtained using the culprit alone. However, the inclusion of moxifloxacin in the evaluation of ciprofloxacin allergic patients did not improve sensitivity.30 The improvement in BAT sensitivity with the inclusion of ciprofloxacin may be due to several reasons. The most important is photo-degradation of the FQ molecules, since moxifloxacin has a higher rate of photodegradation than ciprofloxacin. Indeed, performing the test in dark compared to light conditions increases sensitivity from 17.9% to 35.7%.60 A recent study has highlighted the importance of the choice of activation marker. It has been observed that ciprofloxacin induces a greater upregulation of CD63, particularly for milder reactions, whereas moxifloxacin preferentially upregulates CD203c in more severe reactions. Thus, the use of both is recommended in FQ evaluation when possible.30 Finally, as with BLs and other drugs, it is important to take into account the time interval between reaction occurrence and BAT performance. It is very critical to perform the test as soon as possible after the reaction, due to a negative correlation between the time interval and the up-regulation of the activation marker.30 Due to the scarce availability of alternative diagnostic tests and the proven diagnostic value of BAT, this test has been recommended for diagnosing IgE-mediated allergy to FQs by the European Network for Drug Allergy.32
Regarding other antibiotics, although all antibiotics that induce IR can be potentially evaluated by BAT, few reports have been found for drugs other than BLs and FQ. One study described the performance of BAT in 18 patients with IR to macrolides, of whom 14 showed positive results.61 Moreover, a case report of a patient with anaphylaxis after topical administration of rifamycin SV showed positive BAT results in the patient and negative results in 2 controls.62
Histamine release test (HRT)
The HRT is based on the detection of histamine release by human basophils after incubation of blood with the antibiotic. The optimized procedure consists of the incubation of heparinized blood on glassmicrofibre plates and stimulation with the antibiotic of interest, followed by the detection of basophil histamine release using fluorometric techniques. This method is suitable as a routine diagnostic test because stimulation of the blood cells can be performed in any laboratory; the plates can then be sent to a reference laboratory for histamine detection and data analysis. HRT has been used for the diagnosis of allergic reactions to several allergens, but rarely to drugs. Recently, the HRT has been used for the evaluation of IR to CLV in a group of patients with positive skin tests,63 showing a sensitivity of 55% and a specificity of 85%. The same study also describes a passive HRT, with similar sensitivity and specificity values to the direct method. Passive HRT is based on the use of “IgE stripped” donor blood sensitized with patient serum followed by incubation with the antibiotic. This is an indirect way to confirm that an IR is mediated by IgE antibodies, which is useful in the absence of methods for the detection of sIgE as in the case for CLV. Furthermore, the passive method presents the advantage that only the patient's sera and not cells are required, eliminating the need to perform the test 24-48 hours after blood extraction.64 Despite the promising results of this study, further research is needed to standardize the use of HRT as a diagnostic test for allergic reactions to CLV and other BLs.
In vitro test for NIR
Lymphocyte transformation test (LTT)
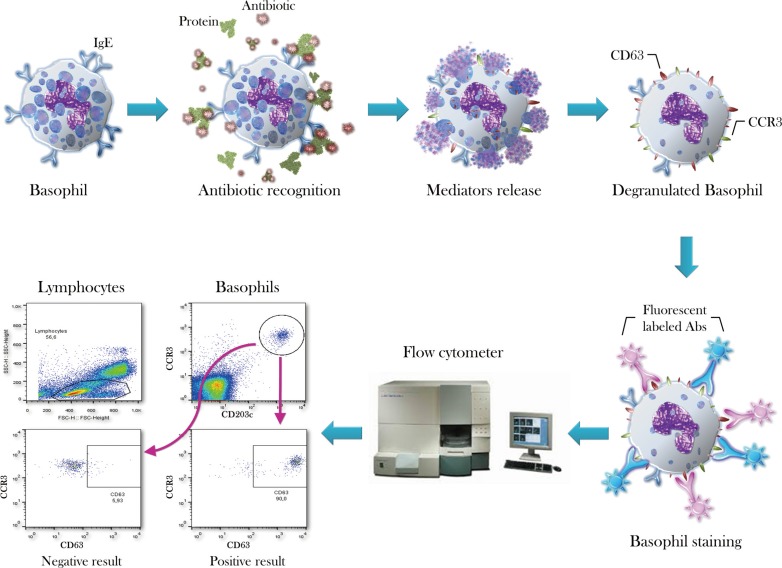
This test is based on the proliferation of drug-specific T cells from patients with NIR upon stimulation with the suspected and/or other related drugs.49 This proliferation can be measured via the incorporation of tritiated thymidine (3H) into the genome of proliferating cells or by the serial dilution of a fluorescent molecule (carboxyfluorescein diacetate succinimidyl ester [CFSE]) into the cells using flow cytometry (Fig. 3).32 The advantage of CFSE is the possible identification of the effector cells involved; however, there is a lack of studies comparing the 2 methods in terms of sensitivity and specificity. Nevertheless, LTT in general has been shown to be more sensitive than skin testing for NIR diagnosis.32 Both sensitivity and specificity depend on the clinical manifestations of the reaction, being higher for MPE, FDE, acute generalised exanthematous pustulosis (AGEP), and DRESS3265 than for SJS/TEN, for which LTT seems to be of little value.65 For DRESS and SJS/TEN, controversy exists regarding when to perform the test. Some studies have found higher sensitivity for DRESS in the resolution phase, while for SJS/TEN the acute phase appears to be more appropriate.32 However, other studies found no differences related to LTT performance timing.6667 Several modifications have been carried out to the original LTT protocol to improve its sensitivity, such as the use of professional antigen-presenting cells, the inclusion of drug metabolites that could be the recognized determinant, the depletion of FoxP3+ regulatory T cells that can suppress activation, and the evaluation of isolated effector cells.32
 | Fig. 3Schematic representation of the flow cytometric lymphocyte transformation test. Lymphocytes are labeled with a fluorescent dye which accumulates in their cytoplasm. After antibiotic presentation, lymphocytes are activated and start to proliferate. This proliferation process leads to the sequential dilution of the dye which can be measured, so that quantified and successive cell generations can be visualized by flow cytometry.
|
Regarding BLs, most studies using LTT have focused on BLs. Its sensitivity and specificity have been revised several times, ranging from 58% to 88.8% and 85% to 100%, respectively.32 The test shows higher sensitivity than skin testing for diagnosing NIR to these drugs.68 Improved sensitivity has been obtained using some of the modifications mentioned above. In the evaluation of NIR induced by AX, the use of professional antigen-presenting cells, such as monocyte-derived dendritic cells, in the cell cultures led to sensitivity increase from 22% to 88%.69 Moreover, the involvement of co-factors, (i.e., from infectious diseases) which were present during the in vivo allergic reaction, has also been investigated as a possible cause of the low sensitivity observed in some studies. For this reason, TLR agonists have been included in the test for the evaluation of AX-induced NIR, increasing sensitivity from 40.5% to 80.7%, with small changes in specificity (from 72.7% to 78.6%).70
Regarding quinolones, most studies have used the LTT to demonstrate the involvement of T cells in the pathogenesis of clinical entities, such as MPE and AGEP induced by FQ.147172 However, there is a lack of studies regarding the sensitivity and specificity of this test in FQ allergy. Although low sensitivity (30%) was found in one study with 10 patients,71 LTT has shown higher sensitivity than skin tests, making it a promising in vitro diagnostic tool for these antibiotics. This may be due to a low capacity of FQ to penetrate the skin or the use of suboptimal FQ concentrations in skin testing.14 LTT has also been used to study FQ-induced photo-allergy, and it has been demonstrated that peripheral blood mononuclear cells photo-modified with quinolones using ultraviolet A light are able to stimulate homologous cell proliferation.72
Regarding other antibiotics, to our knowledge, there are few studies that analyze the LTT in other types of antibiotics. One study used the LTT to analyze sulfonamide-reactive lymphocyte frequency in the peripheral blood of patients with drug-induced eruptions; however, the results were disappointing, with a high rate of false-negative and false-positive results.73
Enzymelinked immunosorbent spot (ELISpot)
ELISpot allows the visualization of the secretory products of individual activated or responding cells, such as relevant cytokines and cytotoxic markers, after cell activation by the culprit drug or their metabolites. Each spot that develops in the assay represents a single reactive cell. Thus, the ELISpot assay provides both qualitative (regarding the specific cytokine or other secreted immune molecule) and quantitative (the frequency of responding cells within the test population) information. One of the advantages of this test is its capacity to detect low-frequency cells in the peripheral blood of the patient; it is able to detect <25 secreting cells per million peripheral blood mononuclear cells.32 Another advantage is that this test can detect drug-reactive T cells even several years after the reaction occurred.74 This technique represents a good alternative for LTT in severe cutaneous reactions, as has been shown for granzyme B and granulysin ELISpot assays.65 Moreover, more than one cytokine can be determined in the same assay, improving the accuracy of the test and reducing the number of cells that must be used.6567 ELISpot for Interferon gamma (IFNγ) has been used in the evaluation of BL-induced NIRs, mainly for AX, with sensitivity ranging from 13% to 91%. Other antibiotics, such as vancomycin, have also been evaluated with this technique, though data on sensitivity and specificity was not provided.32
Other cell markers
Other markers that can be measured by flow cytometry (CD69) or by ELISA (several cytokines and cytotoxic mediators) have been used in the diagnosis of NIR to antibiotics. It has been shown that CD69 is up-regulated in patients allergic to BL and sulphamethoxazole, and flow cytometry determination correlates with LTT results. Moreover, the assessment of different cytokines, such as IFNγ, IL-10, and IL-5, by flow cytometry in NIR showed a sensitivity of 75%. These cytokines can also be measured using ELISA with the LTT supernatant and may be useful for diagnosis.32
Go to : 
CONCLUSIONS
Allergy to antibiotics is an important worldwide problem, with an estimated prevalence of up to 10%. However, most patients with suspected drug allergy cannot be confirmed as such using a proper diagnostic workup. Many patients are diagnosed based on clinical history, which is not always reliable, followed by the performance of in vivo tests that are not always recommended or useful. Therefore, in vitro tests can help guide clinicians to an accurate diagnosis. Immunoassays and BAT are the most highly employed techniques for diagnosing IR to BLs and quinolones; however, their sensitivity is lower than that of in vivo tests. LTT has been the preferred test for diagnosing NIR, though more recently cytokine determination has emerged as a valuable tool. Intensive research will be needed in this area in coming years in order to produce a suitably accurate and accessible in vitro diagnostic test.
Go to :
 XML Download
XML Download