

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic rhinitis (AR) is one of the most common chronic allergic respiratory diseases worldwide. Although AR is not a life-threatening disease, it causes a significant healthcare problem through the chronic, and relapsing characteristics, inducing poor quality of life and work/school loss.12 The impact of AR on the social, professional, and educational performance has been recognized; furthermore, AR in childhood leads to socioeconomic inequalities.3 Therefore, early diagnosis and adequate management of AR have been highlighted to achieve healthy aging.
The prevalence of AR has progressively increased over the last 3 decades in developed countries including Korea, and has been estimated approximately 40% in the world population. The nation-wide prevalence of AR in Korea has varied with 28% in 2008 based on the questionnaire alone, and 16.2% in 2010 based on the questionnaire, examination, and test for atopic sensitization.45 The Korean National Health Insurance Corporation reported an increased trend of medical care-use associated with AR, approximately 4.28 million cases in 2007 (10th ranked prevalent chronic disease) to 6.35 million cases in 2014 (fifth ranked prevalent chronic disease).6 The direct and indirect costs related with AR have been estimated at $223.68 million and $49.25 million, respectively, in 2007.7
Practical guidelines, proposed by Allergic Rhinitis and its Impact on Asthma (AIRA),8 and Academy of Otolaryngology-Head and Neck Surgery,9 recommended evidence-based management. However, up to 40% of patients with AR remain symptomatic.10 Although international practical guidelines are well established, unmet needs for AR care still exist in real-world practice. The existing guidelines were developed on the basis of evidence from randomized controlled trials (RCTs). RCTs would be the best way to assess the effect size under the high-quality design. However, they cannot answer every clinical question in the real-practice.3 Furthermore, existing guidelines do not reflect the characteristics of Korean patients because these guidelines are based on Western populations. Therefore, unmet needs in the clinical practice of AR should be evaluated.
The purpose of the study was to identify the needs for AR care of primary physicians to manage AR patients in Korea and to evaluate needs on the development of new guidelines reflecting
the clinical features of Korean patients.
MATERIALS AND METHODS
A questionnaire-based survey was conducted through e-mail, among a total of 99 clinic based primary physicians consisting of internal medicine (IM), otorhinolaryngology (ORL), and pediatrics (PD) groups (each 33) between June 2 and June 16 of 2014.
Questionnaire development
The questionnaire was developed by the collaborative working group comprising allergists in the departments of IM, ORL, and PD; and the Allergic Rhinitis Work Group (ARWG) in the Korean Academy of Asthma, Allergy and Clinical Immunology (KAAACI). It was based on the free-text questions arising from primary physicians in the clinic-based, real practice. A total of 117 free-text questions were collected and reviewed by the expert panel of ARWG, and consequently developed as 39 questions relating to the respondents' agreement or disagreement with the existing practical guidelines for the diagnosis, treatment, and prevention of AR. The questionnaire-items were uncategorized and shuffled to minimize the proximity effects. The questionnaire asked “Do you agree that the existing guidelines unclearly answer the following question, and do you need development of a new practical-guideline reflecting real practice?” Each questionnaire item was rated on a 5-point Likert scale from 1 to 5 where 1=strongly disagree, 2=disagree, 3=unsure, 4=agree, and 5=strongly agree.
Statistical analysis
To select items that showed overall high agreement, the responses were presented as mean and standard deviation (SD) and assessed by the average deviation index ADmed. The ADmed index proposed by Burke and Dunlap11 provided a clear rationale for defining acceptable levels of interrater agreement on a 5-point Likert scale for values of ≤0.833. We separated the responses into agreement, no opinion, and disagreement. Agreement was the responders choosing 4 (agree) or 5 (strongly agree), and disagreement was considered present if the responders choosing 2 (disagree) or 1 (strongly disagree) for each statement. Thereafter, the items were divided into 3 subgroups, including consensus items, polarized items, and neither consensus nor controversy. The criteria of categorized items were follows: (1) consensus items were defined as <25% of responders indicating neutral opinion and the percentage of agreement was at least 4 times as large as that of disagreement; (2) polarized items were defined as >30% of responders indicating agreement and also disagreement; and (3) neither consensus nor controversy was defined as not included in the consensus or the polarized items. All statistical analyses were performed using R 3.1.3 version (R Foundation for Statistical Computing, Vienna, Austria) and SPSS 14.0 version (SPSS Inc., Chicago, IL, USA).
RESULTS
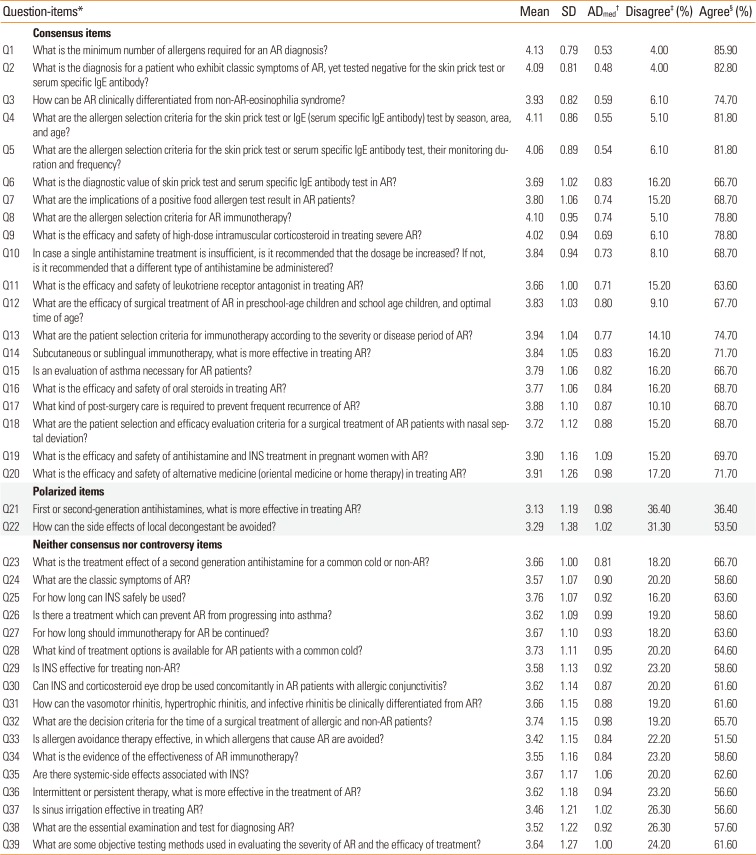
Of the 39 items, there were 20 “consensus items” (51.3%), 17 “neither consensus nor controversy items” (43.6%), and 2 polarized items (5.1%). Fifteen of the 20 consensus items with ADmed of ≤0.833, showed strong interrater agreement, and the remaining 5 items showed poor agreement (ADmed >0.833). However, all the proportion of agreement for these items was approximately 70% (Table 1). Table 2 summarizes the proportion of agreement and the value of ADmed in each specialty-group, respectively, and the specialty-agreement gap.
Among 20 consensus items, 15 (Q1-15) showed the overall agreement. However, only 5 items (Q1-5) showed no specialty-specific agreement gaps (each ADmed ≤ 0.833), the others did not. The Q1-5 consensus items for AR diagnosis that included the minimum test battery of allergens for AR diagnosis, differential diagnosis with non-AR with eosinophilia syndrome or non-AR, and allergen differences by age, season, and area, showed strong agreement on the lack of guidance in the existing guidelines (ADmed; Q1, 0.53; Q2, 0.48; Q3, 0.59; Q4, 0.55; Q5, 0.54) without specialty-specific agreement gaps. However, Q6-7 for the diagnostic value of allergy test and implications of food sensitization showed weak agreement (ADmed: Q6, 0.83; Q7, 0.74) with a specialty-specific agreement gap. The gap was more prominent in PD group than in the IM and OR (Q6-7 ADmed: PD group, 0.60, 0.55; ORL group, 0.83, 0.97; IM group, 0.95, 0.74).
Only 3 items for the second-generation antihistamines, effectiveness of immunotherapy, and effectiveness of sinus irrigation showed overall poor agreement without specialty-specific agreement gaps (ADmed: Q21, 0.98; Q34, 0.84, Q37, 1.02). Twenty-nine other items showed significant specific-specialty agreement gaps, suggesting respondents' needs for specialty dependence. The specific-specialty agreement gaps were mainly observed in the PD group. Neither the IM nor the ORL group showed agreement gaps in 20 of 29 items with specific-specialty agreement gaps, while the PD group showed significant opposing responses, resulting in poor agreement on each question. Q16 for the efficacy and safety of oral steroids and Q20 for alternative medicine, showed disagreement (ADmed: 0.84, 0.98) caused by specialty-gaps (PD, ORL, IM groups: Q16, 0.56, 1.09, 0.84; Q20, 0.73, 0.98, 1.26). Q17-19 also showed disagreement and specialty-gap in the PD group.
In PD group, 35 of 39 items showed acceptable interrater agreement and higher proportion of agreement (90.0%) than the other groups. On the contrary, the ORL and IM groups showed less acceptable interrater agreement (28.2% and 30.8%), respectively. Particularly, 4 items showed interrater agreement for the ORL group, but not IM, group 5 items showed agreement to the contrary.
DISCUSSION
This is the first study to identify the needs for AR care in Korea, to evaluate the gap between real-life practice and existing guidelines, and primary physicians' needs for the development of new guidelines reflecting Korean particularity.
Our results demonstrated various consensus needs for clinical questions, particularly in diagnosis and treatment. There is consensus agreement that existing guidelines are insufficient for AR diagnosis indicating that certain guidance on the minimal selection of allergen tests is needed and should also reflect Korean particularity according to age, area, and season.
However, there are no Korean guides of “How many allergen, and what kind of allergens should be tested to diagnose and exclude AR in Korea?” and “How frequently allergic sensitization should be tested?” An investigation of offending allergens is essential for the diagnosis and treatment of AR. The offending allergens may vary with age, region, and season. Existing guidelines are based on patients outside of Korea; therefore, the minimum test battery of 18 inhalant allergens (Dermatophagoides pteronyssinus and Dermatophagoides farinae, Cat and Dog dander, Artemisia, Blatella, Alternaria, Parietaria, Ambroisia, Aspergillus, Cladosporium, Grass, Cypress-, Olive-, Birch-, Alder-, Plane-pollen, and Hazel) advocated by the Global Allergy and Asthma European Network would not be relevant in Korean patients.12 In Korea, particular pollens, including Japanese hop (Humulus japonicas) or Japanese Cedar (Cryptomeria japonica) have been reported as the major pollens of AR in south provinces.1314 Furthermore, offending allergens are significantly different according to age, variability of offending allergens from indoor allergens in early childhood to outdoor allergens in late childhood.14 Indeed, the National Guideline for the Diagnosis and Management of Allergic disease, published by the KAAACI in 1999, recommended 17 allergens in skin prick test.15 Nevertheless, consensus agreement indicates that respondents still have difficulty in diagnosing AR in the real practice.
Despite existing guidelines, AR primary care seems to be independent of guideline recommendations.16 Furthermore, specialty-specific knowledge and agreement gaps among allergists, otolaryngologists, and pediatricians are known to exist.17 Our findings also demonstrated specialty-specific need gaps that may be caused by specialty-knowledge or -interest gaps. We found the specialty-agreement gap even in the consensus items. The gap was prominent in the safety and effectiveness of treatment. Most guidelines recommend intranasal corticosteroid (INS) as the best monotherapy, while our results showed that 63.6% of respondents still have questioned “How long can INS be safely used?” (Q25). Concerns of INS-safety was stronger in the PD group (69.7% of agreement, ADmed 0.70) than in the ORL group (57.58% of agreement, ADmed 1.03) and IM (63.64% of agreement, ADmed 0.92) groups. The item for the efficacy and safety of oral steroid (Q16) showed specialty-specific agreement gaps between the PD and ORL/IM groups, suggestive of relatively higher concerns of oral steroid use in children than in adults. Therefore, guidance of oral steroid use needs consideration of age specificity. The question on the efficacy and safety of alternative medicine (Q20) also showed conflicting response between the PD and ORL/IM groups. This gap may arise from conflict between guidelines. The ARIA guideline 2010 did not recommend any of acupuncture or herbal medicine in the treatment of AR8; however, the American Academy of Otolaryngology-Head and Neck Surgery stated that clinicians may offer acupuncture for patients who are interested in nonpharmacologic therapy.9 The efficacy and safety of acupuncture or herbal medicine remain controversial. Our results showed high agreement in the PD group, but disagreement in ORL and IM groups. Patients attempt to use alternative or complementary medicine because of several reasons, such as concern of life-long medicine, steroid phobia, and dissatisfaction with the conventional treatments, particularly in children.18 For this reason, the need for unified guidance is growing.
Most guidelines draw their recommendation not from real-world practice, but from the world of RCTs. Although RCTs are considered the gold standard of treatment intervention efficacy, it occasionally fails to be replicated in the real-life setting because it reflects only 10% of the general population.19 In real-life practice, patients do not desire life-long use of steroid, have many co-morbidities, tend to suffer from the mixed type of AR and non-AR rather than AR alone.20 Thus, although RCTs provide highest evidence, guidelines need careful consideration for the acceptance of RCT-driven evidence. Practical guidelines and most of the studies have focused on the management of moderate to severe AR; however, mild intermittent AR is the most prevalent type, comprising approximately >50% of AR at the population level.421 The grading of recommendation, assessment, development, and evaluation system is accepted as the best tool for grading evidence for developing guidelines. It guarantees the highest evidence from the high-graded study; however, numerous questions derived from real practice cannot be answered. Evidence-based guidelines would be insufficient to answer the real world questions. To resolve these gaps, comparative-effectiveness derived from pragmatic trials or real world observation should be considered. Although there has been no pragmatic AR-guideline up to now, The Global Initiative for Asthma Guideline 2016 began to reflect the evidence from real-world effectiveness studies as well as from efficacy studies in the choice of the preferred asthma-controller.22
Taken together, the present survey highlights that existing international guidelines are insufficient for application to real-world practice, and needs of primary physicians for AR care remain unmet; consequently, development of a Korean practical guideline reflecting regional particularity is needed. Furthermore, guideline developers should reflect efficacy from RCTs and effectiveness from the real-world practice, as well the development of regional guidelines.

 XML Download
XML Download