

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic rhinitis (AR) has become a global health problem that affects a large part of the general population.1 According to previous reports, the house dust mite (HDM) is regarded as the most probable inhalant allergen.2 HDM-induced AR is also related to an increased risk of asthma.3 Additionally, compared with other kinds of aeroallergens, if people are exposed to HDM allergens for a long time, the symptoms seem to be more chronic and severe.4 In fact, the prototypic perennial allergen (i.e., HDMs) have not been confirmed, although more and less mite allergens can be found in the early autumn and winter, respectively.5 Symptomatic treatment remains the first treatment choice for patients with AR. However, these methods are costly and impose significant economic burdens on individuals and nations.67 Allergen immunotherapy is the guideline-recommended treatment for AR.8910 Unlike symptomatic drugs, specific immunotherapy provides unique and appropriate management that transforms the process of AR. Remarkably, early treatment of AR with specific immunotherapy may even prevent it from evolving into asthma.1112
Sublingual immunotherapy (SLIT) is regarded as an effective therapy, and is recommended by the World Allergy Organization (WAO) on the basis of relevant research.13 However, a later study on AR using extracts of HDMs demonstrated that there was no consensus on fundamental therapy parameters.14
In evidence-based medicine (EBM), data obtained from meta-analyses and randomized controlled trials (RCTs) are the most convincing regarding the efficacy of an intervention.1516 Both Cochrane's studies and reported meta-analyses171819 confirmed the effectiveness of AR-related immunotherapy. In 2009, to our knowledge, the first meta-analysis of RCTs examining SLIT for HDM-induced AR and allergic asthma20 showed that there was no apparent difference in the sub-analyses on children and adults, indicating that more persuasive data are required. The needed data may now be available because of the large number of reported trials since then. In this study, we investigated the efficacy of SLIT with HDM extracts for AR to resolve the controversy related to the efficacy of desensitisation to this kind of allergen.
MATERIALS AND METHODS
We searched for well-powered RCTs within the last 26 years (1990-2016) on the treatment of PAR. RCTs assessing outcomes of AR-related symptom and/or medication scores were enrolled. The Cochrane Library, Medline, and Embase were searched using Boolean combinations of the following: (“sublingual” or “swallow”) and (“immunotherapy” or “desensitization” or “immunologic”) and (“allergic” or “hay fever” or “rhinitis” or “rhinoconjunctivitis”). When reports pertained to the same patients at different follow-up periods, the one with the longest follow-up was enrolled to avoid duplication. Alternatively, we included all pertinent studies as long as there was no overlap in the information provided whenever multiple reports related to the same trial with different outcomes. Finally, whenever RCTs with multiple intervention and control arms were assessed, for the analysis we retained the placebo arm as the control group and the SLIT arm closest to the US Food and Drug Administration-ratified dosage scheme as the active comparator. Data were requested from authors and study sponsors in cases where data were not reported in published articles or were unsuitable for inclusion in the meta-analysis. Multiple available scores related to rhinitis symptoms were included (i.e., rhinitis symptoms only, rhinoconjunctivitis symptoms, or rhinoconjunctivitis and asthma symptoms) between rhinitis-only scores, which were preferred, followed by rhinoconjunctivitis symptom scores. Regardless of the type and number of outcomes, studies assessing SLIT were enrolled to estimate efficacy in the meta-analysis.
Data extraction
We extracted information on study characteristics and demographics, including investigators, publication year, and journal title, total and per-arm sample sizes, population characteristics, treatment indications, dose and modalities, study duration, rhinitis-related outcomes, and definitions thereof. Continuous outcomes were assessed by the mean difference and standard deviation, which included nasal symptom score and medication score. Data extraction was conducted by 2 investigators (B.F., H.X.) independently with differences resolved by consensus.
Quality assessment
It is essential to evaluate potential biases in the studies selected for a systematic literature review or meta-analysis. Risk of bias in the selected RCTs was assessed according to the Cochrane Collaboration's Risk of Bias tool in Review Manager (RevMan) 5.3 (The Nordic Cochrane Center, The Cochrane Collaboration, Copenhagen, Denmark).
Statistical analysis
The meta-analyses included outcomes of symptom scores and medication scores. The degree of heterogeneity in the estimates was measured, and sources of heterogeneity were explored by removing possible study outliers, and conducting subgroup and sensitivity analyses. Both random effects and fixed effects models were used. Direct pair-wise comparisons of each modality compared with a placebo were undertaken in RevMan 5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration). Two main clinical outcomes for improvement in AR are decreases in symptoms and medication use, as reflected in composite summary scores. We quantified the extent of heterogeneity with the I2 metric (range, 0%-100%), with values of >75% indicating considerable heterogeneity. The observed between-study heterogeneity was explained by performing analyses in prior defined subgroups of trials, and subgroup-specific differences in the effect of the intervention were also defined. Publication bias was examined by funnel plots per assessed outcome and we further assessed asymmetry using Egger regression, which assesses whether there is a significant relationship between the effect sizes and their precision as well as through funnel plots.
RESULTS
Study selection
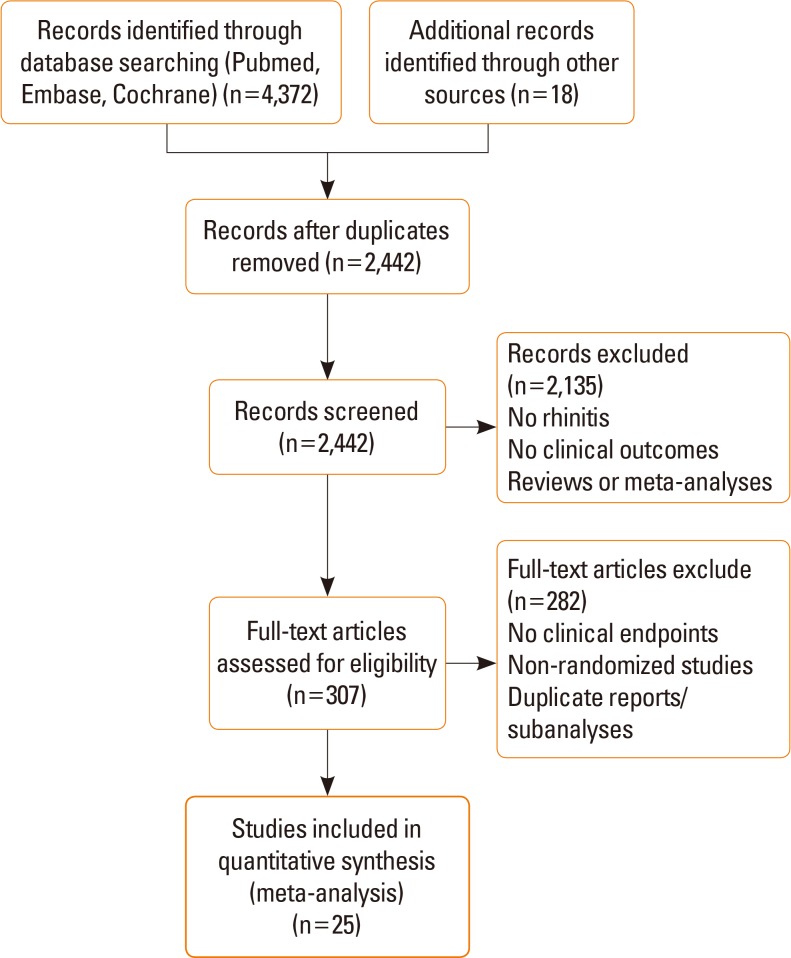
Briefly, of the 4,390 citations retrieved initially through the search algorithm, we finally included 25 eligible clinical trials21222324252627282930313233343536373839404142434445 assessing 3,674 randomized patients. The trials that we excluded from the meta-analysis were not RCTs; moreover, reports that were duplicates and studies with unsuitable data were excluded (Fig. 1).
Population and study characteristics
The characteristics of the included studies are summarised in Table 1. The trials were published from 1990 to 2016. The majority of the trials assessed patients of primarily European backgrounds (13 studies, 2,845 participants). Other patient backgrounds included Eastern Asia (5 studies, 590 participants), Western Asia (5 studies, 149 participants), Oceania (1 study, 30 participants), and Africa (1 study, 60 participants). The largest trial included 992 participants. The SLIT used in the studies in different units was standardized; 19 trials provided the allergens in drops, and 6 provided them in tablets. The period of study drug or placebo administration ranged from 6 to 36 months. The remaining 12 trials only included pediatric patients, with ages ranging from 3 to 18 years. Regarding the studies, patients were sensitised to house dust mites (Dermatophagoides farinae or Dermatophagoides pteronyssinus), cats, or dogs. The prevalence of AR-related comorbidities differed among the included studies. The cumulative doses were variable and measured in different units. Most studies were of high quality and double-blinded, and intention-to-treat analyses were conducted in four such studies. The risk of bias for all studies is shown in Fig. 2 and summarised in Fig. 3.
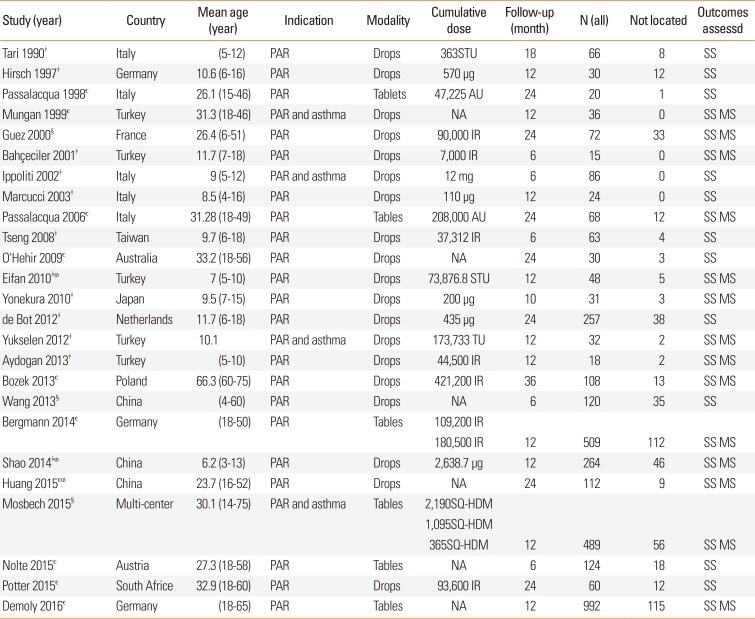
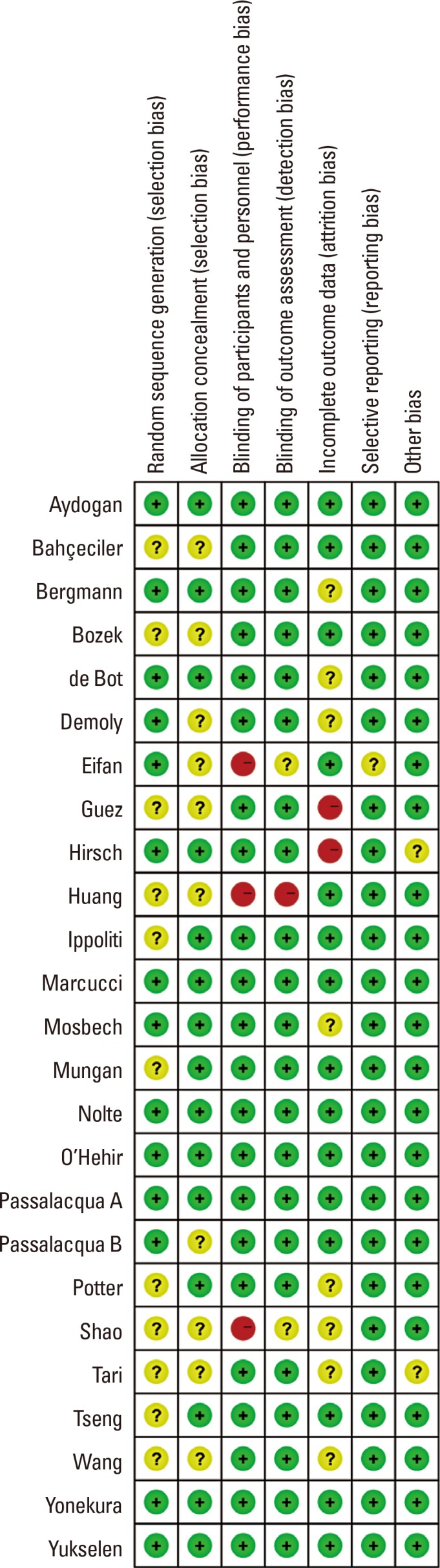
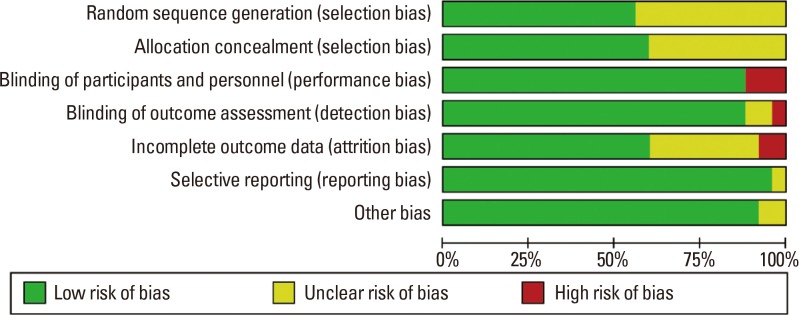
Table 1
Characteristics of the included studies
‡Study only included pediatric patients; єStudy only included adults; §Study included both children and adults; ⱷOpen-label randomized controlled trial.
PAR, perennial allergic rhinitis; AU, allergic units; IR, index of reactivity; STU,specific treatment units; SQ-HDM, standardized quality HDM; TU, treatment units; mg, milligram; ug, micrograms; N, sample size; SS, symptom score; MS, medication score.
![]()
Patient adherence
In the overall population, 539 (14.6%) patients discontinued treatment. Treatment discontinuation was due to adverse events (AEs) in 109 (3.0%) patients, lack of compliance in 70 (1.9%), loss to follow-up in 75 (2.0%), and poor efficacy in 33 (0.9%). Two trials did not provide data regarding discontinuation.3941
Assessed outcomes and evidence synthesis
Symptom scores
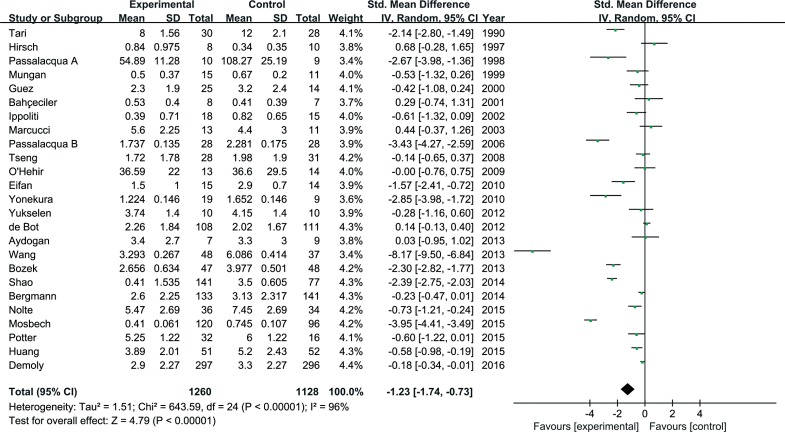
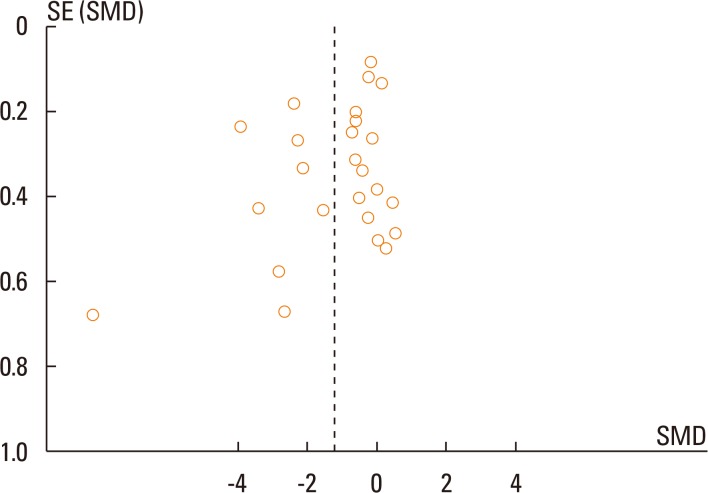
The 25 studies provided enough data to allow a quantitative evidence synthesis based on the symptom scores. Overall, SLIT statistically significantly reduced the daily nasal severity symptom score (SMD=1.23; 95% CI=1.74 to 0.73; P<0.001; Fig. 4), indicating a 1.24 decrease in symptom scores. Significant heterogeneity was found among the studies. Visual inspection of the funnel plot indicated asymmetry (Fig. 5).
Medication scores
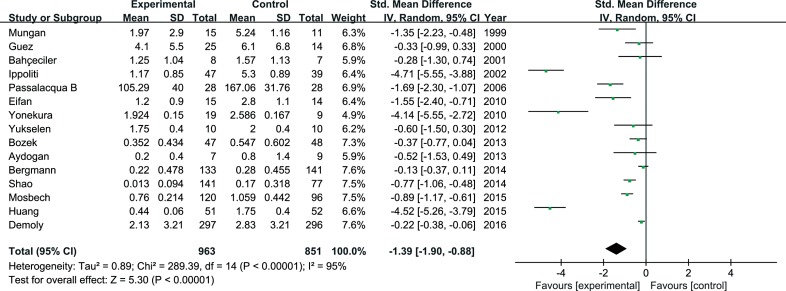
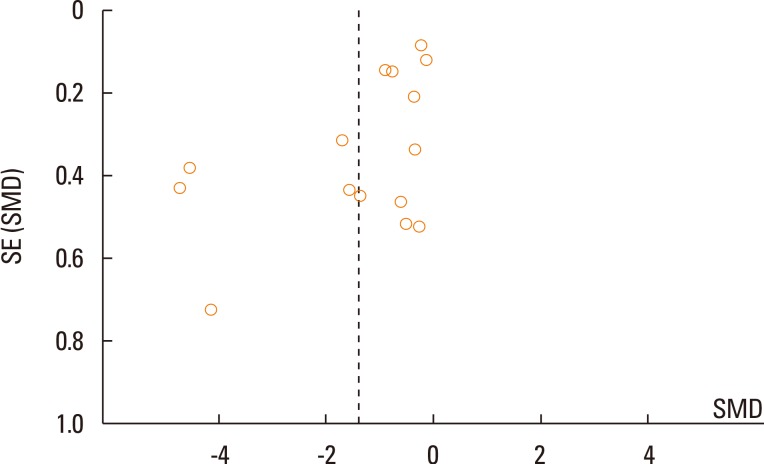
The type of rescue medication varied across the included studies: systemic antihistamines (available in all studies), naphazoline nitrate as a decongestant, topical antihistamines, topical nasal corticosteroids, and systemic corticosteroids. Information on the use of rescue medication was available in 18 studies. Nevertheless, the tools used to assess the use of rescue medication differed substantially among studies. Overall, SLIT reduced the use of rescue medication (SMD=-1.39; 95% CI=-1.90 to -0.88; P<0.001; Fig. 6), corresponding to a 1.12 reduction in the SD for the assessed scores. Significant heterogeneity was found among the studies. Visual inspection of the funnel plot indicated asymmetry (Fig. 7).
Subgroup and sensitivity analysis
We performed a subgroup analysis, evaluating the trials that used SLIT with different modalities. The reduction in symptom scores was significant with tablets compared with drops. Analyses of children who received SLIT did not show a significant effect on symptom scores (Table 2).
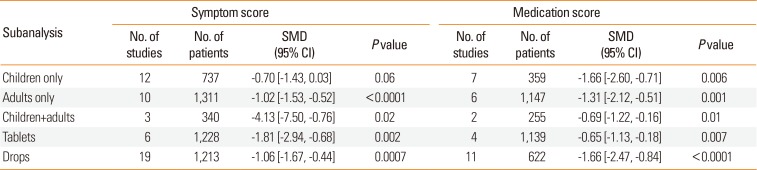
Table 2
Subgroupanalysis of efficacy according to treatment characteristics
![]()
Post hoc sensitivity analyses using the fixed effects model did not substantially change the overall significance for AR symptoms or medication scores. When a sensitivity analysis was conducted in which small studies (n<30) were excluded, we did not find significant changes in any primary outcome of AR. Analogous results were obtained when excluding open label trials for AR symptoms and medication scores. Excluding those studies with dropout rates higher than 20%, the reduction was statistically significant for AR symptoms and rhinitis medication (Table 3).

Table 3
Sensitivity analysis of efficacy
![]()
Publication bias
Funnel plots showed some visual indications of asymmetry for SLIT symptom scores and medication scores. Egger regression produced P values of 0.046 and 0.061 for SLIT symptom scores and medication scores, respectively. Thus, the regression did not provide evidence of publication bias for the studies investigating SLIT medication scores; however, there was evidence of potential publication bias or asymmetry for SLIT symptom scores. The number of studies (25 for symptom scores and 15 for medication scores) also could limit the power of the Egger regression.
DISCUSSION
The present systematic review and meta-analysis was based on 25 RCTs examining the efficacy of SLIT for perennial AR that included 3,631 patients. In 2009, Compalati et al.20 published the first–to our knowledge–meta-analysis examining SLIT for PAR, mentioned limitations and the contrasting results, recommended the more persuasive data are required. Our meta-analysis showed that, in perennial allergic rhinitis, treatment with SLIT provides an improvement of AR symptoms (SMD=1.23; 95% CI=1.74 to 0.73; P<0.001) and a reduction of symptomatic medication use (SMD=1.39; 95% CI=1.90 to 0.88; P<0.001) compared with placebo. Although a review46 of studies found no consensus on basic treatment parameters and questioned the efficacy of SLIT, a considerable number of our included studies support our results. Moreover, multiple systematic reviews474849 have resulted in recommendations for the use of SLIT in the management of perennial AR. The author of a recent review49 also highlighted evidence supporting the efficacy of SLIT in the management of allergic respiratory diseases.
From forest plots for the subgroup of age (Supplementary Figure, we detected SLIT produced significant reductions in adult patients with AR, but not in children (P=0.060). Interestingly, if open-label randomized controlled trials were excluded, this tendency should more obviously (P=0.160). This may be due to the following reasons, suggested in the publications included in the present analysis: lack of effectiveness due to low dosage, poor compliance of children, and the small numbers of patients. The authors of another review50 argued that the severity of disease in patients included in some studies was insufficient to enable the detection of treatment effects. Thus, as has been suggested,46 more trials are needed for the development of recommendations regarding the use of SLIT for pediatric AR caused by dust mites.
The results of subgroup analysis demonstrated that SLIT administration in drop (P<0.001) or tablet (P=0.002) form resulted in significant differences in symptom scores. Most SLIT tablet studies showed significantly reduced AR symptoms. However, many of the included SLIT drop studies were unsatisfactory in terms of symptom scores. Doubtless, the immunologic mechanism of different SLIT modalities (drops and tablets) is similar, and the efficacy depends on allergen type, maintenance and cumulative dose. The information obtained from the literature on SLIT drop studies suggests they are undesirable, may due to the dosage is not applied under guidance and the short duration of immunotherapy-treatment period. Moreover, SLIT tablet studies are associated significantly with symptom relief and decreased rescue medication use in PAR. Unfortunately, the number of SLIT tablet studies is limited (n=6), so the efficacy of SLIT tablets requires further verification in additional, larger clinical trials, as suggested by others.4648
Immunotherapy is generally considered more effective in monosensitised than polysensitised patients. Our meta-analysis confirms this point of view because almost all studies of polysensitised children show insignificant results in terms of efficacy.
Reported treatment-related AEs occurred at comparable rates in patients receiving SLIT and a placebo. Oral pruritus and throat irritation were the most common treatment-related AEs, and no case of malignancy was reported. One review47 showed that SLIT was safer than SCIT, with no death reported during 23 years of testing and clinical use. Although anaphylactic reactions fall within the range of rare, life-threatening events, very large samples are required for their appropriate assessment, and their quantification requires the use of passive and active surveillance systems.
Our study has certain limitations. Initially, differences in the baseline severity of perennial AR, the prevalence of patients with respiratory allergic complications, the scores used for assessment, pharmaceutical preparations, and SLIT protocols among studies compromised comparability and may have limited the accuracy of this meta-analysis. For this reason, we used a robust measure (SMD) to control outcome diversity. To reduce bias due to inter-study heterogeneity, we used a random effects model. Furthermore, language and publication biases should be considered in analyses of efficacy trials. In our study, publication bias may have been attributable to the preferential publication of positive results, bias against the publication of negative results, and analyses of small samples in RCTs. Additionally, caution should be exercised in interpreting the results because the sensitivity analysis erased the statistical significance. Lastly, although the majority of eligible trials were double-blinded and placebo-controlled, the reporting of measures taken to safeguard the blinding process was far from adequate in the trials analysed, resulting in considerable uncertainty regarding important methodological aspects of these studies.
This meta-analysis demonstrates that SLIT was associated with significant symptom relief and decreased rescue medication use in patients. Finally, we stress the concept that SLIT for perennial AR would be more effective with homogeneity. Moreover, we assessed large numbers of clinical trials and explored the effects with statistics, objectivity, and consistency. Additional, large clinical trials are needed to address the effective doses of HDM allergen extracts.
 XML Download
XML Download