

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a heterogeneous condition with variability in the clinical expression of disease, disordered airway physiology, inflammation, and frequency of exacerbations.1234 It affects over 300 million people worldwide.12 To develop effective therapies for asthma, its mechanisms, pathogenesis, and progression need to be better understood. Cytokine profiles have provided insights into potential underlying mechanisms and responses to therapy in asthma and chronic obstructive pulmonary disease (COPD).456789 Sensitization to Aspergillus fumigatus and culture in sputum samples are associated with increasing severity of disease and airflow limitation in asthma.1011121314 However, the sputum cytokine profile in A. fumigatus culture-positive asthmatics is unknown.
We hypothesized that the sputum cytokine profile is different in asthmatics with sputum-positive versus sputum-negative culture for A. fumigatus. To test this hypothesis, we studied moderate-to-severe asthmatics during stable disease in a single center to determine the relationship between the sputum inflammatory profile and A. fumigatus culture.
Go to : 
MATERIALS AND METHODS
Subjects
In this study, 52 adults with moderate-to-severe asthma, according to the Global Initiative for Asthma (GINA) treatment step,1 were recruited from a single center University Hospitals of Leicester NHS Trust, Leicester, UK. Some had participated in a previous cross-sectional study.5 The diagnosis of asthma was made by the subjects' physician consistent with the GINA guidelines and assessed at stable visits at least 8 weeks free from an exacerbation, which was defined as an increase in symptoms necessitating a course of oral corticosteroids and/or antibiotic therapy. All subjects provided written informed consent, and the studies were approved by the local Leicestershire, Northamptonshire and Rutland ethics committee.
Clinical assessments
Demographic, clinical, and lung function data were recorded, which included pre- and post-bronchodilator forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), asthma control questionnaire (ACQ), and symptom scores using the visual analogue scale (VAS). Fractional exhaled nitric oxide was measured, and sputum samples were collected. Sputum plugs were processed to generate cytospins for the assessment of sputum total and differential cell counts.56789 Sputum cell-free supernatants were stored at -80℃ for later mediator analysis. Blood total IgE levels were measured using the ImmunoCap 250 system (Phadia, Milton Keynes, UK). Atopy was assessed by either skin prick testing (Alk-Abello, Horshøln, Denmark) or by blood specific IgE antibody levels (Phadia) and included cat, dog, timothy grass, Dermatophagoides pteronyssinus, and A. fumigatus.
Sputum and blood mediator measurements
A panel of inflammatory mediators was measured in sputum supernatants using the Meso Scale Discovery Platform (MSD®, Gaithersburg, MD, USA) and ELISA as previously described.589 Samples with mediator concentrations below the limit of quantification (BLQ) were assigned half of the limit of quantification. In addition, mediators that were below limit of quantification in more than 60% of the subjects participated in this study were excluded from further analysis.
Bacterial and fungal culture
Standard routine culture to derive the number of colony-forming units (CFU) was performed according to the Health Protection Agency standard operating procedures.15 Quantitative real-time polymerase chain reaction (RT-qPCR) was used to estimate bacterial load based on the abundance of 16S ribosomal subunit encoding genes as previously described.8 The lower limit of quantification was 1×104 genome copies/mL.
Fungal culture was performed as previously described.121416 In brief, undiluted sputum plugs were inoculated onto potato dextrose agar plates containing 16 µg/mL chloramphenicol, 4 µg/mL gentamicin and 5 µg/mL fluconazole; incubated at 37℃ and inspected daily for up to 7 days. A. fumigatus colonies were identified by colony formation and microscopy.
Statistical analysis
Statistical analysis was performed using STATA/IC version 13.0 for Windows (Stata Corp, College Station, TX, USA). The demographic and clinical characteristics, and the patterns of the inflammatory mediators were compared across subjects with and without A. fumigatus. Parametric data are presented as mean with standard error of the mean (SEM), and log-transformed data as geometric mean with 95% confidence intervals (CI). Receiver operating characteristic (ROC) curves were used to determine which inflammatory mediators discriminated between asthmatics with positive versus negative A. fumigatus culture, both significantly and with a ROC area under the curve >0.65. A P value of less than 0.05 was considered significant.
Go to :
RESULTS
The demographic and clinical characteristics were compared across the subgroups with versus without A. fumigatus as shown (Table 1). There were no significant differences between the asthmatics with positive A. fumigatus culture versus without in terms of demographics, symptoms, asthma quality of life, or lung function. The bacterial load assessed by either CFU or total 16S was also not significantly different between the groups.
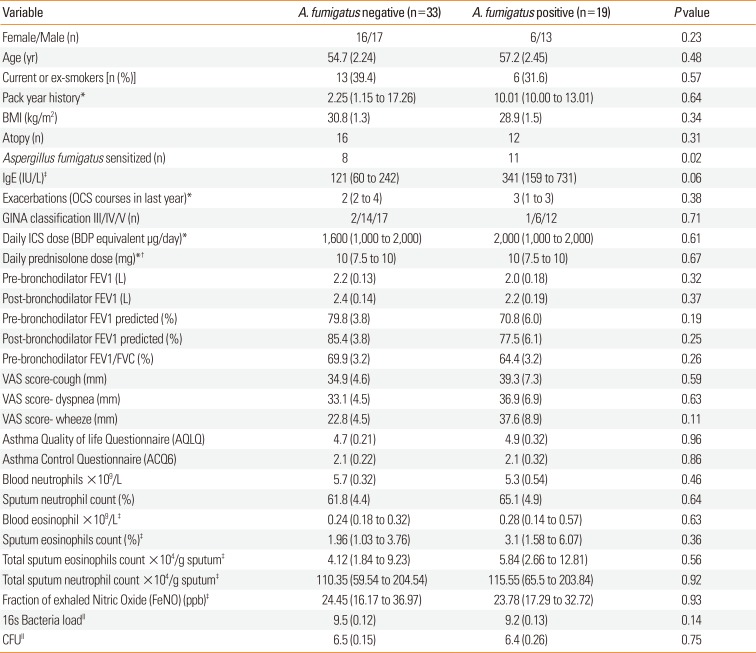
Table 1
Clinical Characteristics in asthmatics with and without positive sputum A. fumigatus culture
Data are presented as mean (standard error of mean [SEM]) unless stated; pack year history for current and ex-smokers.
*Median (first and 3rd quartiles); †dose of prednisolone in those receiving prednisolone; ‡geometric mean (95% CI); ∥logarithmic scale (base 10).
OCS, oral corticosteroid; ICS, inhaled corticosteroid; BDP, beclomethasone dipropionate; VAS, Visual analogue score; BMI, Body Mass Index; FEV1, Forced Expiratory Volume in the First Second; FVC, Forced Vital Capacity.
![]()
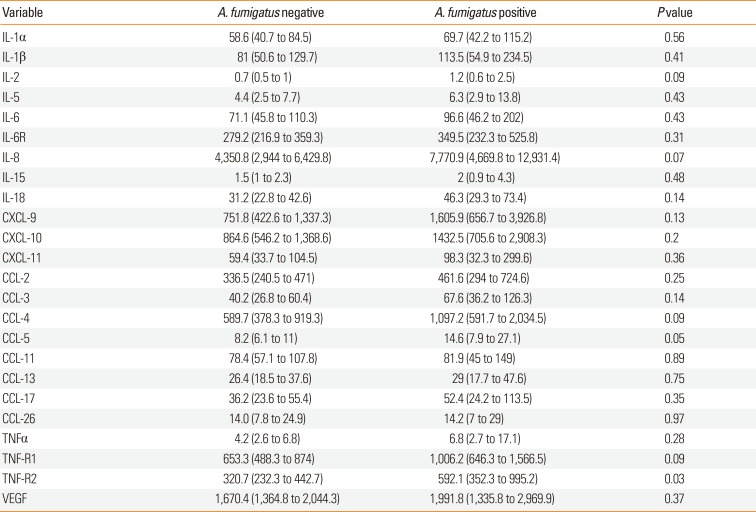
The sputum mediator concentrations in asthma subjects with and without A. fumigatus-positive culture are shown in Table 2. All the mediators were numerically increased in subjects with positive versus negative A. fumigatus culture (24 vs 0, P<0.001), with sputum TNF-R2 increased significantly (Figure). The best predictor of positive versus negative A. fumigatus culture was TNF-R2 (ROC area under the curve 0.66 [95% CI: 0.51 to 0.82, P=0.045]).
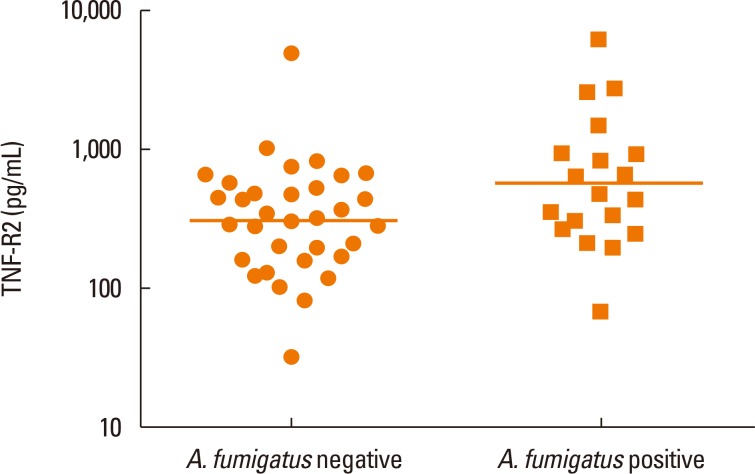 | FigureSputum TNF-R2 concentration (plotted on a log scale) in subjects with or without positive A. fumigatus culture.
|
Table 2
Geometric mean (95% confidence intervals) sputum mediator concentration (pg/mL) in asthmatics with and without positive A. fumigatus culture
![]()
We further categorized the subjects into 4 groups according to the by presence or absence of A. fumigatus sensitization and culture. Comparing the 4 groups by ANOVA and then by pairwise comparisons, we found no significant differences in the sputum cytokines between the subjects that were culture-positive and sensitization-positive versus those that were both culture-and sensitization-negative (data not shown).
Go to :
DISCUSSION
We report here from a single center the sputum cytokine profile for moderate-to-severe asthmatics with or without positive culture for A. fumigatus. We found that although there were no differences in the clinical characteristics between the groups, sputum TNF-R2 concentrations were elevated in those with positive sputum A. fumigatus culture.
In keeping with earlier reports in asthma-positive culture for A. fumigatus was common and detected in 36% of moderate-to-severe asthmatics.12 Positive culture for A. fumigatus and moreover sensitization in asthma and COPD are associated with airflow limitation.111214 Here, we observed no significant difference in spirometry between subjects with or without positive culture for A. fumigatus, although our sample size was small and may have reduced our ability to detect a significant difference. Consistent with other reports, we did not demonstrate differences in demographics or symptoms. Reports of an association between positive culture for A. fumigatus with sputum neutrophilic inflammation in asthma are inconsistent,1112 with one further report of an association in COPD.14 Here, we observed no significant differences between groups for differential or total neutrophil counts.
We have previously described that sputum cytokine profiles in both asthma and COPD clustered into 3 groups consisting predominately of T1, T2, or pro-inflammatory cytokines.59 We observed no significant differences in T1 or T2 cytokines between the groups. However, all of the sputum mediators were numerically increased in subjects with a positive culture for A. fumigatus. The soluble receptor TNF-R2 was significantly increased in the subgroup with a positive culture for A. fumigatus. The TNF-α-converting enzyme TACE can cleave membrane-bound TNFR1 and TNFR2 to yield soluble TNF receptors, which have higher affinity for TNF-α. Thus, in asthma elevated sputum TNF-R2 might attenuate the inflammatory response to A. fumigatus.17
Consistent with our report in COPD, positive culture for A. fumigatus was not associated with increased bacterial colonisation.14 This suggests that the mechanisms increasing susceptibility to either bacterial or fungal colonisation are independent and that an underlying common impairment in the innate immune response is unlikely.
This report has some limitations. Importantly, this is a relatively small cross-sectional study in a single center and requires further validation in larger groups of subjects. Sputum mediator assessments are challenging; however, we have extensively validated these measurements and are therefore confident that the findings are robust. Although our group has carefully optimized fungal culture techniques in sputum samples, new molecular approaches to mycology are under development and future studies will need to include these new technologies. In addition to considering the full mycobiome, the fungal load determined by spore count might be clinically important and should be included in future studies.18
In conclusion, we have found that sputum inflammatory cytokine concentrations were collectively increased in moderate-to-severe asthmatics with positive culture for A. fumigatus. Anti-fungal therapy has benefit in allergic bronchopulmonary aspergillosis (ABPA), although possibly due to its effects on corticosteroid pharmacokinetics.219 Anti-fungal therapy in asthma beyond ABPA is contentious with inconsistent evidence from randomized controlled trials.22021 Whether anti-fungal therapy may be more effective in asthmatics with evidence of positive culture for A. fumigatus and increased airway inflammation warrants further investigation.
Go to :
 XML Download
XML Download