

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hypersensitivity to fungi is associated with rhinoconjunctivitis and asthma.1,2 This association was described in 1,726 by Floyer in asthmatic patients visiting a winery.3 Other allergic diseases are allergic fungal sinusitis, allergic bronchopulmonary aspergillosis, and extrinsic allergic alveolitis.
In the case of A. alternata, the symptoms of asthma are persistent, thus increasing disease severity and the risk of fatal outcomes.4 This has implications for the clinical management of patients, and these diseases have substantial social and economic repercussions.
A. alternata spores and mycelium are the primary source of sensitization, although other fungal particles derived from them may also reach the respiratory system of the allergic patient.5 Their almost permanent presence, both in the atmosphere and in dwellings6 depends primarily on the environmental, climatic, and topographic conditions, and the sources that the fungus colonizes.7
The reported prevalence of A. alternata varies widely according to the geographical location (ranging from 3% in the Nordic countries to 20% in the Mediterranean environment) and the methodology used.8 The prevalence is gradually increasing, with children being especially affected.9
In dwellings and interior environments, species such as Stachybotrys chartarum (S. chartarum) are generally receiving increasing scientific interest due to the severity of the symptoms caused by the mycotoxins released10 and as the cause of the so-called sick building syndrome. The aims of this study was to determine hypersensitivity to fungi in dwellings in patients from Cuenca, Spain, and to study polysensitization and cross-reactivity due to the known sensitization to various species, and the recognition of allergens belonging or not to a same group species from the same taxonomic family.11
MATERIALS AND METHODS
Patients
Patients were selected randomly and prospectively. Inclusion criteria were clinical demonstration of the signs and symptoms of rhinitis or rhinoconjunctivitis and/or associated mild-to-moderate asthma of ≥1 year of evolution and a positive skin prick test (>3 mm wheal) and positive specific IgE levels (≥0.35 kU/L, class 1; ThermoFisher Scientific, last Phadia, Uppsala, Sweden) to various species of fungal extracts. All patients included provided signed informed consent to participate in the study.
Home collection and identification of fungal samples
Fungal samples were obtained from each dwelling (home or workplace suspected of involvement in the symptoms). Samples were identified by the Department of Microbiology, Immunology and Parasitology (University of the Basque Country, Vitoria, Spain) (Fig. 1).
Allergenic sources and extracts
The natural sources of raw materials containing spores and mycelia of Candida albicans (C. albicans), U. botrytis, Mucor mucedo, Fusarium sp, Trichophyton rubrum, Aspergillus niger, A. alternata, S. chartarum, S. botryosum, Penicillium notatum (P. notatum), Rhizopus sp, Aspergillus fumigatus (A. fumigatus), Botrytis sp, and Cladosporium herbarum (C. herbarum) were supplied by Allergon (Allergon, Ängelholm, Sweden), Greer Lab., (Lenoir. USA) and the Departments of Microbiology, Immunology, and Parasitology (University of the Basque Country, Vitoria, Spain).
Proteins from the above-mentioned raw materials were obtained after prior homogenization and subsequent extraction in Coca buffer, under magnetic agitation at 4℃ for 5 hours. The soluble fractions were centrifuged at 8,400 g×30 minutes. at 4℃. The supernatants were subjected to filtration, dialysis (7,000 Da), and subsequent lyophilization.
Skin prick tests
All patients underwent a skin prick test according to standard procedures and a standard battery of fungal extracts (Diater Laboratories, Madrid, Spain).
Standardization of U. botrytis extract
The activity of the allergenic extract of U. botrytis was measured in biological units (10,000 BU/mL), after obtaining the median skin reactivity produced at different concentrations, and compared with a reference solution of histamine dihydrochloride at 54.3 mmol/L (10 mg/mL) in at least 20 sensitized patients, according to the method of Aas12 modified by Malling13 and after conforming to the assumptions of the methodological study by Dreborg14 which, together, are the method recommended by the recent EMEA Guideline on Allergen Products: Production and Quality Issues (EMEACHMP/BWP/304831/2007) which regulates this type of products in the EU.
Briefly, the histamine equivalent prick (HEP) value from the selected population was obtained according to the application of four 10-fold concentrations of allergen together with the histamine reference solution, on the volar surface of the forearm of each patient by duplicate. The area of the wheal was measured with a digitizer by following the contour lines. The dose-response relationship of the allergen was estimated by linear regression analysis using the geometric mean of the 2 wheal areas obtained with each concentration, in a double-logarithmic system. The concentration of allergen estimated to provoke a response with the same wheal area as the histamine reaction (geometric mean of the 2 wheal responses caused by histamine) is then calculated from the regression line formula. The median value based on all patients tested represents the concentration of the allergen preparation corresponding to 10,000 BU/mL.
Specific IgE and histamine release tests
The levels of specific IgE to U. botrytis and Alt a 1 were measured using the CAP system (ThermoFisher Scientific, last Phadia, Uppsala, Sweden). The levels ≥0.35 kU/L were considered positive. The binding capacity for specific IgE protein extracts of C. albicans, U. botrytis, Mucor mucedo, Fusarium sp, Trichophyton rubrum, Aspergillus niger, A. alternata , S. chartarum, S. botryosum, P. notatum, Rhizopus sp, A. fumigatus, Botrytis sp, and C. herbarum were determined by IgE immunoblotting and Dot blot analysis.
Quantification of Alt a 1 and cross reactivity tests
The presence and content of Alt a 1 in extracts of A. alternata, U. botrytis, S. botryosum, A. fumigatus, C. herbarum, and P. notatum were measured using the ELISA quantification kit for Alt a 1 (INDOOR Biotechnologies, Charlottesville, VA, USA). For this quantification, a polyclonal antiserum Alt a 1 obtained by immunization of a New Zealand rabbit17 with rAlt a 1 in complete Freund's adjuvant18 according to the protocol of Gallart et al. was also used.17 Polysensitization and/or cross-reactivity of the extracts tested was measured by ELISA inhibition assays, according to the method of Ceska and Lundqvist19 with modifications.
2D-electrophoresis, 2D-immunoblotting, and sequencing
The orthologous allergen of Alt a 1 in the extract of U. botrytis was identified by choosing the closest to the reference point in terms of the molecular weight and the isoelectric point after performing 2D electrophoresis and IgE-2D-immunoblotting. The point recognized by the sera of patients was subjected to sequence analysis by peptide mass fingerprinting (MALDI-TOF-MS) and MS/MS analysis (Proteomics Center, Faculty of Pharmacy, University Complutense of Madrid, Spain). Trypsin digestion was made using the method of Shevchenko.20 The peptide fingerprint was obtained using MALDI-TOF-MS21 and de novo sequencing by MS/MS according to the method of Gautam et al.22
RESULTS
Study population and selection of the most prevalent species
There were 35 male or female patients. They had (1) a mean age of 15 years (7-32 years), (2) symptoms compatible with rhinitis or asthma showing clear worsening of their symptoms in their dwellings or workplaces where damp areas were identified in walls or ceilings, and (3) positive skin prick tests and specific IgE (≥0.35 kU/L) to U. botrytis, A. alternata, A. fumigatus, and C. notatum (Table 1).
U. botrytis and A. alternata were the most representative species as sources of sensitization in these dwellings.
Skin tests and biological standardization of U. botrytis
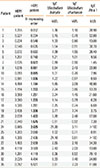
To determine the conventional parameters of biological activity in vivo and allergenic potency in vitro of extracts of U. botrytis, biological standardization was carried out. Of the 35 patients included, 26 were selected according to the inclusion criteria regarding the papules obtained with different concentrations of the allergen extracts used. The 95% confidence limits of the population were determined between the values of HEP of patients 8 and 19 (0.88 and 2.02 mg/mL, respectively).
The HEP value obtained from the U. botrytis extract corresponded to the median individual HEP values in the 26 selected patients and was 1.25 mg/mL (Table 2).
Allergenic profiles
Fig. 2 shows the allergogram of the selected allergen extracts under reducing and nonreducing conditions, revealed by pooled sera, high, medium and low specific IgE of selected patients in the standardization of U. botrytis. The main bands observed, with an approximate weight of 29 kDa (under nonreducing conditions), appeared in the extracts of U. botrytis, A. alternata, and S. botryosum.
The Dot blot in Fig. 3A shows the IgE-binding capacity to recognize different species of fungi, with a positive reaction to samples of U. botrytis, A. alternata, and S. botryosum and, to a lesser degree, A. fumigatus and C. herbarum. Fig. 3B shows the IgE-binding capacity of U. botrytis and A. alternata in each patient, and shows a band of about 15-17 kDa that appeared in all the samples.
Allergenic potency and cross-reactivity
To determine whether the reactivity of sera to different fungal species is due to cross-reactivity or polysensitization, we determined Ag50 values for each fungal extract by ELISA inhibition (see Fig. 4A). The Ag50 value of U. botrytis extract was 6.029 µg/mL, while those for A. alternata and S. botryosum were 3.604 and 25.373 mg/mL, respectively. No inhibition was observed for A. fumigatus or C.herbarum (Fig. 4B).
Taking into account the fact that the allergen Alt a 1 is the most important allergen described in A. alternata and is possibly what most patients react to, we decided to study its capacity to inhibit binding of IgE to extracts of various fungi. Western blot analysis in Fig. 5 shows the inhibitory capacity of Alt a 1 on the specific IgE versus the allergens of the extracts of C. albicans, U. botrytis, A. alternata, S. botryosum, P. notatum, A. fumigates, and C. herbarum. Alt a 1 inhibited its homologue in the extracts of A. alternata, U. botrytis, and S. botryosum.
2D-electrophoresis, 2D-immunoblotting, and sequencing
To confirm the presence of Alt a 1 in the extract of U. botrytis, we carried out 2D-electrophoresis, which showed the presence of a protein of 15 kDa and a pI around 4.5 (Fig. 6A), compatible with the orthologue of Alt a 1 in U. botrytis. Immunoblotting showed the presence of a protein of approximately 17 kDa with a pI of around 4.5, compatible with the orthologous allergen of Alt a 1 in the extract of U. botrytis, recognized by the pooled sera (Fig. 6B1), and a high, medium and low specific IgE values of selected patients (Fig. 6B2, B3, and 6B4).
To identify the possible homologous protein of Alt a 1, this was extracted from SDS PAGE gel and analyzed by MS sequencing. The amino acid sequence coincided in 24% (sequence coverage) with the orthologue allergen of Alt a 1 expressed below (in red):
1 MQFTTIASLF AAAGLAAAAP LESRQDNASC PVTTK 
51  ATNGGTL DFTCSAQADK LEDHKWYSCG ENSFMDFSFD
ATNGGTL DFTCSAQADK LEDHKWYSCG ENSFMDFSFD
ATNGGTL DFTCSAQADK LEDHKWYSCG ENSFMDFSFD
101 SDRSGLLLKQ KVSDE
Histamine release
To evaluate the ex vivo behavior of the allergenic extract used in the skin tests, histamine release tests were made using samples from the 26 patients selected in the skin tests. Basophils were stimulated with extracts of U. botrytis and Alt a 1. The results (see Fig. 7) showed a good correlation between the results obtained with both stimuli.
Quantification of Alt a 1
We then determined the presence and content in Alt a 1 in the extracts of A. alternata, U. botrytis, S. botryosum, A. fumigatus, C. herbarum, and P. notatum by ELISA. The content of Alt a 1 in extracts of A. alternata, U. botrytis, and S. botryosum was 895 ng/mg, 85 ng/mg, and 18.29 ng/mg, respectively, of the total extract. Alt a 1 was not detected in A. fumigatus, C. herbarum, and P. notatum.
DISCUSSION
Currently, more than 3 billion people worldwide are infected by parasites (worms) or suffering from allergic diseases that affect the respiratory tract (asthma and rhinitis), skin (dermatitis, urticaria, and eczema), and different expressions of sensitivity to food and medicine that are considered impaired Th2-(Th2) immune responses.23
The diagnosis of these disorders is essentially based on a combination of (1) etiological identification tests that show the presence of the source of sensitization in the patient's environment and the possible cause and effect, (2) the patient's medical records, and (3) in vivo and in vitro diagnostic tests.24 Diagnostic tests require allergenic extracts, and the results obtained will depend on their quality.25 Allergenic extracts are therefore indispensable tools for the diagnosis and treatment of allergic diseases and research on processes involved in this inflammatory phenomenon.26
In the specific case of allergy to fungi, the problem is compounded due to the wide variety and polymorphisms of species, and the high variability of these organisms which is manifested in different compositions and potency of allergenic extracts obtained, even from those of the same strain. Therefore, the diagnosis is complicated because, in many cases, there is no correlation between the source of sensitization and the possible etiologic diagnosis: this means that diagnostic tests often do not show the efficacy, in terms of sensitivity and specificity, obtained with other allergens.8
The present study analyzed a sample of patients with suspected sensitization to fungi in the home or work environment. The allergenic extracts of fungi used in the study were selected according to aerobiological and incidence studies of the most important reported species,8,27,28,29 including some emerging species, such as S. chartarum.30
The allergenic extracts used underwent the internal procedures of biological standardization and quality control recommended by accepted guidelines.12 The results of serological titration of specific IgE of both Ulocladium species (U. botrytis and U. chartarum) were almost the same, implying that allergenic variation at the species level does not show significant differences.31
Our results suggest that the allergen Alt a 1 of A. alternata could be considered a non-species-specific allergen which could be used as a diagnostic source of sensitization to some species of the pleosporaceae family.
A study by Twaroch et al.32,33 of 80 patients allergic to A. alternata showed recognition of rAlt 1 in 98% of cases, a percentage similar to that found by Asturias et al.34 in a cohort of 42 patients, most of whom recognized the major allergen of U. botrytis, the homologue of Alt a 1, similar to the already described Ste b 1 of S. botryosum, suggesting that Alt a 1 could be used as a marker for sensitization to A. alternata and other species of the Pleosporaceae family, and could replace whole extracts of these species.
Patients who do not recognize Alt a 1 may be recognizing other reported orthologue allergens, such as Alt a 6 and Alt a 14 (MnSOD),35 which like other allergens from fungal species, such as Asp f 4 and Asp f 6, are discriminators of bronchopulmonary aspergillosis and sensitization to Aspergillus, and which could like Alt a 1 and homologues, report and discriminate aspects, such as the greater frequency of asthma in patients sensitized to A. alternata compared to those not sensitised.36
The biological standardization of the allergenic extract of U. botrytis made in this study allows correct etiologic diagnosis and concordance between the identification of the presence of the source of sensitization in dwellings and the perennial, non-seasonal nature of these sources to be established.
Another factor in determining allergenic sources, especially fungi, is the importance of recognizing an allergen in sensitized patients. However, reactivity to IgE does not necessarily reflect its ability to induce allergic symptoms. Hence, the incorporation of the results obtained can apply for the technique of allergen-specific histamine release and identify their concordance with the results of the skin tests and the detection of specific IgE.







 XML Download
XML Download