

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma and allergic rhinitis are chronic diseases with a steadily increasing prevalence. Worldwide, 300 million people suffer from asthma. In Germany alone, 7,000 people die because of asthma each year. The mortality rate is rising in most countries, and allergy and asthma have become public health problems throughout the world.1
In principle, the allergic immune response results from a misguided immune polarization against proteins and other harmless biomolecules. Allergic sensitization is complex and multifactorial, including a genetic predisposition to mount IgE responses (atopy), exposure to microbial diversity, allergens and environmental pollutants, and even use of antibiotics in infancy.23 Moreover, protein-inherent features, such as protease activity (Der p 1) or MD2 mimicry (Der p 2), contribute to the "allergenicity" of certain molecules.456
HDM allergens are one of the main causes of allergy and asthma, and increased exposure to indoor allergens has been suggested as a possible reason for the general rise in allergic diseases.78910 The most frequent species are Dermatophagoides pteronyssinus (with the major allergens Der p 1 and Der p 2) and Dermatophagoides farinae (with the major allergens Der f 1 and Der f 2). Both comprise mite "group 1" and "group 2" allergens,11 and are common in European and American homes. Usually, HDMs colonize every part of a house, and HDM allergens are chemically stable for many years.1213 The structure and sequence of Der p 1 and Der f 1 are almost identical, thus resulting in a high cross-reactivity and similar effects in patients.14
The concentration of HDM allergens correlates with clinical markers for asthma severity, e.g. peak expiratory flow (PEF) variability, forced expiratory volume in 1 second (FEV1), or bronchial hyperresponsiveness (BHR) in asthmatic patients sensitized to HDMs.15 In general, the higher the allergen exposure, the more patients have positive skin prick tests, but even exposure to lower levels of HDM allergens (20 ng/g) was found to be a significant risk factor for sensitization.16 Since early publications in the 1970s, allergologists have postulated decreased HDM load and HDM allergen concentration with increasing altitude and decreasing humidity,17181920212223 while some publications contradict this interpretation.24252627 Based on the assumption of a negative correlation of altitude and HDM concentration, allergen avoidance therapies for HDM allergy and asthma are offered in alpine regions. High-altitude climate therapy has been shown to positively affect medical parameters and symptoms of patients suffering from allergic airway diseases. Clinical studies verified that a stay at high altitude improves relevant surrogate parameters for allergy and asthma, such as the reduction in specific IgE levels, improved clinical asthma markers,28 or mitigate nonspecific BHR and epithelial shedding.152930313233
As a second major parameter, relative air humidity (RH, %) was postulated to significantly influence HDM growth, and low indoor RH was recommended to reduce HDM.22333435 However, in recent studies no association between HDM infestation and RH could be detected.363738
Indoor allergens are usually attached to the surface of indoor particulate matter (PM), e.g. fine dust, which supports their transport to the respiratory tract and also acts as a bronchial irritant,39 which may also aggravate the allergenicity of indoor allergens and was therefore measured in all buildings included in this study.4041
The aim of the present study was to revisit the current hypothesis that altitude inversely correlates with the HDM allergen concentration. For that purpose, HDM allergen concentrations were measured at different heights in alpine regions of Austria and Germany, and these data were analyzed in terms of fine dust pollution, temperature, humidity, and parameters of building characteristics and indoor environment.
MATERIALS AND METHODS
Collection of dust samples
A total of 122 dust samples (65 samples below and 57 samples above 1,500 m a.s.l.) were collected from different types of buildings, such as private residences, taverns, and mountain huts, located at altitudes between 400 m and 2,600 m a.s.l in alpine regions of Germany and Austria. All samples were taken during September in 2012 and 2014, which has been reported as the month with the highest concentrations of mites measured in house dust,1942 using a DUSTREAM™ Collector with inserted nylon filter (INDOOR biotechnologiesINC, Charlottesville, VA, USA) attached to a vacuum cleaner. According to the INDOOR biotechnologiesINC protocol, in all 4 corners of a room, as well as a mattress, an area of 21×30 cm was vacuumed for 30 seconds. The samples collected were stored at -20℃ in dust-proof Ziploc bags (Toppits® Ziploc® Vaughan, ON, Canada).
Allergen quantification
Allergens were extracted by adding 2 mL of phosphate buffered saline (PBS) to the dust samples, shaking (at RT/30 min), spinning (3 min/4,000 rpm) and using 50 µL of the supernatant for further measurement. Allergen concentrations were measured using a MARIA 5-plex Multiplex Array for Indoor Allergens (MRA-C5) kit (INDOOR biotechnologiesINC) on a Luminex S-100 (Luminex, Austin, TX, USA) according to the manufacturers' instructions. Concentrations of Der p 1, Der f 1, and allergens of mite group 2 (both Der p 2 and Der f 2) were calculated via polynomial fit of raw fluorescent units into a dilution curve of allergen standards using xPONENT® software and expressed in ng/µL. The limit of detection was 0.06 ng/mL each for Der p 1 and Der f 1, and mite group 2 allergens are detectable up to 0.02 ng/mL.43 We investigated the weight (g) of collected dust of each sample and standardized the concentrations to nanogram allergen per gram of dust (ng/g). Spearman's rho correlation of allergen concentration with altitude, temperature, fine dust, and humidity was calculated using SPSS software (SPSS Inc., Chicago, IL, USA, version 22.0). Comparing of means was done with the Mann-Whitney U Test for independent samples. The relationship of indoor environmental characteristics with the concentration of allergens was calculated using univariate ANOVA and the post hoc Bonferroni test. The limit of significance was set to 0.05.
Environmental parameters
Particulate matter (PM-1, PM-2.5 and PM-10 in µg/m3), temperature, and RH% were measured with a Grimm Model 1.108 Portable Aerosol Spectrometer (Grimm, Aerosol Technik GmbH Co, Ainring, Germany). The spectrometer was positioned at a height of 50 cm in the middle of each room, and a ventilator was arranged for air circulation. The period of measurement covered about 5 minutes per room. The individual values were averaged arithmetically.
In addition, the position of each building was determined via GPS, and data concerning indoor environmental parameters (number of windows, type of glazing, type of flooring, age of building, quantity of linens, type of heating, people per day/night, floor number, number of beds, type and intensity of usage, cleaning method, and frequency) were collected and stored in an iPad® database system (Tap Zapp Software Inc., Calgary, Canada).
RESULTS
Allergen concentrations and height
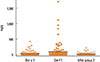
All allergens (Der p 1, Der f 1, and mite group 2) were detectable in 100% of the 122 dust samples collected. The concentration of mite allergens showed high variations. Mite group 2 ranged from 0.01 to 229.12 ng/g (arithmetic mean: 24.49±36.49 ng/g). Der p 1 levels varied from 0.03 to 426.90 ng/g (arithmetic mean: 32.59±63.16 ng/g), and Der f 1 levels ranged from 0.08 to 1,703.69 ng/g (arithmetic mean: 95.04±226.42 ng/g) (Fig. 1). Normal distribution tests failed.
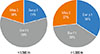
No correlation could be measured between concentrations of the allergens Der p 1 and mite group 2 with the altitude (Der p 1: r=0.088, P=0.334; mite group 2: r=-0.098, P=0.285). Der f 1 showed a weak negative correlation with the altitude (Der f 1: r=-0.319/P<0.001), which may have been due to a markedly higher concentration of Der f 1 in the altitude range below 1,500 m compared to Der p 1 allergen levels (P=0.001). There was a huge percentage disparity of Der p 1 and Der f 1 allergens below 1,500 m altitude (Fig. 2). Concentrations of Der p 1 and Der f 1 allergens did not differ in samples taken above 1,500 m a.s.l. (P=0.689).
No statistically significant difference could be found between allergen concentrations of samples taken above and below 1,500 m a.s.l. of both Der p 1 (P=0.928) and mite group 2 allergens (P=0.127) (Fig. 3). Only Der f 1 was reduced in higher altitude (P<0.001).
In general, mattresses represent a superior biotope for HDM compared to floors. Consistently, allergen concentrations of samples collected from mattresses were significantly higher than those taken from the floors (Der p 1: P=0.001; Der f 1: P=0.005; mite group 2: P=0.017) reflecting a stoichiometric relationship of ~ 2:1 (Fig. 4).
One part of the samples (n=37) was taken from buildings that were only used 6 months a year, at an altitude of 1,750-2,600 m and fully frozen during winter. The other part (n=85) originated from buildings at altitudes of 420-1,650 m, which were occupied all throughout the year. Despite the drastic differences in the living conditions for dust mites in these 2 groups, no significant changes in allergen concentration could be detected for Der p 1 and mite group 2 allergens (Der p 1: P=0.832; mite group 2: P=0.672). Only Der f 1 allergens showed less concentrations in samples taken from buildings closed and unheated during the winter (Der f 1: P=0.005) (Fig. 5).
Allergen concentrations, temperature, and humidity
Air temperature in different buildings ranged from 14.03℃ to 24.96℃ (arithmetic mean: 20.55℃±2.7℃). There was a clear negative correlation of temperature to rising altitude (r=-0.537; P<0.001), but no relationship between temperature and the concentration of mite allergens could be measured (Der p 1: r=-0.133, P=0.201, Der f 1: r=0.027, P=0.799, mite group 2: r=-0.077, P=0.459). There was also a high variation in RH, ranging from 21% to 56% (arithmetic mean: 44.05±8.95%), and RH also showed a clear negative correlation with altitude (r=-0.635; P<0.001). However, in contrast to previous studies, there was no correlation between allergen concentrations and RH (Der p 1: r=-0.158; P=0.129; Der f 1: r=-0.047; P=0.652; mite group 2: r=-0.102; P=0.328) (Fig. 6).
Allergen concentrations, fine dust, and dwelling conditions
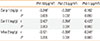
Fine dust PM10 ranged from 5.70 to 468.50 µg/m3(arithmetic mean: 57.49±71.90 µg/m3, PM-2.5 from 1.18 to 56.37 µg/m3(arithmetic mean: 11.44±11.20 µg/m3, and PM-1 from 0.39 to 47.28 µg/m3(arithmetic mean: 7.51±8.60 µg/m3. Indoor fine dust PM values (n=111) showed no correlation with altitude or the weight of collected dust samples. A positive correlation was found for the weight of dust in the collected samples from floors and mattresses with concentration of mite allergens (Der p 1: r=0.359, P<0.001; Der f 1: r=0.398, P<0.001; Mite group 2: r=0.406, P<0.001). Concentrations of mite allergens also showed weak negative correlations with most of the measured PM (Table).
Interestingly, indoor environmental characteristics, such as the type of heating, number of windows and beds, type of glazing, application, quantity of users (day and night), subjective quantity of linens used in the room, age of building or type of ventilation, also showed no association with concentrations of mite allergens. Not even methods or frequencies of cleaning were related to levels of detected allergens. A insignificant difference could be found between different types of floors. Stone floors displayed the lowest allergen concentrations (arithmetic mean: Der p 1: 20.93 ng/g, Der f 1: 11.44 ng/g, mite group 2: 10.86 ng/g), whereas vinyl floors showed the highest concentrations of Der p 1 and mite group 2 allergens (arithmetic mean Der p 1: 56.12 ng/g, mite group 2: 29.30 ng/g). The highest Der f 1 allergen concentrations were found on laminate floors (arithmetic mean Der f 1: 124.83 ng/g).
DISCUSSION
The results of the present study, performed in alpine regions of Germany and Austria, clearly indicate that the concentration of the HDM allergens Der p 1 and mite group 2 does not significantly decrease at high altitude. Moreover, no correlation between altitude, RH, and HDM allergen concentrations could be found. Even in mountain huts at high altitude that were not used in winter and thus were fully frozen at that time, HDM concentrations did not differ from buildings located at lower altitudes which were occupied throughout the year. Similarly, dwelling conditions did not significantly alter the allergen load. Only Dermatophagoides farinae shows a weak negative but significant correlation with rising altitudes. Based on this fact, we assume a higher sensitivity of the American HDM and poorer ability to adapt to changes. The dry and cold air at high altitude may also affect the stability of Der f 1 allergen in comparison with Der p 1 and mite group 2 allergens.
As one would expect, outdoor air pollution at high altitude is generally lower; however, indoor fine dust pollution did not significantly change with altitude. The difference in allergen concentration in the disturbed air and the settled dust could be attributed to the feature of fine dust, binding to allergens on its surface. The higher the particulate matter, the more allergens are hovering in the disturbed air, compared to allergen levels determined in the settled dust on floors or mattresses. This might have a big impact on the health-related quality of life of HDM allergic patients in rooms with high fine dust pollution.
Our data are in line with publications questioning the paradigm "the higher altitude, the lower the allergen concentrations",24252627 which was primarily based on the assumption that a hostile environment to mites accompanied by a reduction in the number of mites (or elimination of mites during winter in frozen buildings) may eliminate the allergens. This biological view may be correct for the mite itself, but its proteins can be stable over a long period of time. Obviously, this is the case with HDM allergens, and high HDM allergen concentrations measured in chalets at high altitude that are frozen for several months a year favor this interpretation. We postulate, that after mites die away, the allergen concentration remains high for a prolonged period, and freezing may even prolong the amount of intact allergens. It has already been shown that mite allergens are chemically stable for up to four years.44 During warmer periods, small populations of mites regenerate, and as people return, more mites are imported, and they deposit "fresh" allergen again. It would be interesting, especially in these specific chalets or mountain huts, to measure the fluctuation in the mite population and the allergen concentration. Due to the mechanism we postulate, the fluctuation in the latter should be low, and in sum the allergen load would be as high as at lower altitudes.
Nevertheless, there is evidence of a salutary effect that accompanies a stay in high-altitude regions for people allergic to HDM, which has been demonstrated in both pediatric4546 and adult patients with allergic and intrinsic, moderate and severe asthma.47 Interestingly, patients with intrinsic asthma also show a reduction in airway inflammation.
Taken together, it is clearly indicated that the mitigating effect of high-altitude climate therapy for allergic asthma can no longer be ascribed to a reduction in HDM allergen in the environment. Other mechanisms remain to be responsible for the beneficial effects. Recent studies address several factors, such as reduced humidity, low endotoxin load, decreased exposure to fungal spores, pollen, and air pollution, which may contribute to the positive influence of high climate therapy on allergic patients and asthmatics.454748 Furthermore, higher air fluidity and lower oxygen concentration at high altitude reduce respiratory resistance and aid in breathing. In addition, increased UV-light exposure can modulate the immune system and holiday-makers visiting high-altitude regions experience a relief from stress during their stay. Also these parameters may have an influence on allergy symptoms and asthma control, comparable to medicinal immunotherapies.4849
The contradictory data concerning the occurrence of HDM, based on altitude and RH, may be partially explained by changes in building construction (modern insulation, heating, and glazing) and climate changes (global warming) since the 1970s.350 However, our data also contradict the widespread assumption that improved isolation of buildings and more frequent heating of rooms, in comparison to previous decades, leads to a higher allergen concentration at high altitude. Again, the HDM concentration in buildings completely frozen during several winter months provides the strongest argument against this postulate.
Similarly, postulations from older papers have to be critically addressed, e.g. it has been reported that HDMs need a RH of 70%-80% to develop, and stop growing and die at a RH of 60% and lower.1933 We measured RH in most of the rooms in which the 122 dust samples were collected for this study. Though the relative air humidity was below 60% in all rooms (n=53), all the samples contained HDM allergens. Whether humidity is not the only and/or major controlling factor for the development and growth of mite populations, or there is a higher RH of the microenvironment of mites, cannot be determined by this study.
Another reason for the differing results in literature may be improved immuno-chemical techniques, which now allow for the targeted detection of very low allergen concentrations in dust samples.
CONCLUSIONS
We provide evidence that HDM allergen levels are not significantly lower in mountainous areas of the alpine region of Germany and Austria. The data indicate that recovery of asthmatics and allergic sufferers during a stay in a high-altitude region is not the result of lacking allergen (allergen avoidance), as has been postulated for several decades. Hitherto unknown mechanisms, possibly triggered by stationary effects or climatic conditions, seem to be responsible for mitigating the allergic immune response, at least its effector phase.




 XML Download
XML Download