

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recurrent wheezing (RW) defined as ≥3 physician-diagnosed wheezing episodes is the main clinical expression of asthma in infants. It is a major health problem (causing a considerable use of health services and medications expenses.123 Furthermore, during the first year of life a high proportion of infants with RW have severe episodes resulting in an elevated frequency of visits to the Emergency Department (ED) and hospital admissions for wheezing,3 evidencing that RW in infants is not a benign condition as usually considered independently of how it will progress later in childhood or adolescence. Despite the magnitude of this health problem, studies regarding prevalence, severity, and treatments of RW in infants are scarce. Several of these wheezy infants, particularly those with troublesome coughing and wheezing, will receive inhaled bronchodilators (IBD), inhaled corticosteroids (ICS), oral corticosteroids (OCS), leukotriene receptor antagonists (LTRA), antibiotics (ATB), and paracetamol (PCM), and others.123 Although there is no information on the frequency of and indications for the prescription of ATB and PCM to infants with RW, it is likely that as with older children,456 ATB are commonly prescribed to infants with viral respiratory conditions and asthma symptoms. This knowledge would be important because both medications have been related to the development of asthma later in childhood.78 However, there is controversy on this aspect910 regarding either ATB1112 or PCM.131415161718 An excessive use of ATB in older children with asthma and common viral respiratory infections (colds) occurs in developed countries,456 but there is no information on this aspect in infants with RW or colds during the first year of life. This study aimed to determine the prevalence and severity of RW and the characteristics of the use of asthma medications, ATB and PCM during the first year of life, and the frequency of and indications for the prescription of ATB and PCM at the community level in a large sample of infants (12,405) from 6 Latin American countries.
MATERIALS AND METHODS
This study is part of the International Study of Wheezing in Infants (EISL from the Spanish "Estudio Internacional de Sibilancias en Lactantes"): a general population-based study that surveys wheezing and related factors in random samples of infants during the first year of life. The data reported in this study were collected during the years 2011 and 2012. A detailed description of the methodology of EISL (questions, and definitions) has been published elsewhere.319 Briefly, EISL uses a standardized and validated questionnaire202122 on wheezing and other related variables occurring during the first year of life, to be responded by parents of infants at 12-15 months of age when attending their health care centers for immunization or a routine health control. The parents responded to questions about wheezing episodes (onset, frequency, and severity), protective/risk factors (pre- and postnatal tobacco exposure, breast feeding, maternal education, common viral respiratory infections, parental asthma, and household income per month, and others) and the use of asthma medications, such as IBD, ICS, OCS, and ALTR.
Definitions regarding wheezing questions and related risk/protective factors, such as tobacco smoking during pregnancy (yes/no), passive exposure to tobacco smoke, nursery school attendance, exclusive breast-feeding in the first 4 months, study level achieved by the mother (primary, secondary, university), and employment status of the mother and others have been described elsewhere.319
The questions about the frequency of and indications for the prescription of ATB were as follows. "During the first 12 months of life, how often on average did your child receive ATB due to his/her wheezing?": Never/1-3 times/4-6 times/7 or more times; "During the first 12 months of life, did your baby receive ATB due to any of the following conditions?" (yes/no): if yes, a) wheezing (obstructive bronchitis), b) common cold or flu, c) pharyngitis, d) pneumonia, e) otitis, f) diarrhea, g) urinary tract infection, h) skin infection, and i) others. The questions aboutthe prescription of PCM were as follows. "During the first 12 months of life, how often did your baby receive PCM?": never/1-3 times/4-6 times/7 or more times; "During the first 12 months of life, did your baby receive PCM due to any of the following conditions?" (yes/no): a) wheezing (obstructive bronchitis), b) common cold or flu, c) pharyngitis, d) pneumonia, e) otitis, and f) other non-respiratory conditions. Infants were considered to have suffered from upper respiratory tract infection (URTI or common cold) when parents positively answered the question, "Has your child had short episodes of cold with runny nose, sneezing, nasal obstruction, and mild cough, with or without mild fever?" They also registered the number of colds during the first year of life. The questions about severity markers (severe wheezing episodes, visits to the ED, and admissions for wheezing) were as follows. "Has the wheezing or the whistling in his/her chest been so severe (so intense) in the past 12 months that he/she was choking and having real difficulty breathing?" "Has the wheezing or whistling in his/her chest ever been so severe (so intense) in the last 12 months that you have had to take him/her to an ED (Hospital, Clinic etc.)?" and "Has your baby ever been hospitalized for wheezing?"
This study was carried out in 11 centers from 6 countries in South America: Argentina (Buenos Aires); Brazil (Cuiaba, Curitiba, São Carlos, São José do Rio Preto, São Paulo, Uruguaiana); Chile (Santiago); Colombia (Bucaramanga); Peru (Lima); and Uruguay (Montevideo). The samples of at least 735 infants were estimated to significantly detect a difference in the prevalence of recurrent wheeze (3 or more episodes) of 5% between 2 centers, 1 of them having approximately 20%, with a confidence level of 95% and a power of 85%. Centers obtained ethics approval to the requirements of the country and funded their own study. Parents or guardians who accepted to participate in the study filled in the questionnaire after reading and signing a full-informed written consent form.
Statistical analysis
The proportions of infants with RW, wheezing severity markers, prescribed medications (IBD, ICS, ATB, and others) between centers, were compared using the chi-square test with Yates's correction for continuity (2-tailed). We categorized infants who received ATB or PCM for respiratory causes (wheezing, colds, pharyngitis, otitis, and pneumonia) and non-respiratory causes (diarrhea, urinary tract infection, skin infection, and other causes); and by frequent use (≥4 times a year) of ATB or PCM. A P value of <0.05 was considered statistically significant. Data from different centers were analyzed by SPSS V.15 (SPSS Inc., Chicago, IL, USA). Data are expressed as mean (95% CI) except for age, which is reported as mean±SD. Univariate analysis, adjusted multivariate logistic regression, and multilevel model (using center as the second level) were used to estimate the strength of wheezing associations (OR and 95% CI).
RESULTS
Eleven centers provided 12,405 questionnaires with a mean response rate of 82.1% (95% CI 81.4-82.8), which were responded by mothers (87.5%), fathers (6.7%), and guardians (5%). The mean age of the whole sample of infants (50.6% males) was 13.4±1.5 months. Prevalence data regarding main variables (severity markers, medications, and others) for the whole sample and infants with RW, as reported by the centers, are shown in Tables 1, 2, 3, 4, 5. One of the participating centers (São Carlos) could not obtain a sufficient sample size and was not included for comparisons between centers and regression models; however, data from São Carlos appear in tables and figures as illustration. In this section, we mainly report findings in infants with RW; those in the whole sample are shown in Tables 1, 3, and 5, and in Figs. 1, 3, and 4.
Prevalence and severity of RW
There was a wide and significant variability in the prevalence, severity markers, and use of medications between the centers (Tables 2, 4, and 5). The mean prevalence of RW was 16.6% (95% CI 16.0-17.3), ranging from 7.5% in Bucaramanga to 26.4% in Montevideo (Table 1); 47.5% (95% CI 45.3-49.6) of the infants with RW started wheezing in the first 3 months of life. RW was strongly associated with wheezing during the first trimester of life (OR 9.31; 95% CI 8.1-10.7, P<0.001) and suffering from colds ≥6 times (OR 3.46; 95% CI 3.0-3.9, P<0.001, after adjusting for birth weight, gender, prenatal tobacco, parental asthma, and monthly household income. There was a significant association between RW and severe episodes of wheezing (OR 2.78; 95% CI 2.39-3.23), visits to ED for wheezing (OR 7.13; 95% CI 6.16-8.25), and admissions for wheezing (OR 1.53; 95% CI 1.30-1.79). The main risk factors for RW were tobacco smoking during pregnancy, parental asthma, household income <1,000 USD, male gender, and nursery school attendance, whereas breast-feeding for at least 3 months was significantly protective against RW (Table 6). The percentage of infants who were breast-fed for at least 3 months was 80.5%, ranging from 69.5% in São Paulo to 94% in Lima.
Common colds and RW
Infants with RW had a significantly higher mean number of colds (6.22; 95% CI 6.07-6.37) as compared to those without (3.57; 95% CI 3.52-3.63), P≤0.001, with 1-2 episodes (4.44%; 95% CI 4.33-4.55, P<0.0001) and without wheezing episodes (3.24%; 95% CI 3.18-3.30, P<0.001). Infants with ≥6 colds had almost 4 times more prevalence of RW (37.3%, 95% CI 35.49-39.10) than those with <6 colds (10.6%, 95% CI 9.97-11.52; P<0.001).
Antibiotic prescription
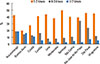
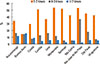
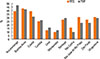
The frequency of the prescription of ATB by center in the whole sample of infants with RW is shown in Figs. 1 and 2. Respiratory causes (wheezing or obstructive bronchitis, colds, pharyngitis, otitis, and pneumonia), were the most frequent reasons for prescribing ATB ≥1 time (87.4%; 95% CI 86.7-88.1) and for ATB ≥4 times (37.5%; 95% CI 36.3-38.7). A 23.8% of those with ≥3 colds received ATB ≥4 times a year. The proportions of infants who received ATB ≥4 times a year for the studied indications in the whole sample and infants with RW are in Fig. 3; no significant difference was found in the variables between the whole sample and infants with RW. A 38.9% (95% CI 37.3-40.6) of infants without wheezing but treated with ATB for respiratory causes received ATB ≥4 times per year.
Paracetamol prescription
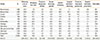
Ninety percent of infants in the whole sample received PCM ≥1 time a year; (1-3 times=31.2%; 4-6 times=30.0%; and ≥7 times=29.1%); in infants with RW: 1-3 times=31.6%; 4-6 times=30.7%; and ≥7 times=26.4%. The difference in PCM prescription between the whole sample and infants with RW were not significant for any of the categories. The proportions of infants who received PCM ≥7 times per year by center are depicted in Fig. 4.
There was a strong association between uses of ATB and PCM in either the whole sample (OR 3.57; 95% CI 3.07-4.15) and infants with RW (OR 2.16; 95% CI 1.62-2.90). Similarly, there was a significant association between use of PCM ≥4 times and use of ATB ≥4 times (OR 3.43; 95% CI 3.07-3.85); 79.5% of those who received ATB ≥4 times also received PCM ≥4 times.
Risk factors for RW
In multilevel analysis, a household monthly income over 1,000 USD was significantly associated with a lower prevalence of RW. In the whole sample, a 58.1% of subjects (95% CI 57.21-59.00) reported a household income per month ≤1,000 USD, ranging from 96.6% in Santiago (Chile) to 6.2% in Bucaramanga (Colombia), while a 34.0% of subjects (95% CI 33.2-34.9) of the whole sample reported a household monthly income of less than 500 USD. In infants with RW, a 68.0% of subjects (95% CI 65.9-70.0) reported a monthly household income ≤1,000 USD and 44.0% (95% CI 41.8-46.2) reported less than 500 USD. Thus, the families of infants with RW had a significantly lower household income per month than those of the whole sample for both household income categories (P<0.001).
Risk factors for pneumonia
The prevalence of pneumonia in infants with RW was 31.5% (95% CI 29.5-33.5), ranging from 12.6% in Lima to 43.2% in Buenos Aires. There was a strong association between RW and pneumonia (OR 4.06; 95% CI 3.59-4.58), and breast-feeding for at least 3 months was significantly protective against the disease (OR 0.65; 95% CI 0.59-0.74). The prevalence of pneumonia was significantly higher in infants with RW than in the whole sample (13.1%; 95% CI 12.6-13.8; P<0.001). Likewise, the frequency of admission for pneumonia was significantly higher in infants with RW (20.1%; 95% CI 7.4-8.4) than in the whole sample (7.9%; 95% CI 7.4-8.4; P<0.001).
Risk factors for colds
It was found that family history of asthma (1.44; 95% CI 1.27-1.64), tobacco exposure during pregnancy (1.68; 95% CI 1.45-1.95), male gender (1.17; 95% CI 1.07-1.28), and lower socioeconomic status (1.30; 95% CI 1.19-1.42) were significantly associated with ≥6 colds during the first year of life (P<0.001). URTI during the first 3 months was significantly associated with ≥2 siblings (1.27; 95% CI 1.16-1.40) and mold stains in the house (1.44 95% CI 1.32-1.58), whereas high maternal education (0.91; 95% CI 0.78-0.92) and higher household income (0.88; 95% CI 0.81-0.96) were significant protecting factors.
After adjustment for gender, prenatal tobacco smoking, parental asthma, and birth weight, cold during the first 3 months was significantly associated with wheezing ≥7 or more episodes (1.24; 95% CI 1.03-1.51), severe wheezing episodes (1.22; 1.10-1.36), ED visits (1.17; 1.07-1.29), and admissions (1.30; 1.14-1.49) for wheezing. There was no association between cold during the first 3 months of life and pneumonia or admission for pneumonia thereafter.
DISCUSSION
Recurrent Wheezing
Our data show that RW in infants is a highly prevalent condition, affecting 1.6 out of 10 infants during the first year of life in Latin America, with a large variability in prevalence and severity. An elevated proportion of infants with RW suffered from frequent and severe episodes, and required ED visits and admissions for wheezing, confirming previous findings in Latin America and Europe,319 with a high proportion of infants with RW reporting pneumonia and admission for pneumonia. The prevalence of severity markers in the first survey,3 which was performed 7 years ago, and the present study, remains similarly high (severe episode 61.2% vs 57.1%; visits to ED 73.3% vs 73.0%, and admissions for wheezing 28.4% vs 29.7%). This notoriously troublesome progression of RW, with exacerbations mainly associated with colds, would explain in part ICS, OCS, ALTR, ATB, and PCM plus several others of doubtful efficacy clinicians prescribe to the large proportion of these infants.123
Tobacco smoking during pregnancy, nursery school attendance, monthly household income less than 1,000 USD and parental history of asthma were associated with a higher prevalence of RW. However, breast-feeding was a protective factor, which is consistent with our previous findings in infants from Europe and Latin America19 showing that although risk/protective factors for RW were similar, the association strength varied between developed and developing countries.
Prescription of ATB
This study shows an excessive use of ATB not only in infants with RW but also in those from the whole sample, which was found to be mainly associated to common viral respiratory infections (colds). There is no information on the frequency of and main indications for the prescription of ATB and PCM from large international multicenter samples of infants with RW during the first year of life. This is an important issue because apart from all the concerns associated with the excessive use of ATB in children,23 that kind of medications and others, such as PCM, used in infancy might be a risk factor for asthma development later in childhood; however, this is still controversial.11121618 As shown in this study, it is likely that viral respiratory infections are important confounding factors for these associations,9101116 as they are frequently present in infants during the first year of life and strongly associated with the frequent use of ATB and PCM. These results are also observed in older children to whom ATB are prescribed in excess, especially in those with asthma and common viral respiratory infections.45623
To the best of our knowledge, our study shows for the first time that a 25% of infants receive ATB ≥4 times during the first year of life at the community level, which is mostly associated with diagnoses, such as colds, pharyngitis, and wheezing. The frequency of the prescription of ATB varied 3.2-fold in the whole sample and 4.7-fold in infants with RW among participating centers; the reason for this variability and overuse at the level is likely to be multifactorial. The medical practice and prescription behavior are important determinants of the excessive use of ATB, and physicians with high-volume primary care practice are more likely to prescribe ATB inappropriately.24 Recently, it has been reported that in well-resourced countries, ATB are prescribed to an important proportion of children with colds,2526 showing that this is a globally extended health problem independent of countries' development status and likely occurs at all ages.
Prescription of PCM
PCM is one of the most commonly used medications in infants due to its analgesic and antipyretic effects, and to its low price and current availability. In our study, 90% of all infants received PCM during the first year of life, and one-third used PCM ≥7 times per year, mostly for respiratory causes related to common colds. Data from birth cohorts show that PCM prescription to infants and toddlers ranges from 60% to 97%;1618 however, the prevalence of the combined use of ATBs and PCM is virtually unknown. In our study, the frequent use of PCM was strongly associated with the frequent use of ATB, demonstrating that in daily practice, these medications are often prescribed together; thus, an independent effect of each drug, as assessed later in life, would be much difficult to ascertain. For this reason, the relationship between ATB and PCM with the development of asthma later in childhood could be biased by confounding indications, mainly colds (or URTIs),91011 which would be indirectly supported by our finding that the excessive and combined use of ATB and PCM in infants during the first year of life is mostly associated with colds and related conditions.
Common colds
An interesting finding of this study is that prenatal conditions, such as family history of asthma, tobacco smoking during pregnancy, and lower socioeconomic status, were predisposing factors for a higher number of common viral respiratory infections during the first year of life (≥6 colds), which was clearly associated with frequent prescription of ATB and PCM. In addition, we found that high household income per month and high maternal education were associated with lower risk of colds during the first trimester of life, indicating that socioeconomic status would play an important role in the early occurrence of common respiratory viral infections, which seems to develop asthma in childhood.2728 According to our results, infants who have colds in the first trimester of life are more susceptible to colds, the prescription of ATB and PCM, and wheezing during their first year of life. This knowledge would offer room for prophylactic measures by increasing the awareness of avoiding respiratory virus exposure at least in the first 3 months, for instance, by prolonging maternity leave after childbirth to 6 months, as recently implemented in some countries of South America.
Other medications
Another finding of this study was the high prevalence of OCS and ALTR prescription in wheeze infants. Sixty-eight percent of infants with RW who reported use of ICSs also reported treatment with OCS, and 32.3% reported use of ALTR, which is rather surprising according to recent evidence showing that either medication would not be useful for the treatment of RW in infants.2930 In this study, ALTR were not provided to the primary health care institutions from participating countries without cost, meaning an additional economic burden on families that, in this study, were poor. It is possible that the high prevalence of severity markers could explain in part the more frequent use of OCS, ALTR, and ATB in this study. However, considering the high frequency of infants treated with ICS and BD, other explanations for this could include a poor aerosol administration technique, inappropriate spacers, lack of consistent availability of free ICS at health community centers, and low adherence to ICS and others, all of which will result in a predictably low or no therapeutic effect of inhaled medications.
Socioeconomic status
In this study, which assessed socioeconomic status at the individual level, a lower household income per month was associated with a higher prevalence of RW and severity markers, which is in keeping with previous studies.31323334 Similarly, our study supports previous findings of the large inequalities present within and between populations in Latin America.35
Limitations and strengths of this study
This study shares the limitations inherent to all cross-sectional studies, the foremost being that causality cannot be inferred. This study uses parental reports instead of physician's reports; however, the questionnaire was validated for infants attending the ED with acute wheezing episodes and against the pediatric thoracic physician's examination.202122 Recall bias is always an issue in transversal studies. In this study, however, parents were surveyed regarding several events in early childhood (12-15 months), in which recall would be easier than in late childhood.
The main strengths of this study are its large populationbased sample and high response rate; thus, it is likely that our results are representative of the Latin American region. This study also provides, for the first time in this region, information on the frequency of and indications for the prescription of ATB and PCM to infants with RW and the whole sample of infants at the community level, demonstrating large and significant differences among centers in the use of medications. Additionally, this study updates information on the prevalence and severity of RW in Latin America, showing that the number of severe episodes, visits to the ED, and admissions to hospital remains remarkably high and similar to those found in this region 7 years ago.3 The latter occurred despite the apparent progress in accessibility to effective inhaled asthma medications and medical attention at the primary care health level, and cast doubt on the efficiency of the health public strategies and programs for managing infants with RW at the community health level. Furthermore, this study confirms the strong relationship between RW and pneumonia in infants and reinforces previous findings from a birth-cohort of infants showing that RW is a strong predictor of pneumonia in infants from unprivileged populations during the first year of life.32
CONCLUSIONS
Our findings undoubtedly imply that RW in infants during the first year of life represents a high economic burden on parents and public health systems, utilization of emergency care centers, hospital admissions, and overuse of medications, particularly OCS and ATB. This study shows that there are urgent unsatisfied needs for a better approach and evidence-based management of infants with RW during the first year of life at the community level in this region. The implementation of adequate educational programs directed to parents and health personnel on prevention, diagnosis and treatment of infants with RW and related co-morbidity, is clearly a pending task. In the same context, a full provision of primary care centers with proper inhaled medications and holding chambers, together with teaching parents on correct inhalation techniques, are likely to have a direct and quick impact especially on decreasing the frequency of severe episodes, visits to the ED, and admissions to hospital in infants with RW.






 XML Download
XML Download