

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a common chronic disease, affecting at least 300 million people worldwide.1 It can develop at any age and is known to be associated with genetic, environmental, nutritional, and socioeconomic factors.2,3 Some known risk factors for adult-onset asthma are female sex, atopy, nasal allergy, family history, and high-risk occupations.4,5 The population-attributable risk for adult asthma due to occupational exposure is thought to be 10%-25%.5
Work-related asthma (WRA) refers to the exacerbation of preexisting or concurrent asthma in the workplace, as well as to new-onset asthma induced by sensitizers or irritants present in the workplace.6 It is the most common work-related respiratory disease in industrialized countries,7,8 and the second most common in Korea after pneumoconiosis.9
The first case of WRA in Korea was identified in a sea squirt processing factory in 1976.10 Many more cases and causal agents have been reported since, with isocyanates and reactive dyes being the most common agents.11,12,13 Before the Korea Work-Related Asthma Surveillance (KOWAS) program began in 2004, apart from a temporary WRA surveillance program conducted for 1 year in 1998, the only method to systematically estimate the number of WRA cases in Korea was by extracting data from workers' compensation schemes.14 This report provides findings from the first 6 years of the KOWAS program (2004-2009). We used KOWAS data to estimate the incidence of WRA by examining various demographic factors and to identify the distribution of causal agents over the study period.
MATERIALS AND METHODS
The establishment of KOWAS
KOWAS is a scheme designed to collect information on WRA cases from multiple reporting sources. It was set up in 2004 by the Occupational Safety and Health Research Institute of the Korea Occupational Safety and Health Agency (OSHRI-KOSHA). The Department of Occupational and Environmental Medicine of Hanyang University was selected as the KOWAS program's headquarters.
The scheme's reporting sources include the Korea Workers' Compensation and Welfare Service, occupational physicians, allergy and chest physicians, and regional work-related disease surveillance systems (i.e. regional surveillance systems that are housed in universities and funded by the KOSHA15). At the start of the program, there were 42 participating allergy and chest physicians, most of whom were affiliated with university hospitals. There were also 30 participating occupational health physicians or institutions, which included members of the Korean Association of Occupational and Environmental Clinics (KOEC). Regional surveillance systems located in the cities of Gumi, Incheon, Busan, and Changwon participated in the scheme in 2004, but from 2005 to 2007, only the systems in Incheon and Busan continued their participation. None of the regional surveillance systems participated after 2007.
Reporting individual cases
Individual patients were written up as case reports and sent to the KOWAS program headquarters. Each case report included the patient's sex, age, geographic location, occupation type, and exposure duration. In addition, the suspected causal agent, dates of asthma onset and diagnosis, whether it was new-onset versus exacerbation of preexisting asthma, and whether objective diagnostic tests had been conducted were also reported.
Definitions
There are 2 sub-types of WRA: (1) work-exacerbated asthma (WEA) and (2) new-onset occupational asthma (OA). New-onset OA is further divided into sensitizer-induced OA and irritant-induced OA, including reactive airways dysfunction syndrome (RADS).16 The definition of WRA proposed by the National Institute for Occupational Safety and Health (NIOSH) was used in our study.17 Thus, all WRA cases satisfied criteria (A) and (B) listed below. In addition, all cases satisfied 1 or more of the following criteria: (A) Diagnosis of asthma by a physician, (B) An association between the symptoms of asthma and work, (1) Workplace exposure to an agent or process previously associated with WRA, (2) Significant work-related changes in forced expiratory volume in 1 second (FEV1) or peak expiratory flow rate (PEFR), (3) Significant work-related changes in airways responsiveness measured by a nonspecific inhalation challenge test, (4) A positive response to an inhalation challenge test with a specific agent to which the individual is exposed at work.
The work-relatedness of WRA was classified as "definite" (satisfied the following elements of the case definition: A, B, 1, plus ≥2 of criteria 2-4), "probable" (A, B, 1, plus 1 of criteria 2-4), "possible" (A, B, did not satisfy 1 but satisfied ≥1 of criteria 2-4), and "suspicious" (A and B only) by the reporting source.13,18
Statistical analysis
The average annual incidence of WRA with regard to sex, age, region, industry, and occupation was based on the size of the working population as estimated in 2006 by the Korean Ministry of Employment and Labor,19,20 and 95% confidence intervals (CIs) were based on Poisson distribution. Industries and occupations were classified using the eighth Korean Standard Industrial Classification (KSIC),21 and the fifth Korean Standard Classification of Occupations (KSCO),22 respectively.
Capture-recapture analysis was used to obtain a nearly unbiased estimator (NUE) of the total number of WRA cases.23 To do this, the 4 reporting sources were stratified into 2 categories as follows: (1) the workers' compensation scheme (i.e. the Korea Workers' Compensation and Welfare Service), and (2) the other 3 reporting sources (i.e. physicians' reports). Capture-recapture analysis was performed on specific industries and occupations when the number of overlapping reports was ≥7. Overlapping reports, i.e. duplicate cases, were defined as individuals who had identical names, dates of birth, resident registration numbers, and employers found in both reporting categories.
The distribution of WRA cases based on sex, causal agent, WRA subtype, and reporting source were described over the study period, and annual trends were tested using the Cochran-Armitage test for trend. SAS 9.1 (SAS Institute Inc., Cary, NC, USA) was used to perform all statistical analyses.
RESULTS
From 2004 to 2009, a total of 239 cases of WRA were reported to the KOWAS, but 3 cases were excluded from analyses because the workplaces associated with these cases were not included in the working population in this study. A total of 236 cases were reported by 4 reporting sources: 52 (22.0%) by occupational physicians, 124 (52.5%) by allergy and chest physicians, 102 (43.2%) by workers' compensation schemes, and 57 (24.2%) by regional surveillance systems. Although some cases were reported multiple times by different sources and in different years, each individual was counted only once. A total of 164 (69.5%) cases were men, and 72 (30.5%) were women. The overall mean age was 44.1 (±11.0) years, and the mean age for men (43.4±11.5 years) and women (45.6±9.5 years) were not significantly different. The highest frequencies of WRA were found among the 40-49 and 50-59-year-olds (31.4% and 26.3%, respectively). WRA was determined as "definite" in 58.1% of all cases (n=137), "probable" in 36.4% (n=86), "possible" in 4.2% (n=10), and "suspicious" in 1.3% (n=3). According to the WRA sub-types, new-onset asthma was most frequent (92.4%, n=218) with sensitizer-induced OA responsible for the vast majority at 86.9% of the total number of cases (n=205), followed by irritant-induced OA at 5.5% (n=13). WEA was responsible for 3.8% (n=9) of WRA cases. KOWAS had information regarding the specific objective tests that met the work-relatedness criteria for only 81 cases. Among these cases, 13 (16.0%) had work-related serial changes of PEFR or FEV1, 3 (3.7%) had work-related serial changes of nonspecific challenge tests, and 72 (88.9%) had a positive response to specific challenge tests. Objective tests were performed on the other 152 cases which were classified as nonsuspicious, but details of this testing were not provided by the reporting source (Table 1).
The number of allergy and chest clinics that reported at least 1 case was 16, and 8 of these clinics accounted for the vast majority of reports (118 [93.7%] of 126 cases). The number of occupational clinics that reported at least 1 case was 15, and 8 occupational clinics reported 41 of these cases (78.8% of 52) (Table 2).
The average annual incidence during the 6-year period was 3.31 per million workers. When stratified by sex, the average annual incidences were 3.78/million male workers and 2.58/million female workers. The incidence was highest in the 50-59 year age group at 7.74/million workers. By region, the incidence was highest in Gyeonggi/Incheon at 8.50/million workers, and lowest in Seoul and Gangwon at 0.92/million workers. The number of cases estimated by the capture-recapture method was 447 (95% CI: 353-541), and the corresponding average annual incidence of WRA was 6.28 (95% CI: 4.96-7.60) cases/million workers, approximately double the crude incidence (Table 3). By industry, the incidence was highest in the furniture and other instrument manufacturing industries at 67.62/million workers. By occupation, the incidence rate was highest in the craft and related trades at 17.75/million workers (Table 4).
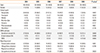
Among the suspected causative agents of OA or triggering factors of WEA, isocyanates were the most frequent at 46.6%, followed by flour/grain (8.5%), metals (5.9%), reactive dyes (5.1%), and solvents (4.2%). The distribution of causal agents was not significantly different between men and women for the 7 most frequently reported agents (Table 5).
During the study period, isocyanate-related asthma followed a decreasing trend (P=0.002). In terms of asthma sub-types, the frequency of sensitizer-induced OA also followed a decreasing trend (P=0.008), while that of WEA appeared to be increasing (P=0.006), but was based on data from a very small number of cases. While the number of cases reported by occupational physicians and regional surveillance systems steadily decreased, those reported by allergy and chest physicians remained relatively steady (Table 6).
DISCUSSION
The average WRA incidence of 3.31/million reported in our study was lower than those reported by surveillance systems in other countries, which ranged from 5-174/million workers.7,8,24,25,26,27,28,29 This difference suggests a lower prevalence of asthma in Korea than in other industrialized countries,1,3,30 and a lower proportion of WRA among adult asthmatics.12 However, most of the available estimates from other industrialized countries are based on data from the 1990s. Since WRA surveillance in Korea began later than in other countries, direct comparison of rates should be performed with caution. In some countries (e.g. the UK and France), the number of WRA cases decreased during the 1990-2000s; possible reasons for the decrease being due to reporting fatigue, changes in industrial structure, and substitution of hazardous materials from the workplace.31,32 Other possible reasons for the underestimation include the workers' unwillingness to report illness because of concerns about job loss,24 lack of workers' compensation coverage among some workers who may be at high risk of developing WRA (e.g. self-employed and temporary workers are not covered, and may carry a high risk of developing WRA),33 physicians' failure to ask about work-relatedness, and physicians' unwillingness to report to surveillance schemes even when work-relatedness is suspected.34 Furthermore, the observed differences in WRA rates between countries arise not only from differences in reporting but also from differences in the distribution of industries and occupations.26
The WRA incidence estimated by capture-recapture analysis was 6.28/million. Capture-recapture models allow the estimation of the true number of cases and the assessment of the completeness of the surveillance data. This methodology has been used in a variety of public health areas.23,35 The NIOSH in the United States used capture-recapture methods and estimated that the "true" number of WRA cases was approximately 6- to 7-fold higher than the number reported using surveillance data.26 In our study, the estimated "true" number of cases was approximately double the reported number.
Approximately 80.1% (n=189) of all reported WRA cases were found in the manufacturing sector, including furniture manufacturing, chemical manufacturing, vehicle manufacturing, and food and beverage manufacturing. The rates in these manufacturing industries were higher than those in almost all other industries. The WRA incidence was highest in the furniture manufacturing industry (67.62/million), likely due to the high rate of isocyanate use, which is the leading cause in the development of WRA.
Workers aged ≥50 years of age had higher rates of WRA compared to younger workers. This pattern has also been observed in previous studies8,24,29,36 and could be due to a combination of reasons. For example, older workers are more likely to have a longer duration of exposure to hazardous substances, and they may have a greater susceptibility to developing asthma. In addition, younger workers may find it easier to change jobs to avoid exposures, and older workers may delay reporting their asthma symptoms.24,26,37
The rates of WRA in Korea differ substantially across regions within the country, ranging from 0.92-8.50/million workers. Regional differences were also found in France.24 These findings may be due to regional differences in reporting, and in industrial composition.
As in other countries,7,8,25,27,38,39,40 the most common cause of WRA in Korea was exposure to isocyanates, but the proportion of WRA cases attributed to isocyanates in Korea (46.6%) was much higher than that in other countries (13.6%-23.1%). Possible reasons were that claims for compensation are generally approved whenever isocyanate is present at the workplace regardless of the actual WRA cause and reporting physicians are familiar with the processes leading to isocyanate exposure. The second most common cause of WRA in our study was grain dust, which was possibly due to a large number of WRA cases identified during an epidemiological investigation at a bakery.41 Approximately 5%-10% of bakery workers are thought to have WRA.42 Moreover, the actual number of cases of WRA caused by grain dust may have been much higher, considering that agriculture workers in small companies (<5 workers) and the self-employed are not eligible for workers' compensation in Korea.33 Some new and emerging causes of WRA were also identified by the KOWAS. Examples include azodicarbonamide43 (used as a plastic foaming agent) and cyanoacrylate44 (used as an instant glue), both of which had not previously been observed to cause WRA in Korea.
The pattern of isocyanate exposure being the dominant cause of WRA in Korea tended to diminish over time. Factors responsible for this decrease may include recent increased awareness and recognition of other causes of WRA, and a true reduction in the incidence of isocyanate-induced WRA, a sensitizer-induced OA. Reductions in the incidence of isocyanate-induced WRA were also observed in France.32 Few cases of irritant-induced OA were identified by the KOWAS. This may be because an understanding of the role of respiratory irritants in the etiology of OA is too recent a phenomenon to be captured by the KOWAS data.45
This analysis has several limitations. Although isocyanates were the most common cause of WRA, in some instances of isocyanate-caused WRA, an agent other than isocyanates may have caused the asthma. Second, the reported rates are likely to be underestimates. Many cases of WRA are never ascertained or reported. This is because many workers are not covered by workers' compensation, or because many physicians fail either to diagnose WRA or to report WRA to the KOWAS. Third, detailed information on the specific objective diagnostic tests that were used to assess the work-relatedness criteria were often not available to the KOWAS. In these instances, the KOWAS relied on the work-relatedness assessment made by the reporting source. Fourth, the specific causal agent of WRA could not be identified because objective tests on the specific agents were either not conducted or the test results were not available to the KOWAS. A similar lack of specificity is present in WRA reports from other countries.7,8,24,25,27,28,29
The effectiveness of the KOWAS could be improved if it was supported by active and ongoing work-related disease surveillance schemes and occasional company-wide health evaluations. The latter, prompted by findings made during the course of our surveillance study, helped to identify many additional WRA cases in a bakery. After a sentinel case of baker's asthma from an industrial bakery was reported to the KOWAS in October 2005, a thorough epidemiological investigation was performed by the KOSHA in 2006-2007.41 As a result, 12 additional workers were diagnosed with baker's asthma and reported to the KOWAS. In other cases where the causal agents could not be identified, or their work-relatedness could not be established, the KOWAS findings prompted additional epidemiological investigations.46,47
Before the KOWAS was established, the only method to estimate rates of WRA in Korea was by analyzing data from workers' compensation reports. However, many WRA patients do not apply for workers' compensation. The KOWAS scheme was designed to overcome this limitation. From 1997-2003, the number of cases of WRA from workers compensation ranged from 4-29. During the study period (2004-2009), the total number of WRA cases identified by the KOWAS was more than double the number of cases identified by the worker's compensation scheme alone. As a public health surveillance system, the objective of the KOWAS is not only to estimate the magnitude of WRA, but to also analyze WRA trends in Korea, to detect emerging causes of WRA, and to guide policy changes and workplace interventions in order to prevent WRA and promote worker health.
In conclusion, the incidence of WRA estimated from surveillance data was lower in Korea than in other countries, and the incidence varied according to industry, occupation, sex, and region. Data provided jointly by workers' compensation schemes and physician reports are useful for determining the rates and causes of WRA in Korea.





 XML Download
XML Download