

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The incidence of asthma, which affects subjects of all ages, is increasing worldwide, and it is a leading socioeconomic burden in many countries. The prevalence of asthma in the elderly ranges from 6% to 17% and is similar to or higher than that in younger adults.12 With aging of the population, the importance of proper management of older patients with asthma has become a global concern. The clinical features of elderly asthma patients are different from those of non-elderly patients, and they suffer from more comorbidities1345 and show more frequent adverse reactions to antiasthmatic drugs, both of which affect asthma control.1 Little is known about the control status of asthma and related factors in the older population, because most clinical trials of antiasthmatic agents have been performed in pediatric or younger adult patients.
Asthma is a chronic inflammatory airway disease characterized by hyperresponsiveness and variable airflow limitation.6 Maintaining controllers, such as inhaled corticosteroids (ICS) and leukotriene receptor antagonists (LTRA), to reduce inflammation is important for the management of asthma. Various effects of ICS and LTRA have been reported, such as anti-inflammatory effects, improved pulmonary function, preventing exacerbations, and reduction of symptoms and bronchial hyperresponsiveness.7 The guidelines for asthma treatment indicate that LTRA can be used instead of ICS for patients with mild asthma.7 When inhaled steroids cannot control asthma completely, the addition of LTRA helps to relieve symptoms.7 Although the efficacy of montelukast in addition to ICS was reported to be inferior to the addition of a long-acting beta-agonist (LABA) in adults or children,8 there have been few reports regarding the effects on asthma in the elderly. Adverse reactions to ICS in older patients may increase systemic and musculoskeletal complications, such as diabetes,9 osteoporosis,10 and cataracts,11 and it is therefore necessary to minimize daily ICS dose in older patients. Moreover, older patients with asthma show greater compliance to oral medications and lower levels of physical activity compared to younger patients.12 Therefore, it is necessary to determine whether combination therapy with low-dose ICS and LTRA is safe and effective in older patients in whom asthma is inadequately controlled by low-dose ICS. In addition, the treatment goal is not only to improve pulmonary function or airway inflammation but also overall asthma control and physical performance.
This study was conducted to compare the efficacy of the addition of montelukast to low-dose budesonide with that of medium-dose budesonide on the Global Initiative for Asthma guidelines (GINA)-defined asthma control and asthma control test (ACT), asthma-specific quality of life (AQoL), and sputum inflammatory cells in older patients with asthma. In addition, to evaluate the correlations of physical function and depression on asthma control in older patients, we measured geriatric physical functioning scales (PFS) and depression scores at baseline and at the end of the study.
MATERIALS AND METHODS
Subjects
The subjects ranged in age from 60 to 75 years and had been diagnosed with asthma more than 6 months before enrollment in the study based on clinical symptoms (such as cough, wheezing, breathlessness, chest tightness and dyspnea), airway reversibility (defined by an increase of forced expiratory volume in one second (FEV1) >12% and 200 mL from pre-bronchodilator use), and airway hyperresponsiveness (PC20 <16 mg/mL of methacholine). Their current treatment was ICS (budesonide 400 µg/day or equivalent) or a combination of low-dose inhaled budesonide and LABA (Seretide® 250 µg/day or equivalent) for over 1 month before participating in this study. To be eligible for this study, the patients were required to have normal results on complete blood count, routine chemistry, urinalysis, and electrocardiogram at the screening. Institutional review board approval was obtained for inclusion of subjects who gave sufficient attention to the purpose and content of the study, agreed to participate voluntarily, and provided signed written consent.
Patients were excluded if they (1) had other acute diseases within 28 days before administration of trial medications, (2) had history of hypersensitivity to montelukast or budesonide, (3) were either current or former smokers with a smoking history of more than 10 pack years, and (4) required administration of any medications that may affect asthma control, such as systemic steroids and immunomodulatory drugs (cyclosporine, omalizumab, etc.) due to diseases other than asthma.
Study design
This was an open-label, multicenter, randomized, prospective trial involving male and female outpatients over 60 years old. Eligible subjects were recruited between August 2011 and February 2012 from 5 university hospitals in Korea. Inhaled budesonide at 400 µg/day was given during the 4-week run-in period, following which 140 subjects were randomized to take either 800 µg of inhaled budesonide (800BUD) or 400 µg of budesonide plus 10 mg of montelukast (MON-400BUD) per day for the 12-week treatment period. At the visit for the randomization, subjects not meeting the criteria of GINA-defined 'well controlled asthma'7 (day symptoms of twice or less in a week, no limit of activities, no night symptom and sleep disturbance, use of reliever of twice or less in a week, normal FEV1 (over 80% of predicted value), and no exacerbation) were finally enrolled. Geriatric assessments, including PFS,13 geriatric depression scale,14 and 6-min walk test,15 were conducted after the run-in period and on completion of the study. Asthma patients' diaries to check administration of investigational drugs, daytime symptoms, nighttime symptoms, and use of rescue medicine were collected. Pulmonary function test (PFT), sputum samples, ACT,16 and AQoL17 were obtained at baseline and every 4 weeks during the treatment period.
The primary endpoint was the proportion of subjects reaching "well-controlled asthma" after the 12-week treatment period based on the GINA guidelines.7 The well-controlled asthma was defined by both asthma symptom control (daytime symptoms and reliever use were less than twice/week and none of night awakening and activity limitation) in the past 4 weeks and normal lung function (FEV1 ≥80%) at the visit. We also determined partly controlled and uncontrolled asthma on the basis of the GINA defined asthma control levels.7 If any measures of the well-controlled asthma criteria are not sufficient, those cases are classified as the partly controlled status. In cases that more than 3 measures were unmet, those are classified as the uncontrolled asthma.
When the study was completed, an independent physician working at the data center assessed the control status based on the patients' diaries and the results of PFT, and then compared their status assessment with investigators' assessment of the control status. For the subjects whose asthma control status was differently assessed by investigators, data center asked the data monitoring team to review source documents of the subjects to make clear the discrepancies with the investigators. Secondary endpoints included changes in sputum eosinophil and neutrophil percentages from baseline, frequency of local adverse events, time to the first well-controlled week, asthma exacerbation including worsening of asthma symptoms requiring oral corticosteroids (prednisolone 10 mg equivalent dose per day for at least 3 consecutitive days) or unscheduled visits, emergency department (ED) visits, or hospitalization due to asthma symptoms. Local side-effects, including oral thrush, sore throat, voice change, laryngeal discomfort, and paroxysmal cough immediately after inhalation, observed in the previous month, were collected by patients' diary and questionnaire and clinical examination at each visit. Adverse events were assessed for severity, duration, and study drug causality. Randomization was performed according to a balanced block design with a centrally generated randomization code and stratified by each center. This trial is registered at ClinicalTrials.gov, number NCT 01147510.
Statistical analysis
A sample size of 140 patients was calculated by the non-inferiority test for primary endpoint with 80% power, 0.025 alpha (one-sided), and 10% drop-out rate (PASS 2005, NCSS, Kaysville, UT). The difference in the rate of well-controlled asthma between the MON-400BUD and 800BUD groups was estimated as 7.9%, and non-inferiority margin was considered 17.2%.181920 For proving therapeutic non-inferiority of MON-400BUD vs 800BUD treatment, the one-sided test hypothesis was used. We applied the per-protocol (PP) principle to evaluate non-inferiority for the primary endpoint to reduce possible statistical bias caused by missing data imputation. Non-inferiority was concluded if the lower limit of 97.5% CI of the difference in proportion of patients with well-controlled asthma between the MON-400BUD and 800BUD groups was greater than the non-inferiority margin (-17.2%). The noninferioity margin was determined by estimating the mean rate differences of the proportion of patients who achieved well-controlled asthma between the ICS vs ICS plus LABA (52% vs 71%, 52% vs 69%, and 33% vs 51%) groups18 and the difference (14.6%) from placebo in the percentage of asthma control days for montelukast group.19 The supportive test was based on the intention-to-treat analysis set with the last observation carried forward (LOCF) approach. The proportion test using the R program (version 3.0.2, R development core team, http://www.r-project.org) was performed for the non-inferiority test.
The t test was used to analyze continuous variables and changes in inflammatory markers, such as sputum eosinophils (%) and neutrophils (%), PFT, and PFS over the 12-week treatment period. McNemar's test was applied to compare the proportion of patients with uncontrolled asthma at each time period. The categorical variables and frequencies of local adverse events, including oral thrush, sore throat, voice change, laryngeal discomfort, and paroxysmal cough immediately after inhalation on every visit, were analyzed by Fisher's exact test (SPSS 20, Chicago, IL). Time to the first well-controlled week during the 12-week treatment period was analyzed by the Kaplan-Meier test.
To evaluate the difference in proportions of subjects with ACT scores at the end of treatment ≥20 between the 2 treatment groups, the proportion test using by R 3.0.2 was performed.21 The correlations between changes in ACT and other clinical assessments, including FEV1, PFS and GDS, were analyzed by Spearman's Rho test. Pearson's chi-square test was used for comparing gender among the patients with 3 levels of asthma control at the end of the study. ANOVA was used for comparing baseline BMI and changes from baseline in clinical parameters, such as lung function, ACT, AQoL, 6-min walk test, PFS, and GDS, among the patients with three levels of asthma control at the end of the study. Multivariate ordinal regression analysis with reference to the uncontrolled group was applied to determine predictors of asthma control status over the 12 weeks of treatment. In all analyses, P<0.05 was taken to indicate statistical significance.
RESULTS
Patients
A total of 157 patients were screened, and 140 were randomized into treatment groups (70 into the MON-400BUD group and 70 into the 800BUD group). Of these, 12 patients were withdrawn after randomization (5 in the MON-400BUD group and 7 in the 800BUD group) because of loss to follow-up (n=2), protocol deviation (n=1), withdrawal of consent (n=5), non-compliance (n=3), or inability to manage asthma exacerbation at home (n=1); 128 (91.4%) completed the 12-week study. The first patient entered the study on August 7, 2011 and the last patient completed the study on July 28, 2012. Patient enrollment is shown in Fig. 1.
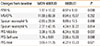
There were no significant differences in baseline characteristics or geriatric assessment between the 2 groups, as shown in Table 1. The mean numbers of days on which the subjects missed taking the trial medications during the 12-week of study were 0.39±1.76 days in the MON-400BUD group and 0.31±1.33 days in the 800BUD group (P=0.793).
Efficacy
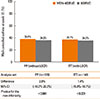
In the PP population, well-controlled asthma was achieved at the end of the treatment period in 24 (36.9%) and 22 (34.9%) subjects in the MON-400BUD (n=65) and 800BUD (n=63) groups, respectively. The patients of the MON-400BUD obtained non-inferiority in proportion of well-controlled asthma status compared to the 800BUD group (a treatment difference of 2.0% and 95% CI of -16.2% to 20.2%). The lower limit of the 95% CI was above -17.2%, which was the predefined margin for the non-inferiority (P<0.001). The results for the ITT population (25/70 patients in the MON-400BUD group and 24/70 patients in the 800BUD group achieved well-controlled asthma) were the same as those observed in the PP population and confirmed the therapeutic non-inferiority between both treatment groups (Fig. 2).
After the 4-week run-in with low-dose budesonide (400 µg/day) treatment, 1.4% and 2.9% of subjects in the 800BUD and MON-400BUD groups were in the well-controlled state, respectively (Fig. 3). There were no significant differences in the rates of well-controlled asthma between the MON-400BUD and 800BUD groups in weeks 4 (35.8% vs 35.1%, respectively) and 8 (27.7% vs 26.6%, respectively). Both treatment groups reached a plateau in asthma control status after the first 4 weeks of treatment compared with baseline. However, there continued to be fewer subjects with uncontrolled asthma between weeks 4 and 8 (24.5% to 13.8% in the MON-400BUD group and 35.1% to 23.4% in the 800BUD group, P<0.001, respectively), and 8 and 12 (13.8% to 6.2% in the MON-400BUD group and 23.4% to 15.9% in the 800BUD group, P<0.001, respectively) in the 2 groups. The Kaplan-Meier plot of time to the first well-controlled asthma indicated no significant difference between the 2 groups (P=0.499, data not shown).
Baseline mean ACT scores were not different between the 2 groups. During the treatment period, no significant differences were observed in mean ACT scores of the 2 groups (19.8±4.1 vs 19.5±4.2 in week 4, 19.2±4.4 vs 18.8±4.7 in week 8, and 19.4±4.7 vs 18.9±4.6 in week 12, P=0.689, 0.660, and 0.525, respectively, Fig. 4A). Analysis of variance for repeated measurements of ACT scores showed no significant interaction between treatment groups and time (P=0.904).
However, the proportion of subjects with ACT scores at the end of treatment <20 was significantly higher in the 800BUD group than in the MON-400BUD group (56.3% vs 35.4%, respectively, P=0.022, Fig. 4B). In addition, of patients with uncontrolled asthma at baseline on the basis of ACT score (<20), 46.9% (15/32) in MON-400BUD and 15.2% (5/33) in 800BUD had a score ≥20 after the 12-week treatment period (P=0.012).
The objective measures, including FEV1%, MMEF%, and sputum eosinophil and neutrophil percentages, were not statistically different between the 2 treatment groups (Table 2). There was no significant correlation among changes in ACT and changes in total scores of PFS (correlation coefficient 0.132, P=0.136)/GDS (-0.073, P=0.418)/predicted FEV1% (0.150, P=0.093) before and after treatment. However, the mean change in total PFS showed a significant increase in the MON-400BUD group compared with the 800BUD group (0.95 vs -4.22, respectively, P=0.021, Table 2). PFS consists of 2 distinct categories, mobility and self-care. With respect to changes in each category of the PFS after treatment, a significant difference was observed in mobility scores (0.38 vs -6.34, P=0.037) between the MON-400BUD and 800BUD groups, while no significant difference was noted in self-care scores (1.74 vs -2.06, P= 0.088, Table 2). However, there was no significant correlation between changes in 6-min walk distance and ACT during the study period.
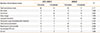
Eleven potential determinants of asthma control, including treatment group, gender, BMI, and changes in FEV1%, ACT, AQoL, 6-min walk distance, PFS (total, mobility, and self-care), and GDS, from baseline in older patients were evaluated with reference to the uncontrolled asthma baseline seen after the run-in period. Univariate analysis indicated that changes in ACT and PFS during the 12-week treatment were significantly different among patients with well-controlled, partly controlled, and uncontrolled asthma (Table 3). Subsequent multivariate ordinal regression analysis revealed that patients achieving well-controlled and partly controlled asthma had significantly lower BMI than uncontrolled asthmatics (24.7 in well-controlled, and 24.6 in partly controlled vs 26.1 in uncontrolled, P=0.018) and higher improvement in FEV1% (2.3 vs 0.4 vs -4.2, P=0.015), ACT (2.0 vs 0.2 vs -2.8, P=0.013), 6-min walk distance (14.9 vs 5.5 vs -10.5, P=0.032), PFS-mobility (1.0 vs -3.4 vs -17.9, P=0.018) and PFS-self-care (1.7 vs 0.9 vs -11.9, P=0.033) during the study period (Table 3).
Exacerbations of asthma occurred in 13 patients (a total of 28 events) in the 800BUD group and in 7 patients (a total of 14 events) in the MON-400BUD group (P=0.016 for the numbers of total exacerbation and P=0.148 for the numbers of patients who had ever any asthma exacerbations during the 12-week of treatment, Table 4). In particular, asthma exacerbations requiring corticosteroids were significantly more frequent in the 800BUD group compared to the MON-400BUD (20 courses in 12 patients vs 9 courses in 7 patients, respectively, P=0.036). Regarding unscheduled OPD and ED visits during the 12-week treatment, 5 patients had 6 unscheduled visits and 2 patients visited the ED once each in the 800BUD group, while in the MON-400BUD group, 3 and 2 patients visited the OPD and the ED once each, respectively.
Safety
There was no difference in adherence to trial medication between the MON-400BUD and 800BUD groups during the study period (95.4% vs 96.3%, respectively, P>0.05). Total experiences of local adverse events, including oral thrush, voice change, laryngeal discomfort, and paroxysmal cough immediately after inhalation, were not different between the 2 treatment groups (P=0.171, Table 4). However, cases of sore throat associated with inhalers were significantly more frequent in the 800BUD group than in the MON-400BUD (22 numbers in 14 patients vs 11 in 10 patients, respectively, P=0.045 for the numbers of sore throat events and P=0.367 for the episodes of patients having sore throat). Of 28 subjects who had experienced at least one local adverse event during the 12-week of treatment, 9 (32.1%) had asthma exacerbation, whereas 5 (5.9%) of 85 subjects without local adverse event had suffered from exacerbation (P=0.001). In particular, changes in GDS from baseline were significantly increased in patients having sore throat as compared to those without sore throat (0.85±1.50 vs -0.12±1.61, P=0.015). However, changes in FEV1 and ACT from baseline were not different according to the presence of local adverse events in the present study. There were no other clinically significant drug-related adverse events, serious adverse events, or discontinuation of treatment because of adverse events. The most common adverse events were sore throat and laryngeal discomfort associated with using inhalers and taking oral corticosteroid due to exacerbation of asthma.
DISCUSSION
This is the first study to investigate the effects of montelukast as an additional therapy to low-dose ICS compared to medium-dose ICS alone in older patients with mild asthma. Several trials demonstrated that combination therapy of ICS with montelukast was more effective than ICS alone in reducing exacerbations of asthma and use of short-acting beta-agonists.202223 However, most of these studies were performed in children or younger adults. In addition, the greater effectiveness of montelukast add-on therapy was noted in patients with lower asthma severity and less treatment levels.22 The results of the present study indicated that montelukast added to inhaled budesonide at 400 µg/day was not inferior to monotherapy with inhaled budesonide at 800 µg/day in GINA-defined asthma control over a 12-week treatment period. These observations are compatible with a recent systematic review23 indicating that adding montelukast to ICS improves control of mild to moderate asthma compared with ICS alone. In terms of exposure to systemic steroids, however, more frequent asthma exacerbations and oral corticosteroid use were noted in subjects in the 800BUD group compared to those in the MON-400BUD group. Therefore, the present study demonstrated that the addition of montelukast to ICS has a similar effect on asthma control as increased dose of ICS, and as well can reduce short-term corticosteroid burst in older patients with mild asthma.
Among various clinical parameters associated with lung function, airway inflammation, and physical function, changes in ACT and PFS, FEV1% predicted, and 6-min walk distance, as well as initial BMI, are significantly related to GINA-defined asthma control status. Therefore, we can judge the treatment effect on asthma control of older asthmatics based on changes in 2 patient-oriented questionnaires, such as ACT and PFS, before and after treatment. In addition, improvement in objective physical measures, including FEV1% and 6-min walk distance, compared with the respective baseline can facilitate prediction of asthma control among older patients. Consistent with previous studies,2425 increased BMI was significantly associated with uncontrolled asthma regardless of treatment group or gender. In addition, changes in FEV1% and 6-min walk distance, which were not significantly associated with asthma control in univariate analyses, became strongly related to poorer asthma control in the multivariate ordinal regression model with various covariates, including BMI. Obese patients with asthma may be less responsive to corticosteroids and may show differences in the levels of inflammation.25
A previous multinational survey indicated that an ACT score <20 predicted poorly controlled asthma in 94% of cases.26 Here, we compared the numbers of patients with poorly controlled asthma (ACT<20) at the initial visit who showed improvement to ACT ≥20 at the end of the 12-week treatment between the MON-400BUD and 800BUD groups. These results indicated that a significantly higher proportion of patients in the MON-400BUD group achieved ACT ≥20 than in the 800BUD group. Furthermore, the overall proportion of patients achieving ACT ≥20 over the 12-week treatment period was significantly higher in the MON-400BUD group compared with the 800BUD group. Of patients with poorly controlled asthma after the 4-week run-in treatment with 400 µg of inhaled budesonide, 84.8% in the 800-BUD group retained an ACT <20 after doubling the ICS dose to 800 µg for 12 weeks, while 46.9% of those in the MON-400BUD group moved to the ACT ≥20 after adding montelukast. These results suggest that most of older patients with mild asthma, but in the poorly controlled state even with low-dose ICS treatment, may be less responsive to increasing ICS dose. As previously demonstrated,27 up to 35% of patients with asthma fail to respond to ICS treatment. A systematic review reported that increasing the dose of ICS provides relatively little further benefit in asthma control but increases the risk of side effects.28 Although all of the subjects in the present study had been treated with ICS alone or combined LABA for at least 6 months, 14 patients in the MON-400BUD group and 17 of those in the 800BUD group suffered from local adverse events associated with ICS. Furthermore, the frequency of sore throat events was significantly higher in the 800BUD group than in the MON-400NUD group. As the frequent occurrence of ICS-associated adverse events may hinder maintenance of inhaler use, more frequent asthma exacerbations and oral corticosteroid use may occur in the 800BUD group. Despite the lack of differences in adherence to medication regimens between the 2 groups, however, the ICS inhalation technique is commonly incorrect in older patients due to impaired cognitive function, weak vision, and a lack of familiarity with the devices.1 This lack of proper ICS technique may have affected the efficacy of ICS treatment in both groups, while the oral bioavailability of montelukast is similar to that in young adults.29
In the present study, we used PFS, a unique geriatric assessment for physical functioning, together with 6-min walk test, which is a well-known measure of functional capacity.15 Changes in PFS from baseline were significantly related to GINA-defined asthma control, while no significant responses were observed in 6-min walk distance after the 12-week treatment period. Although the 6-min walk test has been widely used to assess the responses to therapeutic interventions for pulmonary and cardiovascular diseases, it may not be optimal for assessing less-impaired subjects, such as older patients with mild asthma.30 In contrast, with 2 distinct categories, mobility and self-care, PFS seems to be a more comprehensive measure as they are composed of 10 questions in total and convenient to use. PFS, and particularly scores of mobility, decreased significantly from the baseline in the 800BUD group, whereas the scores in the MON-400BUD group were improved over the 12-week treatment period. It might indicate that the more frequent asthma exacerbations requiring corticosteroids in the 800BUD group may have restricted patients' daily activities more severely compared to the MON-400BUD group.
This study has several limitations, including the lack of blinding and placebo control. Although we checked patients' diaries and PFTs by an independent physician and then adjusted investigators' assessment on the asthma control, the potential for observer bias could not be completely excluded in our study. Because both ACT and GINA-defined asthma control are dependent on the patients' recall of asthma symptoms, these may not be entirely accurate particularly in older patients. Therefore, recall bias on the participating subjects may have influenced the results of the present study.
The goal of asthma management is to achieve control with minimal or no use of systemic corticosteroids. In older patients, the risk of systemic adverse effects of steroids is higher than in younger patients due to their comorbidities, such as osteoporosis, diabetes mellitus, hypertension, and cataracts.3132 The results of the present study indicated that the end-point control was similar between groups based on applying GINA guidelines but significantly better in the MON-400BUD group based on ACT scores.
In conclusion, the addition of montelukast to low-dose ICS for 12 weeks is a good treatment option for older patients with mild asthma that is not well controlled by low-dose ICS monotherapy. Elevated BMI is also associated with poorer asthma control in older patients, regardless of the treatment option. To assess treatment changes such as this, monitoring both ACT and PFS can be used to predict asthma control in response to antiasthmatic drugs in older patients.





 XML Download
XML Download