

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Idiopathic hypereosinophilic syndrome (IHES) is a group of disorders characterized by the overproduction of eosinophils resulting in inflammatory damage to multiple organs, including skin, heart, lung, gastrointestinal tract, and nervous system.1 Signs and symptoms associated with lung involvement are relatively common, occurring in approximately 40% of IHES patients.2,3 However, despite frequent lung involvement, acute respiratory distress syndrome (ARDS) is rarely seen in conjunction with IHES, with only a few cases described in the literature to date.4,5 This is the first case report of IHES presented with ARDS in Korea.
CASE REPORT
A 37-year-old male visited the emergency department at Samsung Medical Center, Seoul, Korea, presenting with a chief complaint of dyspnea. Initial symptoms had begun 1 week prior to his visit, characterized by fever and chills, followed by progressive respiratory difficulty. He appeared acutely ill. A crackling sound was heard upon chest examination. His heartbeat was regular without a murmur. A purplish discoloration of the right ankle was observed, but there were no local heat or tenderness. Initial blood pressure was 163/91 mmHg, pulse rate was 114 beats/min, respiratory rate was 24 breaths/min, and body temperature was 38℃. Oxygen saturation was initially detected as 87%, and increased to 95% upon oxygen supplement via nasal cannula at 5 L/min. Following oxygen supplementation, arterial blood gas analysis (ABGA) showed a pH of 7.39, partial pressure of carbon dioxide (PaCO2) of 40.9 mmHg, partial pressure of oxygen (PaO2) of 113.7 mmHg, and oxygen saturation of 98%.
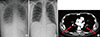
Laboratory tests revealed peripheral eosinophilia and thrombocytopenia with a white blood cell count of 22,580/µL (50% neutrophils, 31% eosinophils, 10% lymphocytes), Hb levels at 13.7 g/dL, and a platelet count of 26,000/µL. Prothrombin and activated partial thromboplastin times were 15 sec, and 35.4 sec respectively. Fibrinogen levels were within the normal range, but the concentration of D-dimer was markedly elevated at 26.69 µg/mL. Serum total IgE and ECP levels (939.4 IU/mL and 201.0 ng/mL, respectively) were both elevated, too. Tests for both anti-nuclear antibodies and anti-neutrophil cytoplasmic antibodies were negative. A test for parasites in the stool and serum were negative. Bone marrow biopsy showed normal cellularity with increased eosinophils. Fip1-like1 and platelet-derived growth factor receptor alpha (FIP1L1-PDGFRA) gene fusion was not detected. Patchy consolidation with ground-glass opacity in both lower lung zones was noticed in the initial chest radiography (Fig. 1A).
During the initial workup, the patient became progressively tachypneic with increased oxygen demand to 15 L/min via facial mask. The patient was transferred to the intensive care unit and oxygen supply was increased to 100% by high-flow nasal cannula. Despite supplementation, PaO2 levels remained low (49.9 mmHg) leading to a diagnosis of ARDS, and then the patient underwent intubation and mechanical ventilation.
Bronchoalveolar lavage (BAL) revealed marked eosinophilia (187/200 evaluated cells, 93.5% eosinophils). Skin biopsy of the right ankle showed diffuse eosinophilic perivascular infiltration of the dermis (Fig. 2A) and eosinophilic abscess of subcutaneous fat (Fig. 2B). Duplex sonography revealed deep vein thrombosis in the left popliteal, soleal, and peroneal veins. Nerve conduction test and electromyography showed neuropathy in the right posterior tibial nerve.
A diagnosis of IHES was reached based on the presence of peripheral and tissue eosinophilia, along with the exclusion of other causes of eosinophilia. High-dose corticosteroid (methylprednisone 1 mg/kg/day) therapy was initiated on the first day of admission. By day 3, eosinophil counts decreased to the normal range (Fig. 3). Extubation was performed on day 4 as a result of clinical and radiological improvements.
A chest CT scan was obtained on day 9 to evaluate symptoms of mild dyspnea despite the dramatic improvement seen by simple radiography (Fig. 1B). Pulmonary thromboembolism (PTE) was detected in the bilateral lobar and segmental branches of the pulmonary arteries (Fig. 1C), and we started anticoagulant therapy. On day 23, the patient was discharged from the hospital with a gradual tapering of corticosteroids.
DISCUSSION
In 1975, Chusid et al.6 established the basic guidelines for diagnosis of IHES, which is still in use today. Criteria include blood eosinophilia>1,500 cells/µL for longer than 6 months, lack of evidence for parasitic, allergic, or other known causes of eosinophilia, and the presence of organ damage or dysfunction related to hypereosinophilia. However, recently these criteria have been changed; when marked eosinophilia and obvious tissue damage such as cardiac involvement are observed, the initiation of treatment is recommended regardless of the duration of eosinophilia.7 Our case fulfills the diagnostic criteria for IHES except the duration of peripheral eosinophilia.
Lung involvement is relatively common in IHES. In a previous study, of 49 patients with IHES, 63% had more than one kind of respiratory symptoms, and 43% showed abnormal findings by chest radiography or CT scan.8 However, despite the fact that lung is frequently involved in IHES, there have been only a few cases that have presented ARDS. ARDS is an acute and diffuse inflammatory lung injury that leads to increased pulmonary vascular permeability, increased lung weight, and a loss of aerated tissue.9 Approximately 60 distinct etiologies including eosinophilic pneumonia have been recognized for ARDS, among which severe sepsis and bacterial pneumonia are the most common.10-14
Our patient presented fever and dyspnea initially, and chest radiography showed bilateral parenchymal infiltration. Intubation was performed due to ARDS, and bronchoscopic examination with BAL revealed profound alveolar eosinophilia. The main cause of ARDS was thought to be severe eosinophilic parenchymal inflammation of the lungs. This diagnosis was confirmed by rapid clinical and radiologic response to high-dose corticosteroid therapy.
Thromboembolic complication is a common cause of mortality and morbidity in patients with IHES. About 25% of IHES patients experience thromboembolisms, with a mortality rate of 5%-10%.15 In this case, a chest CT scan on hospital day 9 revealed a thromboembolism in the bilateral pulmonary arteries. PTE was suspected considering the initial presentation, which included purplish discoloration of the right ankle, thrombocytopenia, D-dimer elevation, and deep vein thrombosis in the left popliteal, soleal, and peroneal veins. However, the marked eosinophilia in BAL fluid and the dramatic response to corticosteroid therapy prior to initiation of anticoagulant therapy suggest that primary cause of respiratory failure is parenchymal lung involvement of IHES, rather than PTE.
Corticosteroids are a first-line therapy for FIP1L1-PDGFRA-negative IHES.16,17 About 85% of patients on corticosteroid therapy reach partial or complete remission by 1 month.17 For patients not responding to corticosteroids, second-line therapies such as hydroxyurea, interferon-α, anti-IL5 antibodies, or anti-CD52 antibodies can be considered.18 In the present case, peripheral eosinophilia and involvement of the skin and lung were successfully treated by high-dose corticosteroid alone.
In summary, we describe a rare case of IHES with ARDS due to eosinophilic lung involvement, which showed a dramatic response to high-dose corticosteroid therapy.


 XML Download
XML Download