

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Angioedema without urticaria is an uncommon skin disease with a prevalence of 1.6%-2.2% and has been classified as either hereditary or acquired.1 Angioedema can be further stratified according to the mediators that induce vascular leakage: bradykinin, histamine, various factor-mediated, and idiopathic angioedema, which is a poorly understood syndrome.2,3 Angioedema with eosinophilia (AE) can be classified to idiopathic angioedema.
AE was first reported in 1984 by Gleich et al.;4 thereafter, about 100 cases have been reported. The cause of the increase in eosinophils and how it induces angioedema in this disorder remains unclear, but seems to be associated with cyclic alterations in serum interleukin (IL)-5 or GM-CSF levels.5,6,7 The benign clinical course of this disease and its lack of association with end organ damage distinguishes it from idiopathic hypereosinophilic syndrome (HES), which may involve internal organs and cause mortality,8 although some consider AE an overlapping syndrome with HES.9
In 2012, Nakachi et al. summarized 11 cases of AE treated at a single hospital in Japan and observed the characteristic features and clinical course of AE in Japanese patients.10 In Korea, several case reports of AE have been published sporadically since 1999. Here, we retrospectively analyzed Korean AE patients from 3 KoreaUniversity Hospitals and summarized their clinical characteristics and course.
MATERIALS AND METHODS
From October 2007 to September 2012, 10 adult patients with AE were analyzed retrospectively from 3 centers (Ajou University Hospital, Hallym University Sacred Heart Hospital Anyang, and Hallym University Sacred Heart Hospital Dongtan) in South Korea. Diagnosis was based on peripheral angioedema on distal extremities that developed concurrently with peripheral eosinophilia (≥1,000/L) and improved while eosinophil count decreased. Eosinophilia due to preexisting underlying diseases, such as tumor, parasite infection, and current uncontrolled allergic disease, was excluded. The age, sex, preexisting underlying disease, development of fever, body weight gain, and internal organ involvement data were collected from medical records. The duration of symptoms and eosinophilia, corticosteroid dose, and treatment outcomes were also noted. Laboratory parameters, including white blood cell (WBC), eosinophil, and WBC differential counts, serum immunoglobulin (Ig)G, IgA, IgM, and IgE levels, C-reactive protein (CRP) level, and erythrocyte sedimentation rate (ESR), were analyzed. We classified AE into 2 groups, episodic-type (EAE) with more than 2 episodes of AE and non-episodic type (NEAE) with only 1 episode of AE.11
RESULTS
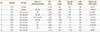
The clinical characteristics of 10 patients diagnosed with AE are summarized in Table 1. Nine of the study subjects were female, and their mean age was 28.5±5.3 (range, 23-38) years at diagnosis. Peripheral edema was observed in distal extremities symmetrically, mostly in the hands and feet without urticaria. Seven patients had a history of allergic disease, such as allergic rhinitis, atopic dermatitis, and bronchial asthma. However, none of these patients had current symptoms, as their underlying allergic diseases were mild and in a state of remission; therefore, we determined that their eosinophilia was not due to underlying allergic disease. No internal organ involvement was documented in any patient. Body weight increase was observed in only one patient (patient 2; 4 kg, 8% of total body weight). All patients had hypereosinophilia, ranging from 1,000 to 23,400/L. The mean total IgM level was 228.9 mg/dL (reference range, 40-260 mg/dL), ranging from 114 to 391 mg/dL. Most patients showed normal ESR and CRP level except patient 5, who showed an elevated ESR of 52.4 mm/h.
Two (20%) of the study subjects had recurrent episodes of AE and were classified as episodic type (EAE). These 2 patients were young females who tended to have higher levels of serum IgM compared to the patients with non-episodic type (NEAE; 344.0 mg/dL vs. 228.9 mg/dL). Systemic steroids were administered to control their symptoms. The angioedema and eosinophilia in patient 2 improved within 3 days, while patient 1 suffered from frequent recurrences of angioedema with elevated peripheral eosinophil counts when tapering the dose of systemic steroid for 3 years. Therefore, to reduce the patient's steroid requirement, anti-IgE antibody (omalizumab; monthly, 150 mg) was administered for 6 months. Since the beginning of treatment, there was no evidence of recurrence during the 18-month follow-up period after stopping all medications, including the systemic corticosteroid.
Eight (80%) of the patients were NEAE and had experienced only one episode of AE. One patient was male, while the others were female. Six (75%) of the eight patients had history of allergic disease, which was mild and in well-controlled or remission states. All of these patients showed normal serum IgM levels. Four (50%) of the patients with NEAE recovered without systemic steroids, and another 4 (50%) patients required systemic steroids to control their diseases. The decision of steroid use and dosage was determined by responsible allergists. None of these patients experienced an episode of recurrence during the follow-up period (average, 18 months) after recovery.
DISCUSSION
Since Gleich et al. reported the first four cases in 1984, EAE has been characterized by recurrent episodes of angioedema, fever, leukocytosis, eosinophilia, elevated serum IgM, increased body weight, and a benign clinical course lacking internal organ involvement.4 Additional cases have been reported sporadically in Europe and the United States.12,13,14,15 In 1998, Chikama et al. reported a non-episodic variant, which was limited to a single attack. The non-episodic variant consisted of a single attack of persistent edema of the extremities associated with peripheral eosinophilia, normal immunoglobulin levels, and lack of internal organ involvement.11 After that report, there has been effort to define the difference(s) between the 2 phenotypes of AE: episodic and non-episodic. In the present study, 20% of AE patients had a history of recurrent attacks and could be classified as EAE. Constitutional symptoms, such as fever or weight gain, were not observed in any of the study subjects. All of the subjects tended to have high serum IgM and eosinophil counts, as compared to those with NEAE. However, the majority of NEAE cases have been reported in Japanese and Korean populations.12,16,17,18 In Japanese data, most of the AE patients were young females, and usually presented with a single, transient episode of AE without constitutional symptoms such as fever or weight gain. They also tended to have normal immunoglobulin levels, and about 70% of these patients recovered without systemic corticosteroid treatment.10,12 In the present study, 80% of the study subjects had NEAE, similar to the Japanese data. The majority of our patients were young females with localized edema in distal extremities without serious constitutional symptoms, including recurrence, fever, significant weight gain, and internal organ involvement. They also showed normal levels of IgM, CRP, and ESR. Similar to our data, among the 10 cases of AE that have been published in Korea, eight (80%) were of non-episodic type. The reason that NEAE is more common in Japanese and Korean cohorts compared to Western populations may be due to racial or ethnic differences.10 Previous case reports of Korean patients demonstrated that some cases of NEAE presented with a single episode but with constitutional symptoms, such as fever, significant weight gain, and/or mildly elevated serum IgM. These patients also required systemic steroids to control their disease.19,20,21,22 These findings suggest no clear distinction between episodic and non-episodic types of AE. NEAE may be a milder form of EAE rather than a distinct disease, as suggested by others.12,17,23
For the treatment of EAE, systemic corticosteroids have been administered widely. However, some cases of EAE suffered from frequent recurrences and steroid dependency, as observed for patient 1 in this study. There have been a few case reports demonstrating successful treatment of steroid-dependent EAE using imatinib (a tyrosine-kinase inhibitor used in the treatment of multiple cancers) and intravenous immunoglobulin.24,25 In the present study, patient 1 was treated with anti-IgE antibody. P previous cases of chronic eosinophilic pneumonia and chronic urticaria treated with anti-IgE therapy were reported.26,27 Anti-IgE therapy results in the rapid reduction of free IgE levels and the down-regulation of FcεRI on basophils, mast cells, and other inflammatory cells. Moreover, anti-IgE therapy exerts profound and significant reductions in airway and tissue eosinophilia in patients with mild allergic asthma and on allergen-induced seasonal increases in circulating and tissue eosinophils in subjects with allergic rhinitis.28 These findings suggest that anti-IgE therapy can be considered a steroid-sparing option for EAE. One report has suggested that NEAE may be a self-limiting disease.10 However, most cases of NEAE are treated with systemic steroids, as it may sometimes progress rapidly and present with severe clinical symptoms.29 Considering that NEAE can be classified as a less severe form of EAE, and EAE can present like an overlapping syndrome with HES,30,31 the appropriate use of systemic steroids is beneficial for patients with EAE who expect rapid relief from their symptoms and to prevent the progression of this disease with careful follow-up.
In conclusion, we are the first to report the clinical characteristics of 10 patients with AE in Korea. Although NEAE was more common, systemic steroids can be used to control symptoms and prevent disease progression.
 XML Download
XML Download