

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Allergic asthma (BA) and allergic rhinitis (AR) are chronic airway inflammatory diseases characterized by eosinophilic infiltration in response to inhalant allergens in genetically susceptible patients. Both conditions are considered to be one airway disease that show different features.1 In many epidemiological studies, 60%-80% of BA patients have concurrent AR, while the prevalence of BA in patients with AR varies from 10%-40%.2,3 Moreover, AR patients are 2-6 times more likely to have BA compared with patients without AR.4
Staphylococcus aureus (SA) is one of the most common human bacterial pathogens and produces enterotoxins that act as toxins and superantigens. Staphylococcal enterotoxins are a family of structurally related proteins comprised of different serological types: Staphylococcus enterotoxins A (SEA), B (SEB), C, D, E (up to U), and toxic shock syndrome toxin-1 (TSST-1).5 The stimulatory role of superantigens in the development of inflammation in chronic rhinosinusitis and nasal polyposis has been documented. It has been postulated that SA and its products are related to the pathogenesis of allergic inflammatory diseases, including rhinitis and atopic dermatitis.6,7,8 Although a high prevalence of serum specific IgE to superantigens has been reported in AR and BA patients,2 their role has not been clearly defined. Therefore, this study evaluated the clinical significance of serum specific IgE to staphylococcal superantigens in patients with BAwAR and AR.
MATERIALS AND METHODS
We recruited BAwAR patients (group I, n=100), AR patients (group II, n=100), and healthy controls (group III, n=88) from Ajou University Hospital. The subjects in groups I and II had been clinically diagnosed by physicians, and they were sensitized to house dust mites: Dermatophagoides pteronyssinus (Dp) and Dermatophagoides farinae (Df). Serum specific IgEs to SEA, SEB, and TSST-1 were measured using the ImmunoCAP system (Phadia, Uppsala, Sweden). Patient blood samples were obtained at the time of diagnosis. Allergen-specific IgE levels >0.35 kUA/L were considered positive. Informed consent was obtained from each subject and the study protocol was approved by the ethics committee at Ajou University Medical Center, Korea. The levels of IgE to SEA, SEB, and TSST-1 in each group were analyzed using the Mann-Whitney U-test or binary regression test after adjusting for age, while their prevalence was compared using the chi-square test.
RESULTS
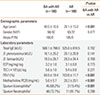
The clinical characteristics of the study subjects are summarized in Table 1. All patients enrolled in this study were sensitized to house dust mites, which are a well known risk factor for the development of BA in AR patients. There were no differences in demographic characteristics between groups I and II, except age. The mean age of group II was younger than that of group I (P<0.001). For laboratory parameters, FEV1 (%) and the provocation concentration of methacholine required to reduce FEV1 by 20% from the baseline value (PC20) were significantly lower in group I. Sputum eosinophils were significantly more numerous in group I (P<0.001) compared to group II. Other parameters, such as serum specific IgE level to Dp and Df, the levels of eosinophilic cationic protein (ECP), and the total eosinophil count, were not significantly different between the 2 groups.
The rate of positive serum IgE to SEA, SEB, and TSST-1 was the highest in group I (22, 21, and 27%, respectively), followed by group II (11, 14, and 21%) and group III (4.5, 3.4, and 2.3%). All of these rates were significantly higher in group I than in group III. The rate of positive response to SEA was significantly higher in group I than in group II (Fig. 1). Moreover, absolute values of serum specific IgE to SEA, SEB, and TSST-1 were significantly higher in group I (0.300±1.533 kU/L, 0.663±2.933 kU/L, and 0.581±1.931 kU/L, respectively) and group II (0.502±2.011 kU/L, 0.695±3.337 kU/L, and 1.067±4.688 kU/L, respectively) compared with those in group III (0.03±0.133 kU/L, 0.03±0.14 kU/L, and 0.028±0.112 kU/L, respectively) (Fig. 2). Regarding laboratory parameters according to the presence of specific IgE to staphylococcal superantigens, serum total IgE levels were significantly higher in patients with IgE to each superantigen compared with those without IgE. The levels of serum specific IgE to Dp and Df were also higher in patients with IgE to TSST-1 (P=0.005 and P=0.032, respectively). Finally, the peripheral blood eosinophil counts were significantly higher in patients with high specific IgE to SEA or SEB (P=0.005 and P=0.032, respectively), and ECP levels were significantly higher in patients with IgE to SEB (P=0.045) (Table 2). These differences were more pronounced in patients with specific IgE to more than 2 superantigens concomitantly (data not shown).
DISCUSSION
Since it was discovered that innate and adaptive immunity were involved in the development of allergic inflammation and that SA is common in the upper respiratory tract, the role of SA and its toxins have been studied in many allergic diseases. Previous studies showed that SA may aggravate AR symptoms and be involved in the pathogenesis of severe asthma.9,10,11 First, we found that the positive response rate and absolute values of serum IgE to superantigens were significantly higher in both the BAwAR and AR groups compared to the healthy controls. In addition, the rate of a positive IgE response to SEA was significantly higher in BAwAR patients compared to AR patients. Although many studies have reported on the role of SA in allergic diseases, this is the first study to compare the positive rate of serum specific IgE to staphylococcal superantigens between BAwAR and AR patients who were sensitized to house dust mites.
AR is an allergic disease of the upper respiratory tract, while BA is an allergic disease of the lower respiratory tract. Although both conditions involve allergic inflammation, it is not understood whether a patient will present with only AR or if it will progress to BA. In this study, we hypothesized that the immune response to staphylococcal superantigens, a major type of bacterial exotoxin, might cause these differences. Also, this response could potentiate the inflammatory process at least 2 ways. First, the exotoxins are superantigens capable of extensive T-cell activation.12,13 Unlike other types of antigen, superantigens do not require processing by antigen-presenting cells but rather bind directly to the major histocompatibility complex class II.14 Superantigens bind to the T-cell receptor in the Vβ region and activate up to 30% of all T cells. Superantigens can generate a massive release of Th1 and Th2 cytokines at the exposure site. Second, bacterial toxins may act as typical allergens that stimulate the production of IgE specific to these proteins.15 Repetitive exposure has the ability to generate both a superantigen and a chronic allergic response through IgE production. Theoretically, the additive effect of these 2 processes should favor a lymphocytic and eosinophilic infiltration in exposed tissue.
We observed significantly higher levels of blood eosinophils, specific IgE to indoor allergens, and total IgE in patients with high serum specific IgE to staphylococcal superantigens. Eosinophilic inflammation and IgE production in response to indoor allergens were greater in patients with IgE responses to more than 2 staphylococcal superantigens concomitantly compared to those with an IgE response to only one staphylococcal superantigen. High levels of IgE to indoor allergens, such as house dust mites, and severe eosinophilic inflammation are risk factors for allergic diseases.16,17,18 These findings suggest that IgE to staphylococcal superantigens may be a risk factor for eosinophilic inflammation and the development of an IgE response to indoor allergens. A possible limitation of the study was the close correlations among the measured staphylococcal superantigens. Further prospective investigations are required to evaluate the roles played by each staphylococcal superantigen and by the IgE response to staphylococcal superantigens in the progression of AR to BA.
In conclusion, these findings suggest that IgE responses to staphylococcal superantigens are prevalent in sera of both BAwAR and AR patients, and may augment the IgE response to indoor allergens and eosinophilic inflammation.



 XML Download
XML Download