

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Primary immunodeficiency (PID) diseases are a diverse group of rare genetic disorders that affect the development and/or function of the immune system. Affected individuals are predisposed to an increased rate and severity of infections, allergy, autoimmunity, and malignancy.1 With the exception of immunoglobulin A (IgA) deficiency, PID diseases are considered to be rare; the estimated prevalence of these disorders in the United States is approximately 1 in 1,200 live births. IgA deficiency is the most common PID, occurring in approximately 1 in 300 to 1 in 500 persons.2 Early detection of PID is important for timely intervention before serious infections compromise the patient's general condition.3,4 However, failure to recognize these conditions remains a major challenge for clinicians worldwide. The problem is that general practitioners lack familiarity with these rare disorders and lack guidance regarding the appropriate use of immunological investigations.5 Moreover, considering that other diseases, including anatomic defect, allergy, and metabolic disorders, are primarily associated with recurrent infections, it is crucial for the general practitioner to determine which patient should be evaluated for PID.6-8 In an attempt to facilitate clinical reasoning concerning when to suspect PID in clinical practice, National Primary Immunodeficiency Resource Center9 developed a list of 10 warning signs of PID (Table 1). Physicians should consider PID if a patient encounters one or more of these warning signs, which basically focus on the site, severity, and frequency of infection. Because the scope of PID clinical presentations includes manifestations other than infection, Cunningham-Rundles and colleagues10 developed an immunodeficiency-related (IDR) score to identify the likelihood of finding immunodeficiency among patients undergoing immune evaluation. The score includes several medical conditions associated with PID (Table 2). An IDR score of ≥6 was considered by the authors to be a threshold indicating a significant number of illnesses with the likelihood of PID.10,11
Egypt is a country with nearly 83 million inhabitants (according to the last national population census in 2009), of which 9 million are below the age of 5 years. The estimated mortality rate among children less than 5 years reached 21/1,000 live births, of which pneumonia and gastroenteritis accounted for 17% of all deaths.12 Unfortunately, no national registry of PID diseases exists in Egypt and currently only 160 Egyptian PID children are registered with the European Society for Immunodeficiencies (ESID).13 These patients are affiliated with two PID centers in the country: one at Ain Shams University (100 cases) and the other at Cairo University (60 patients). These figures clearly do not represent the actual burden of PID diseases in Egypt. We believe that many PID patients die before diagnosis probably because awareness of these diseases among clinicians is suboptimal. In a previous study, we found a significant delayed diagnosis, severe morbidity, and high mortality rates among patients with severe PID phenotypes,14 indicating that more effort is needed to implement educational campaigns that target general practitioners and pediatricians. Thus, in the present study, we aimed to test the validity of the 10 warning signs and IDR score as predictors of PID disease, and to identify the most significant warning signs that would help physicians to identify PID cases in clinical practice.
MATERIALS AND METHODS
This study was approved by the ethical committee of the Pediatric department, Faculty of Medicine, Ain Shams University.
The medical records of 204 patients who presented with recurrent, severe, or unusual infection at Ain Shams University Children's Hospital during the last 7 years were reviewed. Based on the World Health Organization (WHO) diagnostic criteria of PID,15 a diagnosis of PID disease was established in 92 patients. In the remaining 112 patients, laboratory investigations failed to reveal underlying PID disease. For each patient, an evaluation sheet was designed to describe demographic data, including age at onset of symptoms, age at diagnosis, the diagnosis lag, which represents the time elapsed between onset of symptoms and diagnosis, sex, parental consanguinity, family history of PID, history of sibling death due to infections, as well as clinical and laboratory findings at the time of diagnosis. The performed laboratory work-up of these patients included measurement of the complete blood count with differential, C-reactive protein level, erythrocyte sedimentation rate, cultures from infection sites, serum immunoglobulins (IgA, IgG, IgM, and IgE), delayed cutaneous hypersensitivity (purified protein derivative, Candida skin test), peripheral blood lymphocyte subsets, including the basic panel of T-cell subsets (CD3, CD4, and CD8, B-cell [CD19], and natural killer cell [CD56/16]) by flow cytometry. Other laboratory investigations, including nitroblue tetrazolium dye testing, measurement of serum alpha fetoprotein, and assessment of CD18/CD11 on neutrophils by flow cytometry, were performed when indicated. Both complement hemolytic activity (CH50) and genetic testing were not available in our laboratories and hence were not evaluated. Imaging studies such as chest radiography, computed tomography (CT), echocardiography, and abdominal ultrasonography were employed in some cases. Additionally, each patient was evaluated for the frequency of each criterion of the current version of the 10 warning signs (Table 1) and given a score out of 10, representing the number of positive warning signs. Similarly, the IDR score (Table 2) was calculated and the score weight of each patient represented the sum of score descriptions acquired from the date of symptom onset to the date of diagnosis. Chronic conditions were counted only once in a 12-month period. The study was approved by the ethical committee of Ain Shams University. Informed consent was obtained from the legal guardian of every patient enrolled in the present study.
Statistical analysis
The patients' data were analyzed statistically using SPSS version 12 for Windows (SPSS Inc., Chicago, IL, USA). Comparisons between categorical data of the 10 warning signs were performed using the chi-squared test and logistic regression analysis. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated to determine the least number of the 10 warning signs that would help identify cases with PID. Receiver operating characteristic (ROC) curve analysis was used to determine the best cut-off value of the IDR score in predicting PID. A P value less than 0.05 was deemed statistically significant.
RESULTS
Disease distribution of the cohort
Children with definable PID constituted 45% of the cohort and, according to the International Union of Immunological Societies (IUIS) Primary Immunodeficiency Classification Committee,16 patients were distributed among 18 diseases of 5 main categories of PID. No patient was identified in the categories of defects in innate immunity, autoinflammatory disorders, or complement deficiencies. Details of different PID diagnoses are listed in Table 3. Of the cases in the category of combined T and B immunodeficiencies 50% had severe combined immunodeficiency (SCID). and 30% were collectively categorized as unclassified T-cell immunodeficiencies. These cases were considered as unclassified because the molecular tests required to identify various subtypes of combined T- and B-cell immunodeficiencies as listed in the IUIS classification16 were not available in our laboratories. Patients with unclassified immunodeficiencies presented with clinical manifestations of SCID, and were either siblings of diagnosed SCID patients or had a history of previous sibling death.
Conversely, the group of patients with no definable PID disease included 42 patients with recurrent infections due to other underlying diseases that often predispose to frequent infections, including bronchial asthma (25 patients), Down syndrome (6 patients), congenital heart disease (5 patients), protein-calorie malnutrition (4 patients), and pulmonary tuberculosis (2 patients). The remaining 70 patients were grouped together under the term "unexplained recurrent infection" because these cases developed either two major infections or one major and recurrent minor infection per year. However, the necessary laboratory and radiological investigations failed to reveal a definite underlying cause of recurrent infections. The spectrum of unexplained recurrent infections included at least two attacks of gastroenteritis and an episode of bronchopneumonia (48 patients) and two attacks of lobar pneumonia complicated with either septicemia (16 cases) or empyema (6 patients).
Demographic characteristics of the cohort
The age at onset of symptoms, age at diagnosis, and the diagnosis lag showed considerable variations among different PID categories (Table 4). The diagnosis delay was evident in all PID diseases, including the most severe phenotype, SCID, of which the median diagnosis lag was 3 months (range, 0.5-4 months). In other less severe diseases, the diagnosis delay was up to 6 years. As a consequence of delayed diagnosis and referral, 24 patients (26%) died from severe septicemia soon after diagnosis. Male predominance was evident among PID cases (67%). Boys were also affected by autosomal disorders due to the high rate of parental consanguinity, which was significantly higher among PID cases (60%) than non-PID cases (33%). Additionally, a positive family history of PID and a history of previous sibling death from infection were recorded more frequently among patients with PID as compared with non-PID cases (Table 4). In 16 PID patients (17%), a triad of parental consanguinity, positive family history of PID, and sibling death of infection was elicited.
Frequency of the 10 warning signs in the cohort
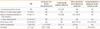
Each patient with PID exhibited at least one criterion of the 10 warning signs, while 32 patients displayed no definable PID (28%) and reported no warning signs. The frequency of each criterion of the 10 warning signs was significantly higher among patients with definable PID compared to those with no definable PID (Table 5). Among patients with PID the most frequent warning sign was the need for intravenous antibiotics, whereas two or more serious sinus infections within 1 year was not observed in any patient. Failure to thrive was more frequent in the categories of combined T- and B-cell immunodeficiencies and predominantly antibody deficiency. Recurrent deep-skin and organ abscesses and deep-seated infections were significantly more frequent in the category of congenital defects in phagocyte number, function, or both. The overall significance of having any of the 10 warning signs to suspect PID showed that when at least one warning sign was exhibited, the sensitivity was 100% (confidence interval [CI]: 95-100%), the specificity was 26% (CI: 19-35%), the PPV was 53%, and the NPV was 100%. Meeting at least two criteria of the 10 warning signs led to a sensitivity of 94% (CI: 86-97%), specificity of 64%, (CI: 55-73%), PPV of 68%, and NPV of 92% (odds ratio [OR]: 26; CI: 10-64%). When at least three criteria of the 10 warning signs were fulfilled, the sensitivity was 77% (CI: 68-85%), the specificity was 86% (CI: 78-91%), the PPV was 82%, and the NPV was 82% (OR: 20; CI: 10-42%).
Warning signs most predictive of different PID categories
A family history of PID was the most significant predictor of PID (Table 6). The other three significant warning signs were the need for intravenous antibiotics, recurrent deep-seated infections, and failure to thrive. When using these four warning signs in addition to parental consanguinity and a history of sibling death, 81% of patients with PID could be correctly identified. Although parental consanguinity and a history of sibling death due to infection are not yet included in the current version of the 10 warning signs, they were significant predictors of PID in our series. In fact, parental consanguinity and a history of sibling death due to infection were the only predictors of patients in the category of combined T- and B-cell immunodeficiencies. As shown in Table 6, a history of sibling death was 138-fold more common among patients with combined T- and B-cell immunodeficiencies compared to those with no definable PID, and 92% of these patients could be correctly identified if both sibling death and parental consanguinity were considered. Additionally, 92% of patients with defects in phagocyte number, function, or both could be identified if a history of sibling death and family history of PID were considered. Meanwhile, 87% of patients with other well-identified immunodeficiency syndromes could be identified when a triad of family history, parental consanguinity, and need for intravenous antibiotics were considered. The need for intravenous antibiotics was the strongest warning sign in identifying patients with predominantly antibody deficiency, and when combined with recurrent pneumonia and parental consanguinity, 84% of patients could be correctly diagnosed.
Performance of the IDR score in the cohort
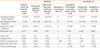
Patients with PID had a significantly higher IDR score than those without PID (Z=6.7; P<0.001). The median value of the IDR score was 8 (range, 2-24) in patients with PID and 6 (range, 2-19) in non-PID patients. As illustrated in Table 4 and Fig. 1, a wide range of IDR scores was observed within each category of PID. The Kruskal-Wallis test with pair-wise comparisons adjusted for multiplicity (Bonferroni correction) showed that patients with congenital defects of phagocyte number and/or function had comparable IDR scores to those without PID (P=0.16), while other PID subgroups had significantly higher IDR scores as compared with non-PID patients (P≤0.01). Patients with combined T- and B-cell immunodeficiencies, those with predominantly antibody deficiency, and patients with other well-defined immunodeficiency syndromes had significantly higher IDR scores than those with congenital defects of phagocytes (P=0.001). Meanwhile, patients with predominantly antibody deficiency had a significantly higher IDR score than those with combined T- and B-cell deficiencies (P=0.03; Table 7 and Fig. 1).
Conversely, the weight of the IDR score did not correlate with the age at diagnosis of PID (r=0.2; P=0.09), indicating that the score was influenced by disease severity rather than the age of patients. The overall performance of the IDR in detecting PID conditions was evaluated using the ROC curve, which showed that the best cut-off value of the IDR score to predict PID was 6, at which the sensitivity was 66%, the specificity was 75%, the PPV was 69%, and the NPV was 73%. The reliability of the IDR score in detecting patients with PID using kappa statistics was found to be good (kappa: 0.4; P=0.0001). Notably, the IDR score was <6 (median, 3; range, 2-5) in 18 PID patients (19%) who elicited only one warning sign, but PID was suspected because they were either siblings of PID patients in the cohort or had a history of repeated sibling death from infection.
DISCUSSION
The present study clearly demonstrates that PID diseases are underdiagnosed in Egypt. In the present study, various PID diseases were identified in 45% of cases with recurrent infection observed at a single tertiary hospital. Delayed diagnosis was evident in all PID diseases, reflecting poor knowledge of PID among clinicians. The overall evaluation of the 10 warning signs revealed that at least two warning signs should be fulfilled to identify nearly two-thirds of PID cases. Similar to other studies,17,18 the need for intravenous antibiotics to clear infection was the most significant warning sign reported in PID patients, denoting that physicians and general practitioners should consider the diagnosis of PID in children when intravenous antibiotics are needed to clear infection. However, the strongest predictors of PID in our cohort were a positive family history of PID, parental consanguinity, and previous sibling death from infection. Indeed, high rates of parental consanguinity in PID patients were previously reported in Middle Eastern countries, including Egypt,14 Iran,19 Kuwait,20 and other North African countries.21 A positive family history of PID was also the strongest predictor of PID in two tertiary pediatric immunology hospitals in the north of England, although 30% of those cases were of Asian-Pakistani descent in whom parental consanguinity was high.17 Failure to thrive was a significant predictor of PID in the entire cohort. However, unlike the study of Subbarayan and associates,17 this sign was not a significant predictor of combined T- and B-cell immunodeficiencies, probably because one-third of non-PID patients exhibited failure to thrive. Although the only significant predictors of combined T- and B-cell immunodeficiencies in the present study were consanguinity and a history of repeated sibling death due to infection, it is possible that deceased siblings had unidentified PID. Thus, physicians must be vigilant to the likelihood of severe PID when a history of previous sibling death and/or parental consanguinity is identified in infants with infection. Fig. 2 illustrates the most significant warning signs found in our study that would help general practitioners to suspect PID among children with one or more of these signs. If available, a neonatal screening test for severe life-threatening PID diseases, such as SCID, will provide timely diagnoses and improve the management and prognosis of such conditions.23
Recently, the feasibility of promoting the use of the 10 warning signs as predictors of PID has been questioned. Specifically, if these signs are considered to be a screening tool for PID, many patients who manifest with atopy,24 autoimmunity, malignancy, or initially present with fulminant infections will be missed.25 In a recent publication, Modell and colleagues26 acknowledged the 10 warning signs to be a useful tool to promote awareness among PID families, the general public, and medical practitioners, but urged for the development of additional tools that facilitate identification of patients at high risk for PID.
Conversely, the cut-off value of the IDR score in predicting PID in our cohort was similar to that in other series,10,11,27 indicating that nearly 75-80% of PID cases could be identified at a score ≥6. However, our data showed that the IDR score did not help in the diagnosis of severe life-threatening PID diseases, because nearly one-fifth of PID patients had scores <6 and their diagnoses could have been missed if the IDR score was the only predictor of PID. Undoubtedly, appropriate clinical and laboratory assessments are required to confirm or exclude the suspicion of PID. Education regarding the various manifestations of PID diseases should target not only general practitioners and pediatricians, but also specialists in hematology, oncology, rheumatology, and neurology.25 To improve the recognition of PID diseases in children, ESID has recently developed a multistep diagnostic protocol for PID diseases28 that describes the various clinical presentations of PID disease and the essential laboratory tests required at the initial step of evaluation. Thus, early identification and timely referral of suspected cases to a specialized PID center may be achieved, allowing for more detailed investigations and genetic diagnoses,29 which are important to guide the treatment and follow-up of PID patients, as well as genetic counseling of families.
Finally, our study possessed some limitations. First, the study was conducted on a small number of patients who presented at a tertiary hospital, which made it difficult to evaluate the prevalence of different PID diseases in the entire country. Second, patients in the present cohort presented at a tertiary hospital because they either had critical acute illnesses or chronic difficult-to-treat conditions; thus, the cohort was biased towards the severe forms of PID diseases as well as severe and complicated non-PID conditions. Additionally, advanced molecular and genetic studies are not available in Egypt; hence, we could not confirm the diagnosis of many subtypes of PID diseases listed in the IUIS classification16 that require molecular analysis for diagnosis.
In conclusion, the present study represents an evidence-based analysis of the 10 warning signs and IDR score as predictors of PID. Our data showed that only 4 of 10 warning signs were significant in identifying PID, of which a family history of PID was the strongest predictor. Parental consanguinity and a history of sibling death were two additional significant warning signs in our community. A high index of suspicion is still the mainstay for detecting PID. Negative scoring of either the 10 warning signs or the IDR score must not exclude PID diagnosis if clinically suspected, and early referral to a specialized center should be considered. It is essential to encourage genetic counseling of affected or high-risk families, and to establish population-based neonatal screening of severe life-threatening PID diseases.







 XML Download
XML Download