

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Dipyrone is a non-opiod analgesic and antipyretic drug that belongs to the family of pyrazolones. In some countries dipyrone is banned because of the risk of agranulocytosis, while in others it is the leading analgesic and antipyretic drug, having an impressive amount of sales.1,2 Dipyrone is effective in postoperative analgesia and has opiate sparing effect.3,4 It is also used to improve cancer pain management and is one of the most frequently used drugs in palliative care.5 It is widely prescribed in the hospital setting2 and is also used as an over-the-counter analgesic.6
Dipyrone administration may cause adverse reactions of many types. Some reactions result from the inhibition of cyclooxygenase in patients with acetylsalicilic acid triad or chronic urticaria.7 Other reactions have an underlying immunologic mechanism, and are, at least in part, IgE-mediated.8 In Spain pyrazolones are the second cause of IgE-mediated reactions to drugs, preceded only by beta-lactam antibiotics.9
Drug challenge tests, the gold standard for the diagnosis of drug allergy, are time consuming and potentially dangerous. Thus many efforts have been made to find safe in vitro techniques to complement skin testing in the diagnosis of drug allergy, one of them being the basophil activating test (BAT).10 BAT has been proved to be useful in the diagnosis of allergy to neuromuscular blocking agents11 and antibiotics.12 There are several open questions for the application of BAT concerning the optimal drug concentrations and the threshold for positivity, the minimal basophils number to be analysed, drug solubility, blood sample storage and optimal incubation conditions.10 Flow cytometric determinations of basophil activation following stimulation with dipyrone represents an important technique for the in vitro diagnosis of immediate-type allergy and a suitable complement to other in vitro and in vivo tests used to quantify IgE.13 Several studies tried to establish the diagnostic value of flow cytometry in dipyrone allergic patients with different drug concentrations ranging from 0.25 mg/mL to 25 mg/mL using Beckton Dickinson or FlowCAST techniques.8,9,14
Recently, in a multicenter study, basophil activation by non-steroidal anti-inflammatory drugs (NSAIDs) occurred both in clinically hypersensitive patients and in apparently healthy controls (who tolerated NSAIDs) in a dose-dependent manner.15
Using Flow2CAST technique (Bühlmann Laboratories AG, Switzerland), NSAIDs were provided by the manufacturer and the vial concentration for dipyrone is 50 µg/mL, the recommended concentration in stimulation being 25 µg/mL.
Starting from this concentration, the aims of our study were (1) to determine if the BAT using lower concentrations of dipyrone than the ones previously tested by other authors, discriminates well between patients and controls; (2) to find the optimal concentration for dipyrone when performing BAT; (3) to establish the threshold for positivity using receiver operating characteristics (ROC) curve analysis; and (4) to determine the sensitivity and specificity of BAT in patients with IgE-mediated immediate-type hypersensitivity reactions to dipyrone.
MATERIALS AND METHODS
After the approval of the Research Ethics Committee of the University Hospital of Cluj-Napoca and after obtaining patients' informed consent, a total of 45 consenting adult patients with a positive history of an immediate hypersensitivity reaction to dipyrone and no history of intolerance to NSAIDs or chronic urticaria were prospectively included. From these ones we found 20 patients with documented positive skin tests suggesting IgE-mediated immediate-type hypersensitivity to dipyrone. Ten healthy controls without previous drug allergies (who tolerated intravenous dipyrone administered in our department) were also tested in vivo and in vitro. The subjects have not been taking steroid medication, H1 or H2 antihistamines or antidepressants. Intolerance to NSAIDs was excluded both in patients and controls by performing oral provocation tests with aspirin and diclofenac.
In vivo tests, the skin prick test (SPT) and the intradermal test (IDT), were performed using commercially available solutions of dipyrone (Algocalmin®, Zentiva, Bucharest, Romania): 2 mL injectable solution containing 1.05 g of dipyrone natrium monohydrate and water for injections. Normal saline solution (0.9% NaCl) was used to dilute the commercial dipyrone. The tested concentrations were 500 mg/mL for the SPT and 5 mg/mL for the IDT, as these were established as being the maximal non-reactive concentrations in healthy volunteers.16 The SPTs and IDTs were performed in conformity with international recommendations,17 and according to the testing methodology described by authors with experience in skin testing.18 We used 1% histamine as positive control and Normal saline solution as negative control. The SPT was considered positive when the wheal diameter was superior to 3 mm within 20 min. For IDT the wheal area was marked initially and 20 min after testing. An increase in diameter greater than 3 mm or the doubling of the initial injection wheal represented a positive result.17
For BAT, flow cytometric analysis of in vitro activated basophils was performed with Flow2Cast technique (Buhlmann Laboratories AG, Schonenbuch, Switzerland). We used 6 test tubes containing 50 µL of whole blood. The blood was collected into K-EDTA venipuncture tubes, up to the dedicated volume, from antecubital vein (no garrote). We performed the cell stimulation immediately after collection of the blood and we did not store the blood samples. The first sample was mixed with 50 µL of stimulation buffer as negative control. The next two samples were mixed with 50 µL solution of anti-FcεRI (a highly specific monoclonal antibody for the IgE receptor) and 50 µL solution of FMLP (an unspecific cell activator- the chemotactic peptide N-Formyl-Met-Leu), as positive controls. In the remaining 3 test tubes, 50 µL of dipyrone solution was added. The tested drug concentrations were 25 µg/mL (c1), 2.5 µg/mL (c2) and 0.25 µg/mL (c3). Subsequently, 20 µL staining reagent with two monoclonal antibodies, anti-CCR3-PE (human chemokine receptor labelled with phycoerythrin) and anti-CD63-FITC (or Gp53, a glycoprotein expressed on activated basophils), were added in each tube. The samples were incubated for 15 min at 37℃in a water bath. A prewarmed lysing solution of 2 mL was added to each tube and incubated for 10 min at room temperature. After centrifuging (500xg, 5 min) and washing, the cells were suspended in 300 µL wash buffer. The up-regulation of CD63 marker on the basophils was measured using Cell Quest programme (FACSCalibur Analyzer 2001, Becton Dickinson, San Jose, CA, USA). Our flow cytometer is equipped to detect forward scatter, side scatter and the two fluorochromes FITC and PE. Our laboratory limit of basophilic cells analyzed for allergies was set to 500. The gate was set by including the entire basophil population with low side scatter (SSC low) and calculating the percentage of CD63 positive cells compared to the total amount of basophilic cell gated.
The stimulation index (SI) for all subjects and all concentrations was analysed. The stimulation index is calculated as the percentage of activated basophils after stimulation with dipyrone divided by the number of basophils with no dipyrone stimulation.8,9 A receiver operating characteristics (ROC) curve analysis was performed for all concentrations with SI as discrimination variable. The reference standard was considered when patients had positive history of allergy to dipyrone and positive skin tests. The area under curve (AUC) and p-values were evaluated.19,20 The cut-off in the ROC curve is the closest point on the ROC curve to the point (0,1) which is the point of absolute classification, where sensitivity and specificity are 1.21 For better prediction, it is obvious to see if using the highest SI from all three dipyrone concentrations for each subject we could obtain an optimal SI as classification variable. We performed the ROC curve analysis for each of the three dipyrone concentrations, as well as for the highest stimulation indexes of all three dipyrone concentrations in patients and controls to calculate the optimal cut-off value (optimal stimulation index).
The result of BAT was considered positive when at least one of the SI for c1, c2 or c3 (the highest stimulation index) was higher than the threshold. In addition, the result was considered positive only when the percentage of activated basophils after stimulation with dipyrone was above 5% in order to rule out small unspecific activations, as previously described.8,9 Sensitivity was defined as the number of patients with BAT positive results per total number of patients and specificity as the number of controls with BAT negative results per total number of controls.
RESULTS
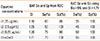
A total of 20 patients with IgE-mediated immediate-type hypersensitivity to dipyrone demonstrating positive skin tests (9 with positive SPT and 11 positive IDT) were tested both in vivo and in vitro, as well as 10 healthy controls. None of the controls presented a positive skin test (SPT and IDT) (Table 1).
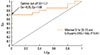
The cut-offs for BAT dipyrone positivity (stimulation index, SI) was calculated by ROCs. The ROC curves for c1, c2 and c3 dipyrone concentrations were performed (Table 2). For 25 µg/mL (c1) the AUC was 0.68 (0.49-0.86) (P=0.04), for 2.5 µg/mL (c2) the AUC was 0.69 (0.50-0.87) (P=0.03) and for 0.25 µg/mL (c3) the analysis revealed the highest area under curve (AUC), 0.80 (0.64-0.96), P<0.01 (Fig. 1). P<0.005 on ROC curves means that AUC is different of 0.5 and that variable is involved actually in the process.
When all dipyrone concentrations are used, considering the highest SI from all three dipyrone concentrations (per patient and control), ROC curve analysis yields a higher AUC of 0.82 (0.66-0.96), P<0.01. The optimal SI (threshold for BAT dipyrone positivity), corresponding to the best sensitivity and specificity, from ROC performed with the highest SI from the three dipyrone concentrations (per patient and control) is 1.71(Fig. 2).
Considering this 1.71 SI value as the threshold for positivity and a percentage of activated basophils of more than 5%, for c1 there were 7 BAT positive patients, for c2 there were 9 patients and for c3 concentration there were 10 BAT positive patients. Six patients were BAT positive for all the three dipyrone concentrations. Thirteen patients had a positive BAT for at least one of the tested dipyrone concentrations (65%). All of the healthy controls presented negative BAT (Table 1).
BAT sensitivity for the c1, c2 and c3 dipyrone concentrations and BAT sensitivity for all the three concentrations used together obtained from ROCs were higher than BAT sensitivity defined as the number of patients with BAT positive results/total number of patients, where BAT was considered positive if SI was higher than the threshold (SI>1.71) and the percentage of activated basophils was above 5% (Table 2).
When flowcytometry was performed for the 14 patients tested within one year after the allergic reaction (Δt<1 year), there were 10 BAT positive results (72%). For the 6 patients tested after one year (Δt>1 year), there were 3 BAT positive results (50%). The percentage of positive BAT results was higher when the patients were tested within one year after the allergic reaction.
DISCUSSION
The performance of the BAT, which measures the cellular reactivity after stimulation with the allergen, is closely related to the drug concentration and the chosen threshold for positivity.
In our study, we assessed the reliability of flow cytometry in the diagnosis of anaphylaxis to dipyrone, evaluating its sensitivity and specificity at an optimal given threshold, which is the SI. As the golden standard for the diagnosis of dipyrone anaphylaxis, the drug challenge test, is potentially dangerous, at present, skin testing remains the reference test for detection of IgE-specific allergies and skin testing coupled with history remain the mainstay of the diagnosis of an IgE-mediated reactions.22,23 Specific allergic reactions to dipyrone are likely to be associated with IgEs and skin tests unravel IgE-mediated anaphylaxis.24,25 BAT is well applicable in cases of IgE-mediated immediate-type hypersensitivity.10 In our study we included a well characterised group of patients with a positive history of anaphylaxis to dipyrone and positive skin tests, as well as dipyrone-tolerant healthy controls with negative skin tests and negative dipyrone challenge tests.
Optimized drug-specific decision thresholds can be calculated through inclusion of allergic patients and exposed control individuals, those with and without the disease.26,27 In the past, thresholds for positivity were set arbitrarily, but have been replaced by ROC curves which improve the diagnostic accuracy of tests by applying drug-specific cut-offs instead.10,26
The design of the studies assessing the sensitivity and specificity of BAT for dipyrone varied from one to another, from variable inclusion criteria, to different skin testing protocols and different BAT techniques. BAT was performed for dipyrone dilutions of 0.25 mg/mL and 2.5 mg/mL8 or dilutions of 0.625 mg/mL and 5 mg/mL9,14 BAT results were considered as being positive when at least one stimulation index was above 2.8,14 Sensitivity ranged from 15%14 to 85.7%.8 One of the studies reported 100% specificity.9 These major differences render the results of the tests incomparable and highlight the need for standardised decision thresholds and the use of optimal drug concentrations.
Recently, NSAIDs-induced basophil activation was reported to occur in vitro in both clinically hypersensitive patients and apparently healthy controls, as anti-inflammatory compounds can interact pharmacologically with basophils and induce non-specific histamine release in controls.8,15 Basophil activation by NSAIDs occurs in a dose-dependent manner. Hypersensitive patients seem to react to lower NSAIDs concentrations. Thus, BAT might discriminate allergic patients from healthy individuals when used at lower concentrations, therefore we chose concentrations three log scales lower than in previous studies (25 µg/mL, 2.5 µg/mL and 0.25 µg/mL). The result of the test depends on the concentration of the drugs and a wide concentration range, spanning several log scales, is advised in order to establish the optimal stimulation concentration.26
The assumption that one single allergen concentration is not sufficient to analyse basophil responses was based on the experience with histamine release tests, but not on the experience with CD63 expression.28 The opportunity to restrict basophil activation experiments to an "optimal" concentration that discriminates between patients and controls was thought to be possible for drugs.29 In our study, the diagnosis of dipyrone allergy in patients with anaphylaxis and positive skin tests was confirmed for 7 patients for c1 dipyrone concentration, for 9 patients for c2 and for 10 patients for c3 dipyrone concentrations. When all three dipyrone concentrations are considered, there are 13 BAT positive patients, thus BAT detects a larger number of cases when all the three dipyrone concentrations are used together. One should not use a threshold concentration but three concentrations to maximize sensitivity.
Moreover, the cut-off for positivity must be established by the assessment of the optimal values of sensitivity and specificity for each allergen by means of ROC curves.25,28 In our study, the optimal threshold calculated by ROC for all the three concentrations is a stimulation index of 1.71. By lowering the cut-off value for drugs sensitivity increases avoiding false negative results which might have dramatic consequences.26 The threshold of 1.71 gives 70% sensitivity and 100% specificity from ROC performed with all three dipyrone concentrations together. Thus, the best methodological approach is to test each patient for all three dipyrone concentrations in BAT.
In conclusion, in our study BAT detects a larger number of positive patients when all the three low dipyrone concentrations are used together. With an assay-specific threshold of 1.71, ROC curve analysis yields 70% sensitivity and 100% specificity.


 XML Download
XML Download