

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asymptomatic phenotypes of asthma are frequently found in patients with rhinitis.1-3 Nonspecific airway hyperresponsiveness (AHR) in patients with rhinitis, regardless of atopy status, has been proposed as a risk factor of asthma development,4,5 and has been a topic of considerable investigation. However, lower airway eosinophilic inflammation in patients with rhinitis, as reflected by increased eosinophil counts in bronchial biopsy tissues, bronchoalveolar lavage fluid, or hypertonic saline-induced sputum samples, has garnered far less attention.
Eosinophils are known to play an important role in allergic diseases.6 In patients with non-asthmatic allergic rhinitis, sputum eosinophilia is related to nonspecific AHR, but is insufficient to cause symptoms of asthma.7,8 In asthma, elevated numbers of eosinophils in the lower airway correlate with asthma severity. Major basic protein (MBP) is one of the major granule proteins of eosinophils and is known to mediate AHR. Eosinophils also secrete cysteinyl leukotrienes that may lead to increased vascular permeability, mucus secretion, and smooth muscle constriction.6 However, there is no direct evidence causally linking eosinophils or their products to AHR in clinical asthma. Research has instead focused on the possible role of lower airway eosinophilic inflammation on repair and remodeling in asthmatic airways.6 In addition, eosinophils are reportedly related to irreversible airflow obstruction in recurrent eosinophilic bronchitis, which is also present with lower airway eosinophilic inflammation but without AHR.9,10
Eosinophils have been found to be the source of several fibrosis-related mediators, such as transforming growth factor-β (TGF-β) and matrix metalloproteinase-9 (MMP-9) in asthmatic airways.6 TGF-β is involved in many aspects of airway remodeling in asthma, including epithelial changes and subepithelial fibrosis.11 MMP-9 and tissue inhibitor of MMPs-1 (TIMP-1) are important enzymes involved in airway remodeling in asthma. In particular, an aberrant MMP-9-TIMP-1 ratio has been suggested to contribute to airway remodeling in asthma by perturbing the balance between extracellular matrix destruction and repair.12
A number of techniques can be used to assess inflammation and the expression of mediators in the airway.13 Direct methods require biopsy samples, which implies a risk of bleeding; indirect methods, such as bronchoalveolar lavage and hypertonic saline-induced sputum examinations, are more convenient and relatively free of such risks.13 Moreover, fibrosis-related cytokines and mediators in airway diseases can be measured in induced sputum samples at the protein and mRNA levels.13,14
The present study was designed to evaluate the clinical significance of lower airway eosinophilic inflammation measured by sputum eosinophilia in patients with rhinitis without AHR. In addition, we investigated the sputum mRNA levels of fibrosis-related mediators such as MMP-9, TIMP-1, and TGF-β.
MATERIALS AND METHODS
Study subjects
Data were collected from 89 consecutive patients with moderate-to-severe perennial rhinitis without AHR who visited Seoul National University Hospital (SNUH) between 1 January 2005 and 1 January 2007. Rhinitis severity was classified according to the guidelines proposed by the Allergic Rhinitis and its Impact on Asthma (ARIA) workshop group.15 Lower airway symptoms such as wheezing, dyspnea, and cough were documented at the first visit.
Skin prick tests or multiple allergen screening tests (MAST) (RIDA® Allergy screen kit; R-Biopharm, Darmstadt, Germany), lung function tests, methacholine bronchial provocation tests, hypertonic saline-induced sputum examinations, chest X-rays, and serum total IgE levels were investigated. The presence of nasal polyps was determined by nasal cavity examination using a nasal speculum, flexible rhinoscopy, or computed tomography. Radiologic findings and chest X-ray images were reviewed to confirm the absence of a destructive lung lesion.
Patients taking systemic steroids at initial presentation were excluded. Subjects with lower-airway symptoms at presentation, destructive lung diseases (e.g., chronic obstructive lung disease, idiopathic pulmonary fibrosis, or sequelae of pulmonary tuberculosis), or a positive methacholine bronchial provocation test result were also excluded.
Allergologic work-up
All patients discontinued their medications, including systemic and intranasal corticosteroids and antihistamines, at least 1 week prior to allergologic work-ups. Skin prick tests for 55 common inhalant allergens included Dermatophagoides pteronyssinus, D. farinae, cat fur, dog fur, Aspergillus, Alternaria, tree pollen, grass pollen, mugwort, ragweed, and cockroach (Allergopharma, Reinbek, Germany), and were performed as described previously.16 Atopy was regarded as the presence of at least one positive skin prick test or MAST result. The methacholine bronchial provocation test was performed as described previously.16 In short, 0.25, 1, 4, and 16 mg/mL methacholine were prepared by dilution with normal saline. The five-breath dosimeter protocol using a DeVilbiss 646 nebulizer (DeVilbiss Healthcare, CA, USA) controlled by a KoKo dosimeter (Pulmonary Data Service Instrumentation Inc., Louisville, CO, USA) was used. Subjects inhaled five inspiratory capacity breaths of increasing methacholine concentrations either until the forced expiratory volume in 1 second (FEV1) fell to <80% of its baseline value or until the highest concentration was reached. Methacholine AHR was expressed as the provocative concentration of methacholine causing a 20% fall in FEV1 (PC20) and was regarded as positive if the PC20 was <16 mg/mL. FEV1 and forced vital capacity (FVC) were measured using the PO Box 6 (MicroMedical Limited, Rochester, England) and WinDx (version 1.0.51, Creative Biomedics, San Clemente, CA, USA) software, and FEV1/FVC ratios were calculated. FEV1 and FVC values are expressed as the predicted percentage of each parameter throughout the manuscript. Sputum eosinophilia was regarded as positive when the percent of sputum eosinophils relative to all nucleated cells (other than squamous epithelial cells) was ≥3%. Subjects were divided into two groups according to their sputum eosinophilia status (eosinophilia-positive [EP] group if sputum eosinophils were ≥3% and eosinophilia-negative [EN] group if sputum eosinophils were <3%). Serum total IgE levels were measured using radioimmunoassay kits (Packard, Meriden, CT, USA).
Sputum induction, processing, and RNA extraction
Sputum samples were obtained as described previously.16 After measuring basal FEV1, all subjects were administered 200 µg of inhaled salbutamol (Ventolin™; GlaxoSmithKleine, Brentford, UK). An ultrasonic nebulizer (Omron Co., Tokyo, Japan) was used to administer 4.5% saline at an output of 4.5 mL/minute for 5 minutes, up to four times. After each saline administration, subjects were asked to rinse their mouths and were encouraged to expectorate into a sterile Petri dish. Samples were treated with a 4% solution of the mucolytic agent dithiothreitol. Total cell counts were determined using a hemocytometer, and cell concentrations adjusted to 1.0×106 cells/mL. Cytospins were prepared by adding 60 µL of these cell suspensions to Shandon II cytocentrifuge cups (Shandon Southern Instruments, Sewickley, PA, USA) and spinning for 5 minutes at 500 rpm. Slides were stained with Diff Quik solution (Sysmex Co., Kobe, Japan) to determine differential cell counts for leukocytes, bronchial epithelial cells, and squamous cells. Samples were discarded if there were ≥20% squamous cells.
In addition, sputum samples were mixed with 1 mL of TRIzol (Gibco, Carlsbad, CA) and stored at -80℃ until required for mRNA extraction, which was performed according to the manufacturer's instructions (Gibco, Carlsbad, CA, USA). RNA was quantified by measuring optical density (OD) at 260 nm with a NanoDrop ND-1000 spectrophotometer (NanoDrop Technologies, Wilmington, DE, USA). The RNA obtained was stored at -80℃ until required for reverse transcriptase-polymerase chain reaction (RT-PCR).
Reverse transcriptase-polymerase chain reaction
Sixty-two sputum samples were available for RT-PCR (20 in the EP group and 42 in the EN group). Two micrograms of total RNA were used to synthesize first-strand cDNA from oligo-dT-primed RNA using reverse transcriptase (Promega, Madison, WI, USA). In brief, total RNA mixtures were incubated with 200 UM-MLV reverse transcriptase, 20 U RNasin, 0.5 mM dNTPs, 25 µg/mL primer dT, 50 mM Tris-HCI (pH 8.3), 75 mM KCI, and 3 mM MgCl2 in a final volume of 50 µL for 60 minutes at 42℃. The cDNA products were stored at -20℃ for subsequent amplification by PCR. PCR reaction mixtures for glyceraldehyde-3-phosphate dehydrogenase (GAPDH), TGF-β, MMP-9, and TIMP-1 contained 2 µL of sample, 0.5 mM dNTP, 0.5 U Taq polymerase, 1 µg of each primer, 50 mM Tris-HCI, 3 mM MgCl2, and 75 mM KCl 0.01% gelatin in a final volume of 100 µL. PCR was performed on a thermal cycler (Personal Cycler Biometra, Germany). Reaction conditions for GAPDH were 95℃/30 seconds, 58℃/30 seconds, and 72℃/30 seconds for 30 cycles, followed by a 5-minute extension at 72℃; those for TGF-β PCR were 95℃/30 seconds, 60℃/30 seconds, and 72℃/30 seconds for 35 cycles, followed by a 5-minute extension at 72℃; and those for MMP-9 and TIMP-1 were 95℃/30 seconds, 60℃/30 seconds, and 72℃/30 seconds, followed by a 5-minute extension at 72℃. Primer sequences for the internal control (GAPDH) were 5'-GAA TTC GCC AGC CGA GCC ACA TCG C-3' for the downstream primer and 5'-CTC GAG GAC GAA CAT GGG GGC ATC AGC-3' for the upstream primer. Primer sequences for TGF-β were 5'-TTT CGC CTT AGC GCC CAC TG-3' for the 5' primer and 5'-TCC AGC CGA GGT CCT TGC GG-3' for the 3' primer. For MMP-9, primer sequences were 5'-ATC CAG TTT GGT GTC GCG GAG C-3' for the 5' primer and 5'-GAA GGG GAA GAC GCA CAG CT-3' for the 3' primer. For TIMP-1, primer sequences were 5'-CTG TTG TTG CTG TGG CTG AT-3' for the 5' primer and 5'-TCC GTC CAC AAG CAA TGA GT-3' for the 3' primer. Amplifications resulted in products of 200-600 bp, as determined by electrophoresis in a 2% TAE agarose gel containing ethidium bromide. Protein concentrations were measured using the Bio1D image analysis software. All results were normalized vs. GAPDH to compensate for variation in cDNA loading.
Statistical analysis
Data were analyzed using SPSS version 12.0 (SPSS Inc., Chicago, IL, USA). The t-test or Mann-Whitney's U test were used to compare the two groups with respect to continuous variables, and the chi-square test was used for categorical variables. The relationship between sputum eosinophil counts and FEV1 was assessed using Pearson's correlation test. P values of <0.05 were regarded as indicative of statistical significance. Data are presented as means and standard deviations. The study protocol was approved by the Seoul National University Hospital Institutional Review Board.
RESULTS
Based on sputum eosinophil results, the 89 patients were divided into two groups: the EP group members had sputum eosinophils at ≥3% of total nucleated cells (n=28), and the EN group had sputum eosinophils at <3% (n=61). Clinical characteristics of each group are shown in Table 1. No significant difference was found between the two groups in terms of sex, age, atopy, duration of illness, or total IgE.
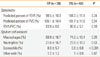
Relationship between sputum eosinophil counts and lung function
With the exception of eosinophils, no significant difference in differential cell counts in hypertonic saline-induced sputum between the two groups was observed. FEV1 was significantly lower (98.5%±10.3% for EP vs. 104.0%±11.9% for EN groups, P=0.04) and FEV1/FVC tended to be lower (83.9%±8.6% for EP vs. 86.9%±5.1% for EN groups, P=0.1) in the EP group. No difference in FVC was observed between the two groups (Table 2). Sputum eosinophil counts were negatively correlated with FEV1 (β=-0.62, P=0.02) and FEV1/FVC (β=-0.41, P=0.005), but not with FVC (β=-0.11, P=0.66) (Fig. 1).
Sputum fibrosis-related mediator mRNA levels
mRNA transcript levels were examined in 62 of the 89 sputum samples (20 in the EP group and 42 in the EN group). MMP-9 mRNA expression was significantly higher in the EP group (0.8±0.6 for EP and 0.4±0.3 for EN, p=0.005) (Fig. 2A), whereas TIMP-1 mRNA levels were similar between the two groups (1.1±1.0 for EP and 1.2±1.1 for EN, P=0.65). In addition, the MMP-9/TIMP-1 mRNA ratio was significantly higher in the EP group (1.2±1.0 for EP and 0.6±0.6 for EN, P=0.01) (Fig. 2B). There was no significant difference in the TGF-β mRNA level.
DISCUSSION
We found that sputum eosinophil counts were negatively correlated with FEV1 and FEV1/FVC in non-asthmatic patients with moderate-to-severe perennial rhinitis. In addition, subjects with sputum eosinophilia showed higher MMP-9 mRNA levels and MMP-9/TIMP-1 mRNA ratios in hypertonic saline-induced sputum than those in patients without sputum eosinophilia.
The study population included those who had moderate-to-severe perennial rhinitis without lower respiratory symptoms such as cough, sputum, wheezing, and dyspnea. Thus, the diagnosis of these patients was rhinitis not accompanied by asthma or eosinophilic bronchitis. Sputum eosinophilia as well as AHR in patients with rhinitis is not an uncommon finding in both allergic7,17 and non-allergic18 rhinitis without asthmatic symptoms. Although sputum eosinophilia showed a strong relationship with airway hyperresponsiveness measured by methacholine or adenosine in patients with non-asthmatic rhinitis, cases of sputum eosinophilia in the absence of AHR have been reported.7,17,18 To investigate the role of lower-airway eosinophilic inflammation in rhinitis separately from AHR, we excluded patients with rhinitis who showed a positive methacholine bronchial provocation test.
Patients with non-asthmatic rhinitis with sputum eosinophilia showed a significantly lower FEV1 and FEV1/FVC ratio than did those without sputum eosinophilia in our study. This finding is consistent with previous reports, which found reduced lung functions in some patients with perennial rhinitis.17 In previous studies, forced expiratory flow at 25% to 75% of vital capacity (FEF25-75%) was found to be impaired mainly in patients with allergic rhinitis without symptoms of asthma. FEF25-75% was thought to change earlier than FEV1 in the development of asthma.19,20 However, recent studies demonstrated that FEV1 could also be reduced along with FEF25-75% in patients with rhinitis without symptoms of asthma, and that these findings were related to AHR.19,20 In the present study, we measured only FEV1 values and not FEF25-75%. However, after controlling for the possible influences of AHR, differences in FEV1 values between the EP and EN groups were noted, which may have been due to the presence of lower-airway eosinophilic inflammation. The influence of lower-airway eosinophilic inflammation on airflow limitation has been investigated in patients with eosinophilic bronchitis, and patients with recurrent eosinophilic bronchitis developed progressive airflow limitation.10,21,22 The mechanism underlying the influence of eosinophils on lung function is not known; however, bronchial biopsies of patients with eosinophilic bronchitis showed structural changes similar to the airway remodeling in asthmatic patients.23 The presence of lower-airway remodeling in non-asthmatic AHR was identified by bronchial biopsy.24 Together, those findings support the idea that lower-airway eosinophilic inflammation in patients with non-asthmatic rhinitis may influence lung function.
We found that MMP-9 mRNA levels and MMP-9/TIMP-1 ratios were significantly higher in patients with non-asthmatic rhinitis with sputum eosinophilia than in those without sputum eosinophilia. MMP-9 is the predominant matrix metalloproteinase in the lung and is believed to play an important role in airway remodeling by degrading the extracellular matrix, modulating epithelial repair, and controlling the activities of cytokines and chemokines.25 MMP-9 levels were frequently found to be elevated in asthmatic subjects, and to increase significantly during acute asthma attacks and after allergen challenges.26 TIMP-1 is a well-known counterpart of MMP-9, and imbalances in MMP-9 and TIMP-1 expression are believed to be important for airway remodeling.25,26 Because we did not determine the mRNA levels of MMP-9 and TIMP-1 in a normal control population, we were unable to determine whether the values were elevated or decreased compared with normal controls. Also, we were unable to investigate the functional implications of the different MMP-9 and TIMP-1 expression patterns in the airways of patients. However, we did identify different patterns of expression of these enzymes between the EP and EN groups.
Because of the retrospective design of this study, it had several limitations. First, the subject population was heterogeneous: some had allergic rhinitis while others had non-allergic rhinitis. The inclusion criteria were highly specific, and we were unable to source sufficient patients with each rhinitis subtype. In particular, we were unable to characterize non-allergic rhinitis subtypes, such as atrophic rhinitis, idiopathic rhinitis, and non-allergic rhinitis with eosinophilia syndrome, because nasal smears for eosinophils, nasal secretion analysis of specific IgE, and nasal allergen provocation tests were not performed. Second, we could not determine whether the differences in the expression of fibrosis-related mediators had any clinical implications. We found significant differences in FEV1 between the EP and EN groups. However, we could not assess whether the airflow limitation in the EP group was due to reversible factors or irreversible structural changes, which could be determined by computed tomography or bronchial biopsy. Third, the EN group contained more intranasal corticosteroid users than the EP group, although the difference was not statistically significant. Because the use of intranasal corticosteroids can influence AHR,27 patients with mild AHR might have been included in the EN group by chance. In addition, intranasal corticosteroids may have directly influenced sputum eosinophil counts and mediator expression. In this study, patients were educated not to use intranasal corticosteroids for at least 1 week before inducing sputum. No data on the proper abstinence period to exclude the effects of intranasal corticosteroids on sputum cells and mediators are available, though previous studies found intranasal corticosteroids to have little or no influence on sputum eosinophil counts.28,29 In asthmatic users of inhaled corticosteroids, the sputum eosinophil counts returned to baseline within 2 weeks after withdrawal of inhaled corticosteroids.30 Inhaled steroid did not affect MMP-9 and TIMP-1 expression in mild asthma31 and TGF-β expression did not decrease after treatment with oral corticosteroid in moderate-to-severe asthma.32 Therefore, we believed that withdrawal of intranasal corticosteroids 1 week before sputum induction would be sufficient to remove their influence on sputum eosinophils and mediator expression. Fourth, airway responsiveness to adenosine was reported to be more closely related to the extent of sputum eosinophilia than to methacholine.7 In our study, we were unable to evaluate airway responsiveness to adenosine. Thus, it is possible that some subjects had AHR to adenosine. Finally, we could not evaluate sputum mRNA levels in all patients, as only 62 samples were suitable for the procedure. We also were unable to determine actual protein levels of the fibrosis-related mediators due to use of mucolytics in sputum sample processing.
In conclusion, sputum eosinophilia in patients with moderate-to-severe perennial rhinitis without AHR influenced FEV1 and the expression pattern of fibrosis-related mediators.




 XML Download
XML Download