

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is an increasingly common health problem in adults and children.1,2 The prevalence of asthma has increased every year for the last five decades.3-5 A Korean survey showed that 8.9% of the population has been diagnosed with asthma.6 Further, the prevalence of asthma in Korea has increased from 5.7% in 1980 to 10.1% in 1990.6
Genetic (cytokine and immune response genes),7,8 developmental, and environmental factors such as viral infections,9 allergens,10 and occupational exposure11 have been associated with asthma susceptibility, age at onset, and severity. Although the pathogenesis of the disease has not been fully elucidated, a major risk factor is the development of an immune response to a foreign antigen that is characterized by the production of antigen-specific immunoglobulin E (IgE).12 IgE-mediated allergic reactions to environmental allergens play an important role in the pathophysiology of asthma. Atopic persons have high levels of IgE that is reactive against one or more specific allergens and they often have increased plasma total IgE concentrations.13 Moreover, the prevalence of asthma is closely related to serum IgE levels standardized for age and sex.14 Overwhelming evidence has confirmed the role of IgE in atopic asthma, while a link between IgE and non-atopic asthma has also been reported.15
Several studies have reported a strong relationship between exposure to house dust mites, the presence of serum IgE directed against mite allergens, and asthma.16-18 Epidemiological evidence indicates that atopic asthma is correlated with a high serum IgE level, although the contribution of allergen-specific IgE antibodies to the pathogenesis and severity of this disease is unclear. In the present study, we examined the prevalence of atopy and compared clinical characteristics and the presence of airway inflammation by atopy in the Cohort for Reality and Evolution of Adult Asthma in Korea (COREA) cohort asthmatics.
MATERIALS AND METHODS
Subjects
The Corea is an eight-year (2005-2012), multicenter, prospective cohort study of asthmatics 19 years of age or older.19
Patients were enrolled at 11 clinical centers in various regions of South Korea. The participating institutions were the Asan Medical Center at the University of Ulsan and the hospitals of Seoul National University, Bundang Seoul National University, Yonsei University, Chung-Ang University, Ewha Womans University, Hanyang University, Soonchunhyang University, Ajou University, The Catholic University of Korea, and Chonbuk National University. We retrospectively studied the clinical data of 2,588 asthma patients who were registered in the COREA cohort. Asthma was diagnosed based on GINA guidelines.20 All subjects had a clinical diagnosis of asthma that was supported by one or more of the following criteria: 1) variability in the maximum diurnal peak expiratory flow of >20% over the course of 14 days, 2) an increase in FEV1 of >15% after the inhalation of 200-400 µg of albuterol, or 3) a 20% reduction in FEV1 in response to a provocative concentration of inhaled methacholine (PC20) of <25 mg/mL. Asthma control status and allergic rhinitis severity were classified to GINA guideline20 and ARIA guideline.21 The subjects underwent a standardized assessment, including an analysis of induced-sputum specimens, complete blood cell counts with differential counts, IgE concentrations, chest posteroanterior radiography, allergy skin prick tests, and spirometry. The body mass index (BMI) for each patient was calculated as weight (kg)/height (m2).22,23
The exclusion criteria were respiratory infection, COPD, vocal cord dysfunction, obstructive sleep apnea, Churg-Strauss synsyndrome, cardiac dysfunction, allergic bronchopulmonary aspergillosis, and poor adherence to treatment. All subjects were ethnic Koreans and required to provide written informed consent. The research protocol for this cohort study was approved by the Institutional Review Board (IRB) of each center.
Lung function
During a baseline visit, information regarding demographic characteristics was collected from all subjects, and spirometry was performed before and after the use of a bronchodilator. Baseline FVC and FEV1 measurements were obtained in the absence of recent bronchodilator use (within 8 hours). The basal and post-bronchodilator FEV1, FVC, forced expiratory flow between 25 and 75% FVC (FEF25-75%), and DLCO were measured. FVC and FEV1 were measured at regular intervals of one or two months. We used Vmax Series 2130 Autobox Spirometry (Sensor Medics, Yorba Linda, CA, USA) and applied a calibration check every morning at 8:00 AM.
Allergy skin tests
Common inhalant allergens, including dust mites (Dermatophagoides farinae and Dermatophagoides pteronyssinus), Cat fur, Dog fur, Cockroache, Grass, Tree pollen (mixed), Ragweed, Mugwort, Alternaria, and Aspergillus spp. (Bencard Co., Brentford, UK) were used for the skin prick test.24 Atopy was defined as having an allergen-induced wheal reaction equal to or greater than that caused by histamine (1 mg/mL) or equal to or greater than 3 mm in diameter. Total IgE was measured using the UniCAP system (Pharmacia Diagnostics, Uppsala, Sweden).
Sputum examination
Sputum samples were obtained for differential cell counts for patients in a stable state. Sputum was induced using isotonic saline containing a short-acting bronchodilator, and the samples were treated within 2 hours of collection as described previously.25 Briefly, all visible portions with greater solidity were carefully selected and placed in a pre-weighed Eppendorf tube. The samples were treated by adding eight volumes of 0.05% dithiothreitol (Sputolysin; Calbiochem Corp., San Diego, CA, USA) in Dulbecco's phosphate-buffered saline (PBS). One volume of protease inhibitor (0.1 M EDTA and 2 mg/mL phenylmethylsulfonylfluoride) was added to 100 volumes of the homogenized sputum, and the total cell count was determined with a hemocytometer. The cells of the homogenized sputum were collected by cytocentrifugation, and 500 cells were examined on each sputum slide after staining with Diff-Quick (American Scientific Products, Chicago, IL, USA).
Statistical analysis
The data were double-entered into a statistical software package (SPSS, version 14.0; SPSS Inc., Chicago, IL, USA). The data are expressed as the mean±standard deviation (SD) or standard error of the mean (SEM). Group differences in atopy were compared using a two-sample t-test, Mann-Whitney test, or Pearson's χ2 test for normally distributed, skewed, or categorical data, respectively. Differences in the proportions of the patient populations were analyzed by the χ2 test with Fisher's exact test when low expected cell counts were encountered. A P value<0.05 was considered to be statistically significant.
RESULTS
Common inhalant allergen sensitization
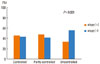
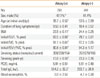
House dust mites (D. farinae and D. pteronyssinus) were the most prevalent allergen on the skin prick test (Fig. 1). The percentage of atopic patients with sensitization to two or more allergens was 39.3%. Total IgE levels were higher in atopic asthmatics than in non-atopic asthmatics (514.2±32.2 vs. 293.7±26.9 ku/L, P=0.001, Table 1).
Relationship between atopy and clinical variables
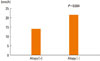
BMI was lower in atopic asthmatics than in non-atopic asthmatics (23.5±0.11 vs. 24.4±0.25 kg/m2, P=0.001). Although the allergen sensitization number was correlated with the total IgE level (r=0.351, P=0.001) and total IgE was correlated with asthma severity (r=0.101, P=0.005), allergen sensitization was negatively correlated with asthma severity (r=-0.102, P=0.001). As compared with non-atopic asthmatics, atopic asthmatics showed early onset of the disease (30.2±0.45 vs. 43.1±0.65 years, P<0.05). Cigarette smoking (in pack years) was higher in the non-atopic asthmatics than in the atopic asthmatics (23.3±0.76 vs. 13.8±0.59, P=0.001). The erythrocyte sedimentation rate (ESR) was higher in the non-atopic asthmatics than in the atopic asthmatics (20.1±2.68 vs. 12.5±1.03 mm/hr, P=0.004, Fig. 2).
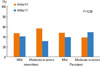
Relationship between atopy and severity of asthma and allergic rhinitis
Atopic patients with asthma had a higher FEV1 (83.5±0.68 vs. 79.7±0.81% predicted, P=0.001), FVC (91.1±0.61 vs. 87.2±0.65% predicted, P=0.001), and FEV1/FVC (90.8±0.81 vs. 84.3±1.17%, P=0.001) as compared with non-atopic patients with asthma. Asthmatics without atopy had more uncontrolled asthma (control status [n=atopy/non-atopy], controlled=185/177 vs. partly controlled=326/289 vs. uncontrolled=127/200, P=0.001, Fig. 3) and severe rhinitis as compared with atopic asthmatics (severity [n=atopy/non-atopy], mild intermittent=99/87 vs. moderate to severe intermittent=59/35 vs. mild persistent=232/197 vs. moderate to severe persistent=68/83, P<0.05, Fig. 4).
Relationship between atopy and sputum inflammatory cells in patients with asthma
The atopic patients with asthma had a higher percentage of sputum lymphocytes (4.46±1.49 vs. 2.44±0.47%, P=0.001) than the non-atopic patients with asthma, and those patients with non-atopic asthma had a higher percentage of sputum neutrophils (36.0±2.28 vs. 25.3±2.02%, P=0.001) than those with atopic asthma (Table 2). There were no differences in PC20 and blood eosinophils counts between the two groups.
DISCUSSION
The results of this study suggest that atopy is associated with the severity of adult asthma and rhinitis, independent of airway hyperresponsiveness.
Asthmatics are typically classified as atopic or non-atopic based on sensitization to environmental aeroallergens. However, atopic and non-atopic asthma are not well-separated disease entities.26 Although atopy is clearly a risk factor for the development of asthma, only a small subset of subjects sensitized to aeroallergens express persistent symptoms, suggesting that additional pathogenic mechanisms such as respiratory viral infections are involved as cofactors.27 In this study, house dust mites were the most prevalent allergen and atopy was related with the severity of asthma and allergic rhinitis in the COREA cohort. These results are consistent with the notion that the quantification of IgE antibodies may serve as a marker of asthma severity.22 In this study, although allergen sensitization was correlated with total IgE levels and total IgE was correlated with asthma severity, the allergen sensitization number was negatively correlated with asthma severity, indicating that not only IgE antibody levels, but also the number of allergens reacting positively when tested, are involved in asthma severity.23 In this study, the atopic asthmatics showed early disease onset and high IgE levels, indicating a role for allergen-specific IgE antibodies in the pathogenesis of asthma and suggesting preventive and therapeutic measures for asthma control.
Asthma and allergies in developing countries may be associated with the adoption of an urbanized "Western" lifestyle. Total caloric intake is increasing with the industrialization of Korea, and BMI has been shown to be associated with wheezing in older adults living in rural areas of Korea.28 General obesity and central obesity are potential risk factors for asthma in relatively non-obese Korean adults.29 Further, BMI has been shown to be associated with airway hyperresponsiveness in school-age boys. In this study, the BMI was lower in atopic asthmatics than in non-atopic asthmatics. In addition, the non-atopic asthmatics were older and most were not obese, suggesting that Korean adult asthmatics are relatively non-obese.
Limited data regarding systemic inflammatory markers exist with respect to asthma. Some studies reported that systemic inflammatory markers were elevated in patients with non-allergic asthma and obese patients with asthma.30
Measured systemic inflammation markers, including C-reactive protein (CRP), total leukocyte count, and ESR were higher in patients with asthma and reduced by inhaled steroids plus an inhaled β2 agonist.31 One study showed that CRP was higher in patients with non-allergic asthma than in patients with allergic asthma or healthy controls.32 Another study investigated the role of obesity in local and systemic inflammation in patients with asthma.33 In this study, although the number of white blood cells did not differ between the atopic and non-atopic asthmatics, the ESR was higher in non-atopic asthmatics than in atopic asthmatics, indicating that systemic inflammation is involved in non-atopic asthma.
Cigarette smoking and asthma are associated with poor symptom control and impaired therapeutic responses to anti-asthma drugs.34 In the developed world, approximately 25% of the population smokes cigarettes35,36 and an additional 25% are former smokers. Smoking rates are similar amongst adults with asthma.37-39 Higher levels are seen in patients with asthma that present to emergency departments with exacerbations.39 As compared with nonsmokers with asthma, those who smoke have worse symptom control,37,38 an accelerated decline in lung function,40,41 and an increased mortality rate.42 Asthmatic smokers have more severe symptoms,36,37 a greater need for rescue medication,43 and worse health status indices as compared with never-smokers.43,44 In this study, non-atopic asthmatics had higher pack year values and more severe asthma, suggesting that smoking contributes to difficulties in controlling asthma.
Previous immunopathologic studies of patients with mild asthma that underwent bronchoscopic biopsy suggested that eosinophilic airway inflammation is a characteristic abnormality in both atopic and non-atopic asthma.45-47 However, other pathologic studies have suggested that neutrophils are present in higher quantities in the airways of patients with severe asthma than in the airways of patients with mild asthma or in normal control subjects.48-50 In this study, although small group of asthmatic patients of total patients were included, non-atopic asthmatics had high sputum neutrophil counts, suggesting that sputum inflammatory cell numbers can be used as a guide in the treatment of asthmatics, and that the pathology in non-atopic asthmatics is different from that in atopic asthmatics.
In conclusion, our study of a Korean cohort indicates that atopic asthmatics had an early onset of disease and high IgE levels, while non-atopic asthmatics had decreased lung function and a high sputum neutrophil count, suggesting that the treatment of asthma may be different by the atopic status of the patient.

 XML Download
XML Download