

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Levofloxacin is an L-isomer of ofloxacin that has been used to treat various infectious diseases.1 Common adverse reactions to levofloxacin include gastrointestinal problems, central nervous system disabilities, such as headache, dizziness, and insomnia, increased liver enzyme levels, QT prolongation, and skin rashes.2 Anaphylaxis is a lethal adverse event that can be caused by fluoroquinolones. It has been reported that 0.46 to 1.2 out of 100,000 individuals treated with fluoroquinolones develop anaphylaxis.3 Levofloxacin-induced anaphylaxis is rare, although there have been a few reported cases.3-5 Herein, we describe a case in which anaphylaxis was confirmed by a positive oral provocation reaction and increased serum tryptase levels.
CASE REPORT
A 58-year-old male was admitted with dyspnea. Fifteen days prior to admission, the patient had been hospitalized due to asthma exacerbations. The patient developed fever on the third day of hospitalization and was given 250 mg of levofloxacin orally. Two and a half hours later, the patient developed sudden dizziness and a skin rash, and his asthma worsened. He was treated without antibiotics and discharged with improved symptoms. However, 5 days after admittance to our hospital, his dyspnea worsened.
There were erythematous papules over the patient's entire body, and blisters were observed around his lips. The patient had visited a dermatology clinic 2 days prior. A biopsy had been performed on the patient's blisters and he was diagnosed with a herpes infection. Peripheral blood tests revealed a white blood cell count of 7,070/µL (6.0% eosinophils), a hemoglobin level of 15.5 g/dL, and a platelet count of 313,000/µL. Biochemistry tests returned the following results: AST, 146 U/L; ALT, 698 U/L; ALP, 233 U/L; gamma-GT, 868 U/L; total bilirubin, 3.1 mg/dL; and direct bilirubin level, 1.9 mg/dL. The patient's total serum immunoglobulin E (IgE) level was 150 U/mL. A chest X-ray and liver computed tomography (CT) did not reveal any abnormalities. All viral markers for hepatitis were negative. In addition, skin prick tests for 55 allergens were negative. A pulmonary function test (PFT) showed an FEV1/FVC of 59.1%, an FEV1 of 2.14 L (70%), and an FVC of 3.62 L (86%). The PC20 in a methacholine bronchial provocation test was 6.46 mg/mL.
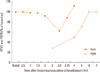
After the patient's dyspnea subsided, he was given 250 mg of levofloxacin at 10:00 AM and spirometry was performed every 30 minutes thereafter. The patient's peak expiratory flow rate (PEFR) was evaluated every hour beginning at 3 hours after oral provocation (Fig. 1). At 3.5 hours following oral provocation, a skin rash developed over the patient's entire body (Fig. 2) and he complained of dyspnea. At this time, the patient's FEV1 had decreased by 22% to 1.15 L. The patient inhaled salbutamol, and after 15 minutes his FEV1 was 1.62 L (53%). The patient complained of dizziness at 4 hours and 10 minutes after provocation; at this time, his blood pressure dropped to 67/45 mmHg. The patient was stabilized with shock positioning and a rapid saline drip. He was then given 10 mg of chlorpheniramine and 125 mg of methylprednisolone intravenously. We prepared the epinephrine before the provocation test, but mistakenly did not administer it. Two hours after the patient's blood pressure began to drop, his serum tryptase level was 17.7 µg/L (1.9-13.5 µg/L). There were no changes in PEFR during the first 13 hours and following 2 days.
DISCUSSION
Anaphylactic reactions can be classified as either IgE-mediated anaphylaxis or an IgE-independent anaphylactoid reaction.6 The presence of fluoroquinolone-specific IgE antibodies can be confirmed by radioimmunoassays. However, these assays are performed for research purposes only because it can be difficult to isolate antibodies and there is currently no standardized method available.7,8 One limitation of this report is the fact that neither a skin prick test nor serum analysis was performed. Because an IgE-mediated reaction was not excluded by a skin prick test or serum analysis, the patient was diagnosed with anaphylaxis.
To make an accurate diagnosis, additional testing methods, such as a skin prick test, intradermal test, or oral provocation test, must be utilized.9 The oral provocation test is currently the most accurate method. Although an exact mechanism has not been elucidated, studies suggest that the release of mediators such as histamine, which result from the high penetrability of fluoroquinolone into cells, plays an important role in the development of anaphylaxis.10 Thus, it has been suggested that skin prick and intradermal tests frequently produce false-positive results because fluoroquinolone can directly trigger the release of histamine.11
During an anaphylactic reaction, activated mast cells and basophils secrete histamine and tryptase. The finding of increased serum tryptase levels in patients suspected of having an anaphylactic reaction can be very useful.12 Histamine levels peak after 5 minutes and return to normal after 15-30 minutes. However, tryptase levels peak from 15-120 minutes after the onset of anaphylaxis and remain elevated for 6 hours. Therefore, these values can provide valuable diagnostic information in suspected cases of anaphylaxis.13,14 In the present case, the tryptase level became elevated 2 hours after the point at which the patient's blood pressure had decreased.
Previous studies have shown a correlation between drug allergies and viral infections.15 Fluoroquinolone administration is associated with patients infected with human immunodeficiency virus (HIV); according to Kelesidis et al.,10 10 of 22 ciprofloxacin-induced anaphylaxis patients were HIV-positive. These findings have been ascribed to the over-production of cytokines, including interferon-gamma, which expedite the activation of the immune system.16 In the present case, the patient had been diagnosed with a herpes infection following a blister biopsy. Herpes is known to be correlated with drug hypersensitivity syndrome.17 No studies have assessed the association between anaphylaxis and herpes infections; however, given that the patient in this report presented with both a herpes infection and anaphylaxis, future studies should be performed to evaluate this topic.

 XML Download
XML Download