

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic urticaria (CU) is a skin disorder characterized by the recurrent appearance of wheals and/or angioedema for more than 6 weeks.1,2 CU accounts for 25% of urticarial,2 and the prevalence of CU is 0.1%-0.6%.3,4 Almost 40% of CU patients continue to experience urticarial wheals 10 years later.5 CU has detrimental effects on the quality of life (QOL) and is associated with poorer general health and reduced emotional well-being;5-8 As a result, CU has a large impact on society in terms of healthcare costs.9,10 Patients with refractory CU do not respond to standard treatments with antihistamines or additional immunomodulators that are, in a few cases, unsafe when used for prolonged times.
CU is a heterogeneous disorder and includes idiopathic, autoimmune, and physical urticaria and vasculitis.11 For more than 50% of patients with CU, the underlying cause has not been identified.12 However, up to one-third of patients with chronic idiopathic urticaria have autoantibodies to FcεRI (a high-affinity receptor for IgE), and about 10% have IgE autoantibodies.13 These autoantibodies can cause mast cell degranulation, and most CU symptoms result from the degranulation of skin mast cells.
Omalizumab, a recombinant humanized monoclonal antibody, forms a biologically inert molecule with free IgE.14 Omalizumab selectively binds to the C3 domain of the IgE heavy chain, where IgE binds to FcεRI, and inhibits the reactions between anti-IgE and IgE-sensitized mast cells; thus, it can improve CU symptoms. Omalizumab was shown to be dramatically effective in chronic autoimmune urticaria,15 chronic idiopathic urticaria,16,17 and various urticaria subtypes such as cholinergic, cold, solar, and non-autoimmune urticarial, as well as CU with IgE autoantibodies against thyroperoxidase.18-22 In the present study, we evaluated the efficacy and safety of omalizumab, and observed the clinical course of omalizumab treatment in 26 patients with refractory CU.
MATERIALS AND METHODS
We conducted a retrospective study of patients who were treated with omalizumab for refractory CU. Patients with refractory CU were defined as having symptoms for at least 6 weeks with persistent hives, and not controlled most days of the week, despite the use of a fourth-line therapy for more than 4 weeks, according to EAACI/GALEN guidelines.19 Omalizumab was administered subcutaneously every 2 or 4 weeks for 24 weeks, dosed according to the patient's body weight and total serum IgE levels as described in previous studies.17,20 Atopy was defined as a positive skin prick test with at least one common aeroallergen or the presence of serum-specific IgE against at least one.
Urticaria activity score (UAS) and chronic urticaria-specific QOL (CU-QOL) questionnaires were completed every 4 weeks. The UAS (total score range, 0-15, with higher scores indicating higher disease activity) was measured using a combination of pruritus and four characteristics of wheals, including number, distribution range, mean diameter, and duration.21 The patient's health-related QOL was evaluated using a previously validated scoring system, the CU-QOL, comprising 17 items (total score range, 0-68, with higher scores indicating higher QOL).22 Medications were prescribed and stepped down with monitoring every 4 weeks following the EAACI/GALEN guidelines.19 In patients who achieved remission, the medications were stepped down. Drug requirements for antihistamines and steroids were calculated as described previously.23 Daily doses of H1-antihistamine drugs for the treatment of CU were calculated based on the equivalent dose of loratadine (10 mg/day), and the required antihistamine doses were calculated from the total antihistamine doses used for the control of CU during 4 weeks, presented as the equivalent dose (mg/week) of loratadine for the H1 antihistamine. Immunomodulators used included leukotriene receptor antagonists, cyclosporine, hydroxychloroquine, and colchicine.
The responses to omalizumab were described as follows: remission, defined as a condition with no symptoms and no requirement for medications for at least 4 weeks; responsive, defined as a step-down of more than one level of therapy compared with the baseline; and refractory, defined as neither remission nor any symptom improvement during the treatment period. The protocol for the study was approved by the Institutional Review Board of the hospital (AJIRB-MED-OBS-11-300).
Statistical analysis
Quantitative and qualitative results are expressed as the means±standard deviation (SD) and absolute numbers or frequencies, respectively. Descriptive statistics were performed using SPSS software ver. 12.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was assessed using the Mann-Whitney U test and Wilcoxon signed rank test for continuous variables and Fisher's exact test for categorical variables. Values of P<0.05 were considered to indicate statistical significance.
RESULTS
Patient characteristics
Twenty-six patients were enrolled in the present study. The mean age was 43.1±8.4 years, and 14 patients (53.8%) were men. The mean disease duration of CU was 63±72.7 months. Seventeen subjects (68%) had atopy, 16 (61.5%) had nonsteroidal anti-inflammatory drug (NSAID) hypersensitivity, and half of the subjects had angioedema or physical urticaria. Anti-nuclear antibody was detected in five patients (19.2%); antithyroglobulin antibody, in six patients (23.1%); and antimicrosomal antibody, in one patient (7.7%). The mean total IgE level was 247.7±274.6 kU/mL.
Changes in the UAS, CU-QOL, and medication requirements
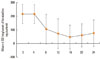
The UAS [12.11±1.97 to 3.0±4.28 at week 12 (P=0.001) and to 2.7±4.23 at week 24 (P=0.001)] decreased significantly, while the CU-QOL score [34.65±13.58 to 62.59±8.71 at week 12 (P=0.001) and to 60.88±11.11 at week 24 (P=0.004)] improved significantly during omalizumab treatment (Fig. 1). Eight of 11 subjects (72.7%, P=0.027) discontinued systemic steroid use, and 12 of 17 (70.6%, P=0.002) discontinued the use of any immunomodulator. The requirements for H1-antihistamines decreased significantly (215.66±70.06 to 60.85±70.53 mg/week of loratadine equivalents; P<0.001; Fig. 2).
Treatment outcomes
Twenty-two patients (84.6%) achieved remission during 24 weeks (remitted group). Ten patients achieved remission at week 4; four, at week 12; three, at weeks 8 and 16; and one, at weeks 20 and 24 (total mean, 9.27±6.1 weeks). In the remitted group, 14 (53.8%) maintained remission throughout the 24-week treatment period. However, symptoms recurred in eight (30.8%) of these subjects; the mean period for recurrence was 11 weeks (range, 4-20 weeks). Five (19.2%) maintained their baseline therapy, and the other three (11.6%) achieved step-down therapy. The causes of recurrence were alcohol (two cases), drugs (one case), coldness (two cases), and unknown causes (three cases). No significant differences were observed in clinical parameters, including age, gender, disease duration, atopy, angioedema, physical urticaria, and baseline UAS and CU-QOL score, or in medication schedules between the recurrent and remission maintenance groups. In the non-remitted group (n=4, 15.4%), two (7.7%) achieved step-down therapy and two (7.7%) were still refractory to omalizumab. One refractory patient had atopy and a history of NSAID hypersensitivity, and the other had atopic dermatitis. In total, 19 patients (73.1%) were responsive to omalizumab (Fig. 3).
No severe adverse events were observed during the treatment period. Only mild and tolerable adverse events were noted: facial rash (one case), dyspepsia (one case), weight loss (one case), and generalized edema (one case). All patients successfully finished the 24-week treatment.
Comparison of clinical parameters according to the response to omalizumab
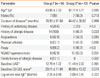
The patients were divided into two groups according to whether they achieved remission at week 24:14 subjects with remission (group I) and 12 subjects without remission (group II; Table). No significant difference in age, gender, disease duration, atopy, angioedema, physical urticaria, or baseline UAS or CU-QOL score was observed between the groups. However, group I had a significantly higher prevalence of personal or family history of allergic diseases compared with group II (P=0.033 and P=0.002, respectively). NSAID hypersensitivity was higher in group II, although the difference was not significant (P=0.051). When comparing the responsive group with the unresponsive group, no significant difference was detected, except that the baseline CU-QOL score was lower in the responsive group (29.69±11.11 vs. 50.75±6.13, P=0.002; data not shown).
DISCUSSION
CU, one of the most frequent skin allergy diseases, is a heterogeneous condition, and prognostic factors for each treatment are not well known. Symptomatic treatment for CU is the most frequently used form of management, and a step-wise approach is recommended.19 First-line therapy with an antihistamine-based regimen may not achieve satisfactory control in 5% to as many as 50% of patients with CU.24,25 Those with refractory CU require the addition of cyclosporine, dapsone, or omalizumab to H1-antihistamines, and frequent exacerbations are treated with systemic steroids. However, the toxicities and adverse events associated with cyclosporine and long-term steroid exposure should be considered carefully.19,26 Thus, a continuing need exists for effective and safe treatments for refractory CU; trials of several novel therapeutics are in progress.
Recent studies have demonstrated favorable effects of omalizumab in patients with refractory CU. Omalizumab significantly improved the UAS, health-related QOL, and medication use, with a rapid onset of effects that persisted for the duration of treatment.15,16,20,27 The onset of effects occurred after 1-2 weeks,15 and greater than 50% improvement in health-related QOL was noted.15,20 In the present study, when we analyzed 26 patients with refractory CU, the effects, including improvement in the UAS, CU-QOL score, and medication use, were comparable to previous findings.15-17,20 However, in eight patients, urticaria symptoms recurred during the treatment period, and medications had to be restarted to control the symptoms, which in half of these subjects recurred at week 24. These findings suggest that although long-term study results are needed, omalizumab may be considered as an alternative regimen for controlling refractory CU in patients who do not respond to conventional treatments.
A longer duration of disease, concurrent angioedema, the combination with physical urticaria, and a positive autologous serum skin test (ASST) are related to severe CU.28,29 While all patients with mild CU were symptom-free after 2 years, more than 30% of patients with moderate-to-severe symptoms appeared to continue to suffer at 5 years.29 At least 50% of patients with CU have angioedema,30 one-third show a positive response on the ASST,31,32 and the prevalence of CU in combination with physical urticaria is 10% to 50%.33,34 These patients were more severely affected and had a longer disease duration.30,33,34 Generally, omalizumab could induce clinical remission in 50%-70% of Western patients with CU.15,20 However, no report has suggested any prognostic factors for predicting the response to omalizumab. In the present study, 53.8% of the patients achieved remission after omalizumab treatment, and half of them exhibited angioedema and physical urticaria. The presence of angioedema, physical urticaria, and the duration of disease were not related to treatment response. Instead, we found a significantly higher prevalence of personal or family history of allergic diseases in the remitted group than in the non-remitted group, indicating that a personal or family history of allergic diseases may be a favorable factor for predicting remission after omalizumab treatment in refractory CU.
Neither severe adverse reactions nor death have been reported in previous studies. Kaplan et al.15 reported no adverse effects. In another study, the rate of adverse events was similar between the omalizumab and placebo groups; the most frequent adverse events were diarrhea, followed by nasopharyngitis, upper respiratory infection, and headache.20 In the present study, minimal adverse reactions were reported in four cases, and no patient discontinued omalizumab treatment.
In conclusion, omalizumab is an effective and safe treatment for patients with refractory CU. The findings suggest that a personal or family history of allergic diseases may be a favorable factor for predicting remission. Further studies will be needed to investigate potential factors for differentiating favorable and unfavorable responders.


 XML Download
XML Download