

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Kawasaki disease (KD) is a systemic vasculitis of medium-sized arteries.1 The pathogenesis of KD has not yet been established, but most feasible theories are based on postinfectious vasculitis in genetically susceptible children less than 5 years of age.2 Thus, the immunologic switches that operate at the peak of infection have been investigated to unveil the pathogenesis of this peculiar disease.1,3,4
There are several unresolved issues regarding the aberrant immune reactions observed in KD.5 First, levels of C-reactive protein (CRP) are often not high in patients with atypical KD; however, coronary arterial dilation has been frequently observed despite low levels of CRP. Second, high levels of interferon (IFN)-γ and immunoglobulin (Ig)E in the serum are observed simultaneously in patients with KD.6,7 The high serum level of IFN-γ does not suppress that of IgE in patients with KD. These two findings suggest that there is another important immunologic factor involved, in addition to already known proinflammatory cytokines. Furthermore, this other regulator may be involved in the differentiation of the germinal center because increased levels of IgE and enlargement of the lymph node may represent defective germinal center differentiation. Clinically, administration of high-dose immunoglobulin (Ig), which is the final product of B cell development, causes rapid shrinkage of enlarged lymph nodes in patients with KD. Before high-dose Ig Koreatherapy, the level of IFN-γ is high and lymph node enlargement seldom subside. Thus, we suspected the new candidate regulator to be involved in the differentiation of B cells, suppression of IFN-γ, and altered expression of serum IgE.
Recently, interleukin (IL)-21, which binds to its receptor IL-21R, has emerged as an important cytokine involved in the pathogenesis of inflammatory diseases, including allergic diseases, cancer, and autoimmune diseases since they were identified in 2000.8,9 IL-21 is a type I cytokine that can inhibit the differentiation of naïve T cells into IFN-γ-secreting Th1 cells.10 When the serum level of IFN-γ is elevated, CD4+ T cells produce IL-21 and inhibit secretion of IFN-γ.11 In addition, IL-21 maintains the activity of CD8+ effector T cells and mainly affects immunoglobulin switching of B cells.12 It functions as a bridge between innate immunity and adaptive immunity,13 and plays an important role in cross-talk among NK cells, B cells, and T cells via a common γ chain which is a common subunit of the cytokine receptors of IL-2, 5, 7, 15, and 21. It is also associated with autoimmune diseases. Autoimmune vasculitis, such as systemic lupus erythematosus, is associated with an increased proportion of Th17 cells due to the stimulation of IL-21.14,15
IL-21R shows structural homology with IL-4R, and is thought to regulate the development of Th2 responses in vivo.16 Interactions between IL-21 and IL-21R affect IgE production induced by IL-4 competitively. In fact, IL-21R gene knockout mice show profoundly elevated levels of IgE.12 Hence, we predicted that a transient lack of IL-21R might induce elevated levels of IL-21 and IgE as well as incomplete B cell differentiation, leading to lymph node enlargement. Elevated levels of IL-21 induce T17 cells, which are related to systemic vasculitis. Thus, by including IL-21 in analyses, the two issues mentioned above regarding KD could be solved.
In the present study, we investigated the involvement of IL-21 in aberrant immune reactions of KD.
MATERIALS AND METHODS
Patients with KD admitted to Wonju Christian Hospital, Yonsei University, Wonju, South Korea, from February 1 to August 31, 2010, were enrolled. The study was approved by the Institutional Review Board of the hospital, and informed consent was received from the parents of patients with KD. The clinical data were analyzed using electronic medical records. The diagnosis of KD was performed by a pediatric cardiologist using KD criteria.17 When the clinical manifestations of a patient met five of the six diagnostic criteria (i.e., high fever for more than 5 days, strawberry tongue and cracked lips, conjunctival injection, cervical lymphadenopathy larger than 1.5 cm, polymorphous skin rash, and swelling of palms and soles), the patient was diagnosed with typical KD. When less than four criteria were met, the patient was diagnosed with atypical KD.
We collected sera in the acute phase of KD, when patients had a fever, and measured serum levels of IL-21 and total IgE in 48 patients with KD. We also measured the serum levels of IL-4 in 14 patients with KD and IL-21 in 12 controls with high fever. Febrile controls were composed of patients suspected of having infectious mononucleosis caused by the Epstein-Barr virus (EBV). Exclusion criteria of febrile controls were having past history of KD or any chronic inflammatory disease including autoimmune disease, and primary or secondary immunodeficiency including hematologic malignancy. Diagnosis of infectious mononucleosis was based on typical clinical symptoms such as fever, sore throat, lymphadenopathy and hepatosplenomegaly, atypical lymphocytosis, and positive results of polymerase chain reaction (PCR) targeting the EBV BALF5 gene. The sera of febrile controls were stored after the diagnostic work-ups for EBV PCR at -70℃ and were used to check the level of IL-21.
The level of IgE in the serum was measured using the Advia Centaur®XP immunoassay system (Siemens, Munich, Germany) and IL-4 and IL-21 levels were measured using enzyme-linked immunosorbent assay (ELISA) kits (eBioscience, San Diego, CA, USA).
Medical history of atopic dermatitis or allergic rhinitis and family history of allergy were taken from the parents of the patients.
The erythrocyte sedimentation rate (ESR), CRP and total eosinophil counts (TECs) were recorded. Echocardiography was performed by the same cardiologist and coronary arterial dilation (CAD) was determined according to the literature.17 Total duration of fever was evaluated using the medical records.
We analyzed the laboratory data and clinical data using GraphPad Prism version 5.0 for Windows (GraphPad Software, San Diego, CA, USA). The difference in the level of IL-21 between KD patients and febrile controls was calculated using Student's t-test. The correlation between IL-21 and IgE levels was calculated using the Wilcoxon rank-sum test. To compare differences in ESR, CRP, TECs, IL-21 and the incidence of CAD according to the level of total IgE, the Mann Whitney U-test (ESR, CRP, TECs, and serum IL-21) or Fisher's exact test (the incidence of CAD) was used. P<0.05 was considered statistically significant.
RESULTS
The demographic characteristics of the study population are shown in Table 1. The median age of KD patients was 3 years of age (range: 0.4-10.0 years). The gender ratio was 1.6:1 (male: female). A total of 10 patients had CAD (20.8%), and there were 38 typical KD cases, 10 atypical KD cases, and 3 intravenous immunoglobulin (IVIG)-resistant cases (6.25%). All 12 febrile controls had infectious mononucleosis caused by EBV infection. The median age of febrile controls was 4.5 years of age (0.6-11) and they had no medical history of KD.
Serum levels of IL-21
The serum levels of IL-21 were significantly elevated in patients with KD compared to those of febrile controls (P<0.001; Fig. 1). The median level of IL-21 in KD patients was 499.5 pg/mL (<62.5-1,544 pg/mL) whereas that of febrile controls was <62.5 pg/mL (<62.5-850 pg/mL). The serum level of IL-21 was not affected by age: even infants <1 year of age had an IL-21 level compatible to that of older children.
Relationships among serum levels of IL-21, total IgE, and IL-4 in patients with KD
The median level of total IgE in KD patients was 58.0 IU/mL (5-1,109 IU/mL). The mean level was 185±310 IU/mL, and the standard error was 45.0 IU/mL. No statistically significant correlation was found between the levels of IL-21 and IgE (Spearman's R=0.2; P=0.19; Fig. 2).
The serum levels of IL-4 were checked in 14 patients with KD. The median value was 4.0 pg/mL (2.1-7.6 pg/mL), and IL-4 was not correlated with total IgE in KD patients (Spearman's R=0.25; P=0.38). We found no statistically significant inverse correlation between IL-4 and IL-21 (P=0.47).
Differences in ESR, CRP, TECs, and IL-21 according to total IgE
Among the KD patients, 16 patients (33%) had a total IgE >100 IU/mL and 30 patients (62.5%) had atopy or a family history of allergic diseases. We divided the patients into two groups according to the serum level of total IgE (>100 IU/mL and <100 IU/mL) and compared the differences in ESR, CRP, TECs, IL-21, and the incidence of CAD between two groups (Table 2). No statistically significant difference was observed between two groups. Total duration of fever was not correlated with the serum levels of CRP, IL-21, or total IgE.
Typical versus atypical KD
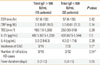
No difference was detected in the level of IL-21 between patients with typical KD and those with atypical KD (P=0.09). The median level of IL-21 in patients with typical KD was 422.5 pg/mL (62.5-1,220 pg/mL) and that in patients with atypical KD was 707.5 pg/mL (62.5-1,544 pg/mL). Other parameters such as total IgE, ESR, CRP, and total duration of fever were not statistically different between these two groups of KD patients (Table 3).
Differences in the incidence of CAD according to IL-21 level
We found no difference in the level of IL-21 between patients with and without CAD (482±102.4 pg/mL vs. 494.8±60.5 pg/mL; P=0.47). Three cases with refractory KD were observed in the present study, and no difference was found in IL-21 between refractory KD patients and well controlled KD patients (data not shown).
DISCUSSION
KD is the most common acquired heart disease in children. High-dose IVIG has proven effective for stopping aberrant immune reactions in KD, which led to the research for an association between KD and abnormal B cell development during infection.18-20 Corticosteroid or aspirin could not be a substitute for IVIG for the protection of coronary arteries in KD.17,21,22 Thus, KD is different from other types of adult autoimmune vasculitis. As early as 1996, Lee et al.20 suggested that abnormal immunoglobulin switching might be involved in the pathogenesis of KD based on evidence that aberrantly increased immature B cells (CD5+ B cells) were suppressed by IVIG therapy. In 2000, the IL-21/IL-21R pathway was reported to be a major factor in B cell development.23 Interestingly, until now, IL-21 and IL-21R had not been investigated in KD, although hypotheses regarding defective B cell differentiation had been suspected as the pathogenesis of KD. Therefore, we concentrated on IL-21 as another possible factor in aberrant immune reactions, and found elevated levels of IL-21 in the serum of patients with KD.
Compared with other cytokines, IL-21 has a potent effect on isotype switching and development for plasma cells, resulting in the production of large quantities of immunoglobulin (up to 50-fold increases).24 IL-21 is important for T cell-dependent antigen-specific immunoglobulin production via CD40 ligand stimulation in humans.24 If there is a blockade in producing effective IgG against a specific antigen, IL-21 could be increased. IL-21 affects germinal center formation of lymph nodes, and IL-21-producing CD4+ T cells are prohibited by another T cell marker, the PD-1 molecule.25 If there is a defect in PD-1 expression, IL-21 production would be increased due to absence of inhibitory feedback. Hence, immunoglobulin-like structures such as PD-1 and IgG may regulate the production of IL-21. We have not yet known if any other abnormality exists in other factors related to B cell development such as Blimp-1, SAP, SOCS-1, or Bcl-6 expression in patients with KD.
In the present study, KD patients had elevated IL-21 levels regardless of age. Andersen et al.26 found that IL-21 was increased in adult spondyloarthritis compared with healthy volunteers. Therefore, elevated serum IL-21 may suggest an inflammatory cascade of autoimmunity in adults and children. In febrile controls (i.e., patients with EBV infection), IL-21 levels were low, although ESR levels were not statistically different from those in KD patients. No difference was noted in IL-21 levels between patients with typical and atypical KD. Thus, we may use serum levels of IL-21 for the differential diagnosis of KD.
We suspected that the high incidence of CAD in patients with atypical KD may be related to elevated IL-21 rather than CRP or IL-6. A low CRP is often found in patients with atypical KD. We predicted that these incompatible results between coronary findings and CRP levels could be explained by the existence of a high IL-21 level. However, our data showed no difference in IL-21 between patients with and without CAD. We interpret these results as follows. First, minimal arterial changes are undetectable, so only severe cases are categorized as having coronary arteritis. If IL-21 is involved in the initial phase of arteritis, IL-21 may be elevated both in patients with CAD and in those with coronary arteritis but without CAD. Second, the role of other factors such as vascular endothelial growth factor (VEGF) or transforming growth factor-β (TGF-β) may be more important than IL-21 in progressing arteritis.
Initially, we thought that the phenomenon of low IL-4 and increased IgE in KD could be explained by the involvement of IL-21 because IL-21 works together with IL-4 competitively. However, our data showed no direct correlation between IgE and IL-21 in patients with KD. The normal range of IgE increases with age.27 Thus, evaluating whether the measured level of IgE is elevated is difficult because the level should be compared with the normal range for each age. We defined an elevated level of IgE as 100 IU/mL, according to previous report.27 We tried to determine whether the high level of IgE may affect inflammatory reactions in patients with KD. However, no difference was observed in inflammatory markers between the group with IgE >100 IU/mL and the group with IgE <100 IU/mL. Thus, we assumed that elevated levels of IgE may not reflect the severity of inflammation. The total eosinophil count was not different between those two groups either.
What is the role of IL-21 in vasculitis? According to the literature, increased IL-21 enhances the production of autoantibodies.28,29 Blocking IL-21 with IL-21R Fc antibodies reduces inflammation in lupus-prone mice.28 IL-21 induces the development of Th17 cells, which are involved in autoimmune vasculitis.8 Interferon regulatory factor 4 (IRF4) is the main transcription factor for IL-17 and IL-21.8 IL-17 has been reported to be increased in KD.14,15 We think that abnormally increased IL-21 may be a sign of the ineffective production of antibodies against a certain infection in patients with KD. To maximize antibody production in individuals whose IL-21R is transiently down regulated due to young age, frequent infections, or frequent vaccinations, IL-21 could be increased. Elevated IL-21 may increase the production of IgE despite the high level of IFN-γ in patients with KD. In another aspect of pathogenesis of KD, if KD patients are producing autoantibodies such as anti-endothelial cell antibodies,30 α-enolase antibodies,31 α-human cardiac myosin autoantibodies,32 and cardiolipin antibodies,33 the autoreactive process could be augmented by an increased IL-21 level.29 Thus, IVIG therapy in KD may effectively suppress the ineffectively activated immune system by providing effective IgG directly and decreasing level of IL-21.
The phenomenon of increased IgE in KD has been explained as increased activity of IL-4,34 IL-5, or eosinophils.35 Our study was performed in line with these studies but showed different results. Although we could not find a direct correlation between IgE and IL-21 in the present study, further studies on IL-21, IRF4, and anti-IL-21 would solve the mysteries that remain concerning allergy, autoimmune vasculitis, and KD.




 XML Download
XML Download