

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The incidence of bronchial asthma in the elderly population is increasing. By the year 2030, the number of such patients will more than double, to almost 5 million in the USA alone.1 Asthma affects 5.3% of those >65 years of age in the USA,2 and the rates are higher in Australia, reaching 10.1% of those >64 and 11% of those >75.1 In Korea, asthma was found to affect 12.7% of people >65 years of age.3 Although the mortality rates associated with asthma have, in general, decreased, they have increased among elderly individuals.2,4 Moreover, almost half of the asthma-related deaths per 100,000 people (5.8/100,000) occurred among those >65.5
Elderly individuals with asthma have several characteristics that differ from their younger counterparts. First, they have decreased lung functioning, with stiffened chest walls, weaker respiratory muscle strength, and an increased residual volume; these impairments exist in addition to the loss of elastic recoil Koreathat occurs as part of the aging process. Second, they respond less well to asthma medications such as bronchodilators and glucocorticoids.6 These traits can contribute to severe symptoms in elderly patients, including impaired abilities, decreased quality of life, and frequent near-fatal episodes.7,8 Third, the coexistence of asthma and chronic obstructive pulmonary disorder (COPD) is frequent in elderly patients due to smoking habits and exposure to endotoxins, organic dust-like grains, cotton, barn environments, and drying tobacco dust as well as latent adenovirus infections.6 Fourth, comorbid conditions such as depression and obesity increase the rate of hospitalizations, emergency-room (ER) visits, and ambulatory-care visits.9 Together, these findings indicate that elderly individuals with asthma generally experience more severe symptoms and higher rates of poor control over the disease than do younger individuals with this condition.
Severe asthma in elderly individuals has been associated with frequent (>4 puffs per day) use of salbutamol, >10 years of symptoms, and >500 mL reversibility in the forced expiratory volume during 1 second (FEV1).10 A study in the USA reported that predictors of uncontrolled asthma despite the use of standard asthma medications included younger age, Hispanic ancestry, male sex, lower income, less education, chronic sinusitis, high blood pressure, and gastroesophageal reflux disorder (GERD).11 A European study suggested that suboptimal anti-asthma drug use was the main predictor of poorly controlled states of asthma.12 Both studies emphasized the need to monitor asthma control through proper health care, medication use, and coordinated care of comorbid conditions. To our knowledge, the published study focused on the predictors of asthma control in the elderly is rare. Therefore, we investigated the characteristics of poorly controlled asthma in the elderly and identified the factors that contributed to poor control.
MATERIALS AND METHODS
Study design and subjects
The study protocol was reviewed and approved by the Ajou University Institutional Review Board, and informed consent was obtained from each subject. This retrospective, observational study was conducted at Ajou University Hospital from October 2010 to March 2011. A total of 108 subjects aged ≥60 years and diagnosed with asthma were enrolled in the study. The study subjects enrolled in this study had recurrent episodes of wheezing, breathlessness, chest tightness, and coughing, particularly at night or in the early morning and/or airway hyperresponsiveness or widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment and this was observed by physician for at least 1 year. We excluded the patients with cognitive dysfunction. Subjects were classified into two groups according to scores on the asthma control test (ACT), which was previously validated for use in Korea.13 Group I consisted of 38 patients with ACT scores ≤19 and was defined as the group with poor control. Group II included 70 patients with ACT scores >19 and was defined as the group with good control.14
Clinical data and comorbid conditions
Data on age, sex, history of smoking, duration of disease, age at onset, weight, height, aspirin hypersensitivity, and occupational relationship with asthma were collected by reviewing patient charts. Skin-prick tests were performed for 50 common aeroallergens (Bencard, Bretford, UK). A positive reaction was defined as a ratio of the mean wheal diameter of the allergen to that of the histamine of >1. Atopy was diagnosed if a positive response to at least one common inhaled allergen was observed by either the skin-prick test or serum-specific IgE test using the ImmunoCAP system (≥0.35 KU/L; Pharmacia-Upjohn, Uppsala, Sweden). The frequency and cause of admission or ER visit during the year prior to study enrollment and the presence of comorbid conditions were noted. The clinical features of the study subjects are summarized in Table 1.
Pulmonary tuberculosis (TB) lesions on chest x-rays were defined by the presence of discrete linear or reticular fibrotic scars or dense nodules with distinct margins, with or without calcification, within the upper lobes; findings were then confirmed by a radiologist. The cases showing tissue destruction due to TB having impact on lung function were excluded.
Evaluation of pulmonary function
Methacholine bronchial-challenge tests were performed according to previously described methods.15 Bronchial hypersensitivity was defined by a PC20 value ≤25 mg/mL in a methacholine-challenge test. Spirometry was conducted by trained pulmonary technicians following the 1994 American Thoracic Society (ATS) recommendations16 using a Jaeger spirometer (Jaeger Pneumoscreen II/1; Epich Jaeger GmbH, Hoechberg, Germany). Reversibility was defined by an increase in FEV1 of ≥12% and ≥200 mL after a short-acting β-agonist or medical treatment. Sputum was induced using a previously described method.17 Eosinophil counts of ≥3%18 and neutrophil counts of ≥65%19 in the induced sputum samples were considered positive.
Treatment and compliance
All asthma medications prescribed to the enrolled patients were identified via their medical records; these included inhaled corticosteroids (ICSs), inhaled corticosteroids/long-acting β-agonists (ICSs/LABAs), theophylline, short acting β-agonists (SABAs), leukotriene-receptor blockers (LRTAs), and systemic corticosteroids (SCSs). The frequency and total amount of use of the asthma medications were determined for the year prior to study enrollment. Medication possession ratios (MPRs) were also calculated by dividing the number of days a medication was supplied by 365 days (the maximum ratio was 1.0 or 100%). MPR can be used as a measure of compliance.20 MPR values provide information regarding whether a patient is using the proper amount of medication within a defined time period. Medication compliance for our patients was calculated for the year following study enrollment using the median and the 75th percentile MPR, defined a priori, for ICSs with or without LABAs, LTRAs, SCSs and theophyllines. To make the control state and index about medication compliance accurate, we selected the asthmatics with previous one-year history of treatment with anti-asthmatic agents and prescribed for only the amount of medications patients asked for.
ACT and asthma quality of life (AQOL)
ACT and AQOL questionnaires were distributed to all enrolled patients.21,22 The ACT has established internal consistency reliability, known-groups validity, and responsiveness; it was previously translated into Korean.13 An ACT score of ≤19 identifies patients with poorly controlled asthma.14 AQOL is an easy and validated tool with good psychometric properties for assessing the quality of life of patients with asthma.22 Subjects were surveyed on the day of enrollment, and the time after anti-asthmatic treatment.
Statistical analysis
Clinical data were compared with Pearson chi-square tests or independent-samples t-tests. The prevalence of comorbid diseases and their medication requirements were analyzed using Pearson chi-square tests. We constructed a multivariate binary logistic regression model using poorly controlled asthma as the dependent variable and age, sex, smoking status, FEV1 value, obesity, atopy, duration of asthma, comorbid conditions, and medication compliance as independent variables. All computations were performed using SPSS software, version 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Clinical characteristics of patients (Table 1)
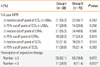
Of the 108 enrolled subjects, 54.6% were female, 7.5% were obese, 32.4% had a history of smoking, and 49.0% were atopic. The mean age of the patients was 70.5, and the average amount of time patients had suffered from asthma was 15.5 years. Those with late onset (≥40 years) comprised 80.6% of patients, and this group experienced less frequent ER visits and clinical admissions than did the group with early to middle onset (5.1% vs. 26.3% for ER visits, P=0.004; 10.1% vs. 26.3% for clinical admissions, P=0.062). Aspirin-intolerance, and occupational asthma were observed in 13.0%, and 4.6% of subjects, respectively. Severe asthma with FEV1 values <60% was noted in 15.7% of patients. Pulmonary function tests resulted in mean values of FEV1, MMEF, and FVC of 88.3%, 67.6%, and 82.3%, respectively. Positive eosinophil (≥3%) and neutrophil (≥65%) counts in the sputum were observed in 36.5% and 80.8% of 52 study subjects, who did sputum exam respectively. The frequencies of unscheduled outpatient clinic visits (7.4%), ER visits (8.3%), clinic admissions (12%), and steroid-burst prescriptions (51.9%) were also examined.
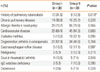
Comorbid conditions (Table 2)
Common comorbid conditions were noted in our patient cohort; these included allergic rhinitis and/or nasal polyp (76.9%), cardiovascular disease (65.7%), degenerative arthritis and/or osteoporosis (51.9%), chronic pulmonary disease (29.6%), diabetes mellitus (22.2%), GERD (15.7%), malignancies (10.2%), gout and/or rheumatoid arthritis (8.3%), IgG subclass deficiency (8.3%), and depressive disorder (5.6%). Patients with poorly controlled asthma (group I) were significantly more likely than those whose asthma was well controlled (group II) (31.6% vs. 12.9%, P=0.019) to have a history of TB. The 21 patients with a history of TB were predominantly male and had lower rates of obesity compared with those without a history of TB (61.9% vs. 41.4% male, P=0.090 and 0% vs. 9.3% obese, P=0.146). Mean FEV1, MMEF, and FVC values were significantly lower in patients with a history of TB than in those without such a history (74.4% vs. 91.7% FEV1, P=0.007, 51.9% vs. 71.5% MMEF, P=0.029, and 75.8% vs. 87.2% FVC, P=0.027). Moreover, these patients had significantly higher rates of chronic pulmonary diseases such as bronchiectasis and/or COPD (47.6% vs. 25.3%, P=0.044) and were more often treated with ICSs/LABAs (76.2% vs. 42.5% took MPR50, P=0.006, and 38.1% vs. 19.5% took MPR75, P=0.070).
Asthma-control status
The mean ACT score for all patients was 20.2, and the incidence of poorly controlled asthma (ACT≤19, group I) was 35.2%. Group I was characterized by lower mean AQOL scores (83.5 vs. 105.7, P<0.001), a greater proportion of patients with a history of TB (31.6% vs. 12.9%, P=0.019), and higher admission rates for asthma-related issues (21.1% vs. 7.1%, P=0.034) than was group II (Tables 2 and 3). Patients with prescriptions for adjunctive therapies were more prevalent in group I than in group II (28.9% vs. 11.4%, P=0.022; Table 4).
When analyzing multivariate logistic regression with covariables, smoking habit, atopy, obesity, FEV1, late onset of disease, medication compliance and comorbid conditions, a patient's history of TB as a significant predictor of poorly controlled asthma (sex and age adjusted OR=4.70, 95% CI=1.06-20.81, P=0.042, Table 5).
DISCUSSION
In this study, we described a cohort of 108 elderly individuals with asthma. At first, the characteristic findings were frequent unscheduled outpatient clinic visits (7.4%), ER visits (8.3%), clinic admissions (12%), and steroid-burst prescriptions (51.9%), which were consistent with the findings of previous studies in Australia and USA.1,8 However, patients had even more frequent admission episodes than subjects of TENOR study with severe or difficult-to-treat asthma (12% vs. 4.6%).23 This might be because asthma was often more severe and hospitalization for asthma exacerbation was more frequent among elderly individuals.8,24 Second, no differences between groups I (poor controllers) and II (controllers) were detected in medication use or compliance. In Lee's study7 from Singapore, even though elderly asthmatics were on significantly more anti-asthmatic medications (2.3+1.1 vs. 1.6+0.9, P<0.001), they had clinically more severe symptoms (Step 2.2±1.2 vs. 1.7±1.0, P<0.001) and more frequent near-fatal episodes (39% vs. 13%, χ2 test P<0.01) than younger patients. However, in a European sample of adults, suboptimal treatment were correlated with poor control of asthma.12 This difference might be from the different characteristics of study subject between these studies (university hospital vs. general clinic, high adherers vs. low adherers) and lack of data about proper usage of inhaler, small number of subjects and no direct comparison to matched younger patients. Third, no differences were noted in duration of asthma and smoking history between group I and II. Duration of asthma was proved as independent predictor for airflow limitation, hyperinflation and severity of asthma, and smoking history for steroid dependent asthma in elderly, but not for lack of control.25-28 This could be explained by that the predictors differ markedly depending on definition of outcome (based on lung function vs. steroid-dependent asthma vs. control status).29 Therefore, these findings suggest that the clinical features of asthma appear to be more severe in elderly patients and that close monitoring of these patients will be essential for the achievement of asthma control.
More than half of the elderly asthma patients in our study reported chronic comorbid conditions such as allergic rhinitis, cardiovascular disease, and degenerative arthritis. In the Real-world Evaluation of Asthma Control and Treatment (REACT) Study, hay fever and allergic rhinitis were experienced by >50% of the 1,812 enrolled adult patients with asthma; arthritis, high blood pressure, obesity, and GERD were present in >25% of these patients.30 Cazzola et al.31 reported that hypertension (23.8%), allergic rhinitis (19.7%), and GERD (18.7%) were the most frequent comorbid conditions suffered by Italian adults with asthma, with cardiovascular disease and osteoporosis also common. The prevalence of allergic rhinitis in adults with asthma was reported to be 60%-80% in Korea,32 and this condition was also closely associated with more frequent asthma attacks, ER visits, and poor asthma control.33,34 Elderly women with asthma were particularly likely to have weakened bone structures after a 6-month treatment regimen with ICS, this was replicated in our data (degenerative arthritis and/or osteoporosis, 71.2% in female vs. 28.6% in male, P<0.001).35 These findings suggest that comorbid conditions are common among elderly patients with asthma and that evaluation and proper control of these conditions will improve asthma control in this population.
In this study, 35.2% of the subjects suffered from asthma that was poorly controlled like 36.5% in UK GP practice.36 Patients with poorly controlled asthma were more likely to have a history of pulmonary TB and hospital admission despite the high rates with which this group used adjunctive therapies. Additionally, the quality of life of patients with poorly controlled asthma tended to be worse than those of patients whose asthma was well controlled, a result reported by this and other studies.13,37 The history of the previous TB was an independent risk factor for obstructive lung disease in a recent Korean study.38 Our data also demonstrated an association between pulmonary TB and uncontrolled asthma with odd ratio, 4.61, even after adjusting for sex, age, smoking history and lung function. It is likely that prior TB infection may contribute to an irreversible change in the airways that results in poorly controlled asthma in elderly individuals.25
Our study has several limitations. This was a cross-sectional, retrospective study involving a sample that was not sufficiently large to permit statistically significant conclusions about the factors that predict asthma control. Moreover, the clinical characteristics of the study cohort were similar, and all patient records were obtained from a single university hospital. Future prospective, multicenter studies with large cohorts are needed to thoroughly examine the factors that contribute to asthma control in elderly individuals with asthma.
In conclusion, asthma in elderly patients presents with more severe and higher rates of comorbid conditions. One-third of these patients had poor control over their disease, leading to frequent clinical admissions. Given that a history of pulmonary TB was a predictor of poor control over asthma, careful evaluation and proper management of comorbid conditions should improve the control wielded by elderly individuals over their asthmatic conditions.



 XML Download
XML Download