

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Immunological reactions to drugs, also known as hypersensitivity drug reactions (HDR) are considered within the category B of adverse drug reactions where the mechanism is related with the subject abnormal response to the drug.1 This is in contrast to type A reactions that occur in normal individuals and are usually dose-related. Within the category B, HDR are those mediated by immunological mechanisms and may contribute up to one third of all reactions.2-4 In the last years there has been a growing interest in this area of knowledge with an increase in the scientific production and worldwide activities dedicated to it.5 This manuscript will focus on the immunological evaluation of HDR. For this purpose it is needed to analyse in certain detail what are the mechanisms involved. In addition drugs reactions to biological agents will be also included, given the increasing importance of these in the elicitation of reactions.6
CLASSIFICATION OF ALLERGIC DRUG REACTIONS
Allergic reactions can be produced by any of the four immunologic mechanisms proposed by Gell and Coombs.7 Type I reactions, also called immediate-type reactions, occur usually within less than one hour after drug administration and are mediated by drug-specific IgE antibodies. Classical examples are anaphylaxis and urticaria induced by betalactams antibiotics, otherwise the most frequent drugs involved in immediate hypersensitivity reactions.8,9
Type II (cytotoxic reactions) and Type III (immune complex reactions), are usually mediated by IgG or IgM specific antibodies.7 Although with the classical drugs (organic compounds) it has been difficult to prove their involvement in Type III reactions, this mechanism is gaining interest in the last years with the use of biological agents, with some evidence pointing out that this can be the case.6 Type IV reactions, mediated by effector drug-specific-T cells, are also known as delayed hypersensitivity reactions (DHR) since they appear from hours to days after the drug intake.10 We will refer to this group in this review as non-immediate allergic reactions. In the immunological evaluation we also include a group that although inflammatory mediators are released, same as those involved in IgE-mediated reactions, non-specific immunological mechanisms take part, as occurs in reactions induced by NSAIDs.11 These are in fact the most common group of drugs involved in HDR.12 In general, all these reactions are included within hypersensitivity reactions, being the term allergic reactions reserved for those where an immunological mechanism takes part.13
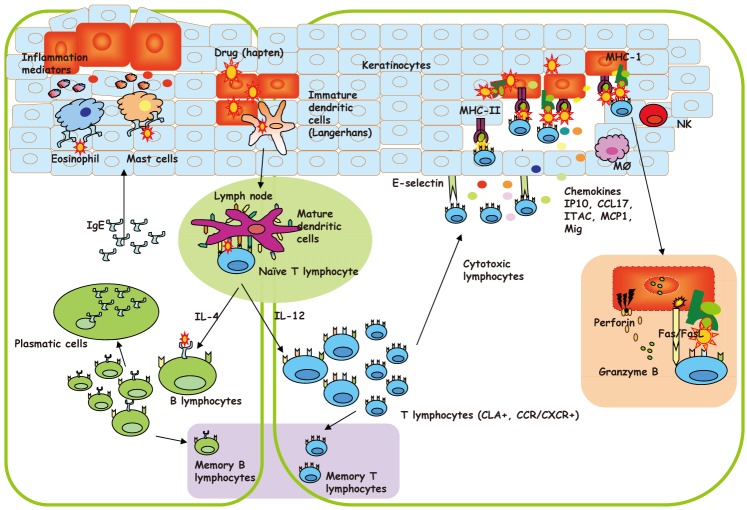
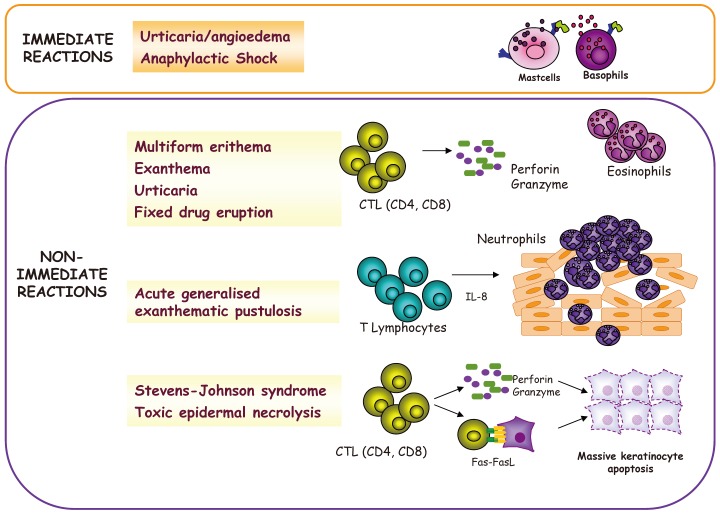
For those where specific immunological mechanisms are involved, a working classification has been adapted from the former proposed by Levine14 considering the immediate reactions as those occurring within one hour after the drug intake and non-immediate reactions as those who occur later than one hour after the drug administration including both accelerated and delayed reactions.15 In general, these reactions can occur from hours to days or even weeks after drug intake and are characterized by a wider range of clinical manifestations than immediate reactions.10 In Fig. 1, it is shown a general pictogram of both immediate and non-immediate reactions with the cell involved. Detailed analysis of these will be given through the text.
IMMEDIATE TYPE IGE MEDIATED REACTIONS
General considerations
Typical reactions included within this group are anaphylaxis and urticaria. Betalactams antibiotics continue to be the most frequent drugs that induce these reactions.16,17 The facility for binding spontaneously to endogenous proteins renders them to some extent immunogenic and able to induce IgE antibodies.9,16 In addition, immediate reactions have been reported by many drugs with an increasing list although at a much lower proportion than betalactams. Relevant emerging drugs are NSAIDs and quinolones.18,19
In the case of betalactams several determinants generated from benzyl penicillin have been proposed (BPO and MDM).8,14 Moreover, other betalactams provide determinants that must be considered in the immunological evaluation.16,20-25 The more relevant for the diagnosis of immediate reactions is amoxicillin and recently clavulanic acid as well as cephalosporins.20,22,25 Second relevant drugs are NSAIDs that although in most instances induce non immunological mediated reactions, up to 30% of subjects can develop urticaria/angioedema or anaphylaxis with a selective response mediated by an IgE mechanism.18 Pyrazolones are the most relevant drugs although propionic acid derivatives, particularly ibuprofen, followed by the aryl acetic acid derivative diclofenac are gaining in importance in this type of reactions.12,18,26 Weather ibuprofen itself or some of its metabolites are the responsible for IgE mediated reactions is not known at present.
In vivo diagnosis
Skin testing is the most sensitive tests for the diagnosis of immediate reactions to betalactams.27 General principles for skin testing with these and with the rest of the drugs are provided by the ENDA group.20 Maximal recommended concentrations are for BPO 5×10-5 M for MDM 2×10-2 M and for amoxicillin and clavulanic acid 20 mg/mL. With soluble cephalosporins concentrations of 20 mg/mL can produce false positive results in some of them due to an irritant effect and 2 mg/mL is recommended.20 Working concentrations for the rest of drugs involved in immediate reactions are also provided.28
Sensitivity for skin testing with betalactams and with the rest of the drugs is time dependent after allergic episode occurrence with subjects converting from positive to negative as time elapses.29-31
In vivo sensitivity is not optimal what implies that in the event of a clear positive history, if skin test negative, subject can still be allergic.16,17 Only in a minor proportion of cases in vitro tests can be positive with skin test negative but up to 20%-30% of patients may need a control administration of the drug for confirming the diagnosis.32,33
In vitro diagnosis
Most assays developed for drug specific IgE detection including the commercial ones consisted on the quantitation of IgE using radiolabelled anti IgE antibodies (RAST) or more recently enzyme (ELISA) or fluoroenzyme (FEIA) assays. The principle consists in a solid phase to which the hapten conjugated to a carrier protein is bound covalently. The carrier proteins can be HSA or other molecules like polylisines or aliphatic spacers.34-36 Although HSA has been used for many years37 this has not shown to be the most suitable carrier being preferable in many instances others with a high capacity for hapten fixation and exposition to IgE antibodies.34-36,38,39 Since last years the radiolabelled method has been substituted for the ELISA and later with the FEIA although no sufficient comparatives studies has been made so far. In general, it is accepted FEIA sensitivity for BPO is reasonable compared to skin testing,40 however, for other betalactams, including amoxicillin, important differences in sensitivity exist.39 This is particularly relevant in the cases of cephalosporins where sensitivity non higher than 20% has been reported.41 This can be due to the not inclusion of the culprit cephalosporin. For many years only cefaclor has been available for in vitro testing and it is well known that for this betalactam the side chain at R1 position is very important in the specific IgE recognition.25,42-44 Similar assays have been developed for other drugs, being in most cases experimental prototypes that need further validations in a sufficient number of positives controls.45-52
An alternative solid phase used for many drugs has been epoxy activated sepharose to which drugs bind covalently. Classical drugs used have been cephalosporins,28,29 quinolones,30,31 and muscle relaxants32 with different sensitivity and specificity results.
It is relevant to note that drug allergy IgE mediated can be an occupational disease affecting workers involved in health care, pharmacy and industries producing or manufacturing pencillins, cephallosporins53-55 as well as other antibiotics.56 In this sense the group of Park has published several reports using the methodology outlined above for diagnosing these cases.53-56
BASOPHYL ACTIVATION TEST (BAT)
The flow cytometry technology facilities exploit the capacity of basophyls to be activated after the interaction of the hapten with specific IgE antibodies on their surface.57 The principle is based on the basophyl property for expressing in their cell membrane di novo or increased upon activation different markers, being the most widely used CD63 and CD203c.57,58 Although this methodology is actually mostly reserved to specialised centres involved in drug allergy, its advantage is that different drugs can be used that are not available for skin testing, have anti-inflammatory properties and/or lack the ability to be conjugated to a solid phase support in an efficient way as occurs with corticoids,59 quinolones,60 contrast media,61 dipyrone,62 anaesthetics,63,64 omeprazol,65 cyclosporine66 as well as many other drugs.67 Most studies have been carried out with betalactams antibiotics.68,69 With this technique sensitivity approaching 60% have been obtained with cases detectable only by the BAT assay being negative to both intradermal testing and the in vitro immunoassays.68 The potential use of these techniques deserves further studies with the possibility of including more drugs for proving the existence of specific IgE antibodies.67
CELLULAR ANTIGEN STIMULATION TEST (CAST)
Alternative to the BAT, the CAST is based on the quantitation of sulfidoleukotrienes released in the supernatant after basophyl stimulation.70 In general this technique has been used in the last years but did not show clear advantages compared to basophyl activation.57 Important to note is that the flow cytometer is not required for their performance but only a system for quantifying the histamine released.57,70 However, no agreement has been made about when and how this technique must substitute the others available or under which circumstances this is indicated.70
NON-IMMEDIATE TYPE T CELLS DEPENDENT REACTIONS
General considerations
These reactions are produced of sensitised T cells that recognise drugs as xenobiotics and induce an immunological effector response.7 Although T cells reactions can occur virtually with any drug in any organ,71 the skin is the most frequent target involved.10,72,73 Clinical entities are shown in Fig. 2. They ranks from maculopapular exanthema to non-immediate urticaria and other less common but more severe entities such as AGEP, drug rash with eosinophilia and systemic symptoms, drug hypersensitivity syndrome (DHS), Stevens-Johnson syndrome (SJS), and Toxic epidermal necrolysis (TEN), fixed drug eruption and contact dermatitis as well as organ specific reactions.72,73 Although maculopapular exanthema is the most common reported reaction, it can sometimes be intense, accompanied with subcutaneous angioedema, and persists for several weeks despite discontinuation of treatment.73 DHS and bullous reactions with mucosal involvement are considered severe diseases.10,72 Erythema multiform, which is less severe, is usually induced by virus and characterized by the presence of typical target lesions.
There is growing evidence that SJS and TEN are a single disease with common causes and mechanisms; the main difference appears are the extent of detachment, which is limited (<10%) in the case of SJS and more widespread (>30%) in that of TEN.74 While rare (2 cases/million population/year), SJS and TEN have high mortality (20%-25%).75
Although all of them are considered T cell mediated drug hypersensitivity reactions, there are important differences in the effector cells involved.73,76 The clinical manifestations described result from the interplay of the immunological system and the cutaneous tissue. In maculopapular exanthema a mononuclear cell infiltrate can be found in the perivascular dermis, with T lymphocytes, mainly CD4 T cells,77-79 with the presence of neutrophils and occasionally eosinophils.80 Recent skin patch test studies have shown CD8 T cells in the dermoepidermal junction81-83 with a cytotoxic capacity.84-87 If this occurs at the onset of the acute response needs to be confirmed. Controversy exists concerning whether non-immediate urticaria or urticarial-like exanthematic rash is a T-cell reaction, although there is evidence that in some cases drug administration induced an urticaria-like reaction with the presence of angioedema and T-cell involvement.78-87 In this process an intradermal infiltration with activated CD4 and CD8 T cells producing granulocyte-macrophage colony-stimulating factors, with IFN-γ and TNF-α with the release of perforin/granzyme B and Fas L expression, which are responsible for keratinocyte death.88,89 These T lymphocytes also produce IL8 (CXCL-8), which is responsible for neutrophil chemoattraction and activation.88-92 Fixed drug eruptions are characterized by intraepidermal resident CD8 T cells with an effector memory phenotype, responsible for keratinocyte necrosis.93-95 CD4 T cells are also found and are thought to act as regulatory cells.84 TEN is characterized by the keratinocyte production of CCL27, which recruits CD4 and CD8 T lymphocytes expressing cutaneous lymphocyte antigen and CCR10 that produce IFN-γ, TNF-α, perforin/granzyme B/granulysin and FasL, which develop the apoptotic mechanisms followed by a massive necrosis.96 In DHS, in addition to the skin exanthema, there are also hematological abnormalities, with eosinophilia and the presence of atypical lymphocytes CD4 Th2 cells producing IL-5 which are involved in the eosinophil activation and trafficking. CD8 T cells also participate, which is the cause of organ damage in this syndrome.95 A general outline of the mechanistic process that occurs in non-immediate reactions is outlined in Fig. 2. Although simplifying drugs as haptens or protohaptens interact with immature dendritic cells Langerhans cells in the skin that become mature or partially mature and migrate to the regional lymph-node interacting with naïve T cells that become memory T cell. To this follows a complex process of homing and skin recruitment that will induce the different pathological entities described.
Diagnosis
Difficulties in the diagnosis of these types of reactions reside in the lack of sensitivity of the available tests both in vivo and in vitro. For the assays it is important to detect the specific cell subpopulation involved and the adequate drug or drug metabolites eliciting the immunological response.15,76 Other difficulties are the lack of knowledge of the cofactors that may have been present at the time of the reaction, and the possibility that symptoms attributed to the drug were not immunologically mediated.73
Skin tests
Reliable skin test procedures for the diagnosis of non-immediate reactions are generally lacking and test concentrations are often unknown or poorly validated for many drugs.28 Delayed-reading intradermal and/or patch tests 24-48 hours after the drug application have been used for many years.97,98 The main advantage of drug patch tests is that they can be performed with any commercially available drug, while intradermal tests are more sensitive, but they need to be performed with a soluble injectable or a pure form, sterile preparation of the drug.97 Both intradermal and patch tests have been widely used in the diagnosis of non-immediate reactions to betalactams, with reported sensitivity ranging from 2.6% to 37.8%.99 Further evidence seems to indicate that skin test sensitivity is lower than previously believed.100-102
Lymphocyte transformation test
In the last years a considerable effort has been made in the reintroduction of lymphocyte transformation test assays in the evaluation of DHR.103,104 This is based on the principle that T cells can proliferate in the presence of a specific antigen. The usefulness of this test in the diagnosis of non-immediate reactions has been debated pointing out that it depends on the drug involved in the reaction.105 Reports published to date have been characterized by small series, a wide range of drugs and different clinical entities and show and overall sensitivity rating 60% to 70% with a rather low specificity (85%).103,104,106,107 However, this test is not available everywhere and is still considered a research tool. In a study by our group, 57% of patients with a non-immediate reaction to betalactams had a positive lymphocyte transformation test to at least one of the penicillins tested.104 A recent study analysing the role of dendritic cells in the enhancement of amoxicillin-specific lymphocyte proliferation in patients with non-immediate reactions to amoxicillin showed that compared to traditional antigen-presenting cells such as B cells or monocytes, dendritic cells improved lymphocyte transformation test sensitivity.108 Similar results have been obtained for non-immediate reactions with other drugs such as heparins and contrast media.109,110
Immunopathological studies
Because in many instances DHR affect the skin, samples can be taken from the lesions at both the acute reaction as well as after positive drug provocation or a delayed skin test. While the immunohistochemistry findings help in the investigation of underlying immunologic mechanism, they do not provide information about the drug involved or even discriminate between different types of reactions. The most common finding is a mononuclear cell infiltrate composed mainly of activated T cells expressing activation markers such as CD69, IL-2R (CD25) and HLA-DR, and the skin-homing receptor cutaneous lymphocyte antigen in both CD4 and CD8 T cells with a predominance of one of them depending on the clinical manifestation.15 In maculopapular exanthema, for example, a predominant perivascular mononuclear cell infiltrate with increased numbers of eosinphils in the papillary dermis has been found, with up to 20% of the cells expressing perforin and granzyme B and enhanced IL12 expression.76 SJS/TEN, in contrast, is characterized by the presence of many dead keratinocytes with a minimum T-cell infiltration, probably due to the loss of superficial skin layers.15,73 In AGEP, keratinocytes express high levels of IL-8, a chemokine that recruits neutrophils to the epidermis.80,88,89
Fig. 3 represents examples of the haematoxylin eosin staining and immunohistochemistry for cell marker of lymphocytes subpopulations as well as effector molecules involved in the lessional skin process.
Drug provocation studies
Because intradermal or patch testing have non optimal sensitivity in patients with non-immediate reactions, a large proportion of patients need to be given the drug to establish a diagnosis or, perhaps more often, to confirm tolerance.111 Drug provocation testing is the best tool by which a causal relationship between drug administration and a non-immediate reaction is established.15 It involves the careful administration of a suspect agent in a specialized centre and close monitoring for symptoms, in particular skin manifestations. Drug provocation testing, however, is not generally recommended and is contraindicated in some cases such as generalized bullous fixed drug eruptions, AGEP, SJS, TEN, DHS/DIHS, systemic vasculitis, specific organ manifestations (blood-cytopenia, hepatitis, nephritis, pneumonitis) and drug-induced autoimmune diseases.75,111
Of all the drugs suspected to cause non-immediate reactions, betalactams have been the most extensively studied.100,112,113 Most patients who develop an exanthematic reaction after betalactam administration and have negative skin tests can tolerate drug in a drug provocation test.87,102 Nonetheless, some patients with clear non-immediate reactions are diagnosed by a positive drug provocation test. This indicates that drug provocation testing is the most important diagnostic tool in the particular case of exanthematic reactions to betalactams.113
NON-ALLERGIC HYPERSENSITIVITY REACTIONS: NSAIDS
General considerations
Non-allergic hypersensitivity reactions refer to adverse drug reactions that are not mediated by specific immunological mechanisms, this is IgE or T cell dependent responses. This group of reactions is commonly described as intolerant, pseudoallergic, or idiosyncratic reactions although the term non-allergic hypersensitivity is actually used for integrating all these terms.13 The most representative group of drugs is made by NSAIDs.12,114 These are medicaments of variable chemical composition that antagonize inflammation by interfering with the function of cyclooxygenases. Cyclooxygenases are enzymes that participate in the conversion of arachidonic acid into prostaglandins and thromboxanes, which generate strong mediators of the inflammatory process. This inhibition results in a shunting of arachidonic acid metabolism toward the 5-lipoxygenase pathway, resulting in the increased release of cysteinyl leukotrienes and a decreased production of prostaglandin E2 mediators that could be involved in the pathogenesis of these reactions.11,115,116
NSAIDs are responsible for 21%-25% of reported adverse drug events which include immunologic and non-immunologic hypersensitivity reactions.11 A recent study indicates that these figures are even higher.117 Depending on the timing, symptomatology and putative mechanism of the reactions there are several subtypes of hypersensitivity to NSAIDs.115,118,119 The following categories are actually recognised:
NSAID-exacerbated respiratory disease presently designated as aspirin-exacerbate respiratory disease.
NSAID-exacerbated cutaneous disease, in particular, urticaria and angioedema in patients with chronic idiopathic urticaria. In analogy to aspirin-exacerbate respiratory disease, it could be called NSAID or aspirin-exacerbated cutaneous disease.
Multiple NSAID-triggered urticaria, angioedema, and anaphylaxis in patients without other underlying disease.
Urticaria, angioedema, and anaphylaxis induced by a single NSAID. In turn these can be divided into IgE or T cell dependent reactions.120
Diagnosis
Because it is estimated that in the 70% of cases with NSAID hypersensitivity non-specific immunological mechanism are involved,12 only in 1/3 of the cases will be theoretically possible to apply in vivo or in vitro specific immunological tests based on the capacity of IgE or T cells. For this, the in vitro test has focused on the mediator release determination.121-123 The capacity for histamine release or other mediators such as leukotrienes or ECP from eosinphils has been used for the development of in vitro assays. Although extensive research has been made these tests cannot be recommended for routine diagnosis.124 These are outlined below.
Basophyl activation test (BAT)
As basophyls can be activated by both specific and non-specific mechanisms and since their involvement has been demonstrated in this type of reactions,128 the measurement of cell surface molecule CD63 upon in vitro drug challenge has been proposed for in vitro diagnosis of aspirin-exacerbate respiratory disease.123 However low sensitivity and specificity were variable with no firm conclusion on the use of this test for the diagnosis has been provided.70
Challenge tests
In patients with a history of reaction to a single NSAID and no additional exposure to a second NSAID, skin testing is possible and may reveal a selective sensitization, although until now it has been shown in a very low number of cases and only with some drugs like pyrazolones.12,18 IgE tests are not commercially available.11,18,129 It may be convenient to confirm the diagnosis by oral challenge, although this should be done cautiously because low concentrations of the drug may already cause symptoms. If the results are positive, another NSAID of a different chemical group should be tested to demonstrate cross-response.130 A history of systemic anaphylaxis would be a contraindication to perform the provocation tests with the incriminated drug.12,131
The oral provocation test is the "gold standard" for the diagnosis, although it should not be performed during an urticaria or airways exacerbation. According to the EAACI/GA2LEN guideline,132 subjects should be challenged under single-blind, placebo-controlled conditions, after at least 1-2 weeks without any skin eruptions. Acetyl-salicylic acid challenges are recommended to be done during two consecutive days, administering on the first day 4 capsules of placebo and on the second day exponentially increasing doses of acetyl-salicylic acid (71, 117, 312, and 500 mg) at 1.5-2 hour intervals, up to a cumulative dose of 1,000 mg of acetyl-salicylic acid. The challenge procedure is interrupted, if cutaneous reactions appear or when other symptoms of NSAID hypersensitivity develop. Challenge protocols for NSAIDs other than acetyl-salicylic acid are available in the literature.132 Most patients react to doses of acetyl-salicylic acid between 325 and 650 mg, and the time interval between acetyl-salicylic acid intake and onset of hives is generally no longer than one hour. The sensitivity of challenge is not 100%; in fact negative results of challenges with the suspected NSAIDs have been reported, even in cross-reactors.133
HYPERSENSITIVITY REACTIONS TO BIOLOGICAL AGENTS
General considerations
Biological agents are new medicaments with increasing applications that are progressively implicated in hypersensitivity reactions.6 They are not synthetic organic chemicals (xenobiotics) being structurally similar to autologous proteins. Different mechanisms have been proposed to be involved in the reactions induced by these agents that have been reviewed in detail elsewhere.134 Because many of them affect inflammatory processes, the immune effect can be induced by their activities; however, they can produce true allergic reactions mediated by specific immunological mechanisms.6,134 Amongst the biological agents considered within this group are cytokines, antibodies against cytokines, receptors, cell surface markers and fusion proteins as cytokine receptors or cellular ligands.6
Reactions induced by these agents belong to all the different immunological mechanisms described in the classic reactions by Gell and Coombs.7 Anaphylactic reactions,135-138 cytotoxic reactions like immune haemolytic anaemia and thrombocytopenia,88,89 immune complex like diseases139-143 and T cell responses144-146 have been reported. We will refer in more detail to Type I and Type IV reactions.
The ability of these reagents for inducing true allergic reactions is related with their ability of being recognised as different by the immunological system. Thus chimeric antibodies (ended by -ximab, are more immunogenic than those partially (-zumab) and whole humanises (-mumab).84 The best studied model is cetuximab, an antibody used for treating different neoplasias.147 It has been shown that many of these patients are primarily sensitised to a carbohydrate, α-Gal present in different natural sources as meat or induced after tick bites.148,149 In the case of non-immediate reactions from mild to severe responses to these agents have been reported indicating that these have been recognised by T cells which are involved in the response.146
Common reactions induced by these drugs are fever, chills, nausea, vomiting, headaches and diarrhea that sometimes may mimic an allergy reaction.149 But these usually may appear after the first administration and are often controlled by symptomatic medications. In the case of anaphylactic reactions these usually appear after several therapeutic courses and can be often severe and potentially fatal.
Diagnosis
Because these medicaments are proteins it is not difficult to work with them both in vivo and in vitro for the diagnostic evaluation. Different studies have shown positive skin tests136,147-149 and in vitro specific IgE antibodies for immediate reactions136 and also T cell responses.144 The general principles outlined in this section are valid for approaching to these patients if specific immunological mechanisms are the responsible of the reactions.6,7
MONITORIZATION OF THE ACUTE RESPONSE
The progress in molecular biology and genetics has enable to monitor the acute response and define to what extent Type I or Type IV reactions occur in more detail.76 This approach is not new but has been recently refined.76 Although the boosted IgE response after an anaphylactic reaction can be monitored149 the most useful is the quantitation of classical mediators for immediate reactions like histamine/histamine metabolites and tryptase.150 The first can be determined in peripheral blood or as N-methyl histamine metabolite in urine or other body fluids like nasal lavage and the second in peripheral blood or affected organ because as a protein it is not excreted in urine.150-152 For their evaluation it is very important to take the sample at the optimal time of release. Histamine peaks only for few minutes in peripheral blood150,151 but a clearance in urine show a peak at 3-5 hours after the episode that normalised in the subsequent 24 hours. On the contrary tryptase after being released in the affected organ pass to peripheral circulation with an optimal peak during the 2-4 hours following the acute episode that further returns to normal levels in a maximum of 24 hours.151 Release of these mediators is compatible with an acute immediate reaction but it is not exclusively for an IgE mechanism since these can be also released in NSAIDs cross intolerance as well as other responses.11
Very often in allergic reactions it is not clearly known which is the specific immunological mechanism involved. This is particularly relevant for T cell mediated reactions.76 Therefore the monitorization of T cell dependent reactions has shown an increase in IFN-γ and the transcription factors T-bet with a down regulation of IL-4 and GATA 3, which is indicative of aTh1 response.153 On the contrary in IgE mediated reactions the opposite was observed with a polarised pattern of response toward a Th2 with up-regulation of IL-4 and GATA-3 and a down regulation of IFN-γ and T-bet that normalised as reaction subsides.153,154
The monitorization can be carried out not only in peripheral blood but also in skin, the organ mainly involved in non-immediate drug reactions, showing a parallelism between the results found in the two compartments with the participation of different T cell subsets depending on the clinical entity.154 Studies in more detail have shown that skin homing receptors78,155 were increased in both peripheral blood and skin whereas the corresponding chemokines ligands were expressed only in skin. In this work it was observed an increase in CCR6 and CCR10 with their corresponding ligands CCL20 and CCL27 responsible for skin homing and CXCR3 with its corresponding ligands CXCL9 and CXCR10 related with a Th1 response in cases with maculopapular exanthema.155 This integrated approach can be more deeply studied with a complete view of the genetic expression by DNA microarrays.156 The determination of the different markers involved in drug allergic reactions can be crucial for discriminating from virus diseases with similar clinical manifestations although different immunological mechanism are underlying.157
CONCLUDING REMARKS
In spite of the difficulties for the immunological evaluation of HDR, increasing interest and progress has been made in the last years that has enabled a better understanding and management of HDR. In the cases of IgE mediated reactions, betalactams continue to be the drugs most frequent involved, being side chain penicillin determinants like amoxicillin needed both in vivo and in vitro in the immunological evaluation. Other drugs can also induce IgE mediated reactions, being fluorquinolones a group of antibiotics with increasing relevance. Although experimental prototypes have been developed for the determination of specific IgE antibodies to many drugs, the BAT is an assay quite useful for identify the culprit drug. In the case of non-immediate reactions, the number of entities is greater than in immediate reactions and the way how T cells and cells of the innate immune system interact followed by a specific recruitment of effector T cells to the affected organ is better known actually. The progress made in molecular biology and genetics is contributing to these advances. Monitorization of the acute response in non-immediate reactions offers great promises.
Concerning NSAIDs increasing evidence is showing that these are the most relevant group of medicaments involved in adverse drug reactions, with a non-immunological mechanism involved in the higher proportion of patients. These are designated as hypersensitivity reactions with absence en allergic mechanism and patients are cross-intolerant, reacting to different NSAIDs non-chemically related. Because there are no in vivo or in vitro tests for the diagnosis, the immunological evaluation in these cases required a drug provocation test to establish the diagnosis of cross-intolerance, selective responder or tolerant cases.

 XML Download
XML Download