

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Correct use of inhaler devices is fundamental to effective asthma management but represents an important challenge for patients. Both bronchodilator reliever therapy (short-acting β2-agonist [SABA]) and most asthma controller (preventer) therapies, including inhaled corticosteroids (ICS) and long-acting β2-agonist (LABA), are delivered by inhalation. Numerous clinical investigations report errors in inhaler device handling by patients, even by those classified as experienced in using their asthma inhalers.1-4 Inhaler mishandling, in turn, has been linked to reduced asthma control, with increased risk of exacerbations and unscheduled care for asthma.1,5
The correct inhalation manoeuvre differs for different inhaler types.6-9 Pressurised metered-dose inhalers (pMDIs) are actuated by pressing down on the canister to release a dose in coordination with the start of inhalation. Breath-actuated metered-dose inhalers (BAIs) and dry powder inhalers (DPIs) are actuated by the patient's inhalation but vary in requirements for inhalation speed and character, which should be slow and deep with a BAI but sharp and rapid with a DPI.
Because of these differences, several authors have recommended that patients should always be prescribed the same device type for each asthma medication.7-11 It would seem logical that confusion could result from using different inhaler device types for asthma controller and reliever therapy, especially for patients just beginning inhaler therapy who lack long-term training and practice with different devices. However, there is actually little definitive research into this topic. In their observational study of 321 adult outpatients with asthma, van der Palen and coauthors12 used a check-list to assess inhaler technique and found no errors among 71% of patients using only one inhaler as compared with 61% of patients using two or more different inhalers. They concluded that the same type of inhaler should be prescribed and that if this is not possible then a combination of two different DPIs is preferable to a DPI-pMDI combination. They did not examine asthma control in relation to inhaler technique, nor, to our knowledge, have other studies investigated this.
Retrospective database studies can be used to examine the comparative effectiveness of interventions for real-world patients under real-world conditions of clinical care. Our objective in this study was to determine whether outcomes differed for primary care patients in the UK who were prescribed the same BAI device for asthma controller and reliever therapy as compared with mixed devices (BAI plus pMDI). We focused on BAIs, as these are often used for controller therapy but not always in conjunction with a breath-actuated reliever because the latter is more expensive than a SABA pMDI.
MATERIALS AND METHODS
Data source and patients
This retrospective observational study drew on anonymised patient data contained in the General Practice Research Database (GPRD), a large primary care database containing prescription and other medical record information for patients at over 500 participating clinical practices throughout the UK.13 The GPRD is a well-regarded and validated data source for pharmacoepidemiologic research, including respiratory and prescribing research.14-18
This study analysed data for patients with asthma aged 4-80 years who received beclometasone dipropionate by Easi-Breathe BAI as their first ICS prescription, together with a prescription for reliever therapy (salbutamol) by either Easi-Breathe BAI or pMDI. These particular combinations allowed for comparability of formulation and drug, as salbutamol pMDI and BAI contain a pressurised aerosol with similar characteristics and the only difference being between the breath actuation amendments. Evidence of asthma in the database was defined as a coded diagnosis of asthma, two or more prescriptions for asthma at different timepoints during the baseline year, or two or more prescriptions for asthma during the outcome year that included at least one ICS prescription. Patients over 60 years old who smoked were excluded from the study to minimise inclusion of patients with concomitant chronic obstructive pulmonary disease (COPD). In addition to COPD, other exclusion criteria were any other chronic respiratory disease, a prescription for asthma controller therapy (ICS or LABA) during the baseline year, or a LABA prescription at the index date.
The study period spanned 16 and a half years from January 1991 through June 2007, a period when all devices of interest were available. As SABA is not always prescribed on the same day as ICS, we prioritised as follows to identify each patient's salbutamol device for the study: (1) the salbutamol prescribed at the index date; (2) the salbutamol prescribed at the closest date before the index date; or (3) the first salbutamol prescribed after the index date if there were no recorded prescriptions before the index date. Eligible patients were required to have 2 continuous years of data in the GPRD, including a baseline year for confounder definition and an outcome year, and to be enrolled at practices with data assessed as up-to-standard by the GPRD during the years in question.
Effectiveness endpoints
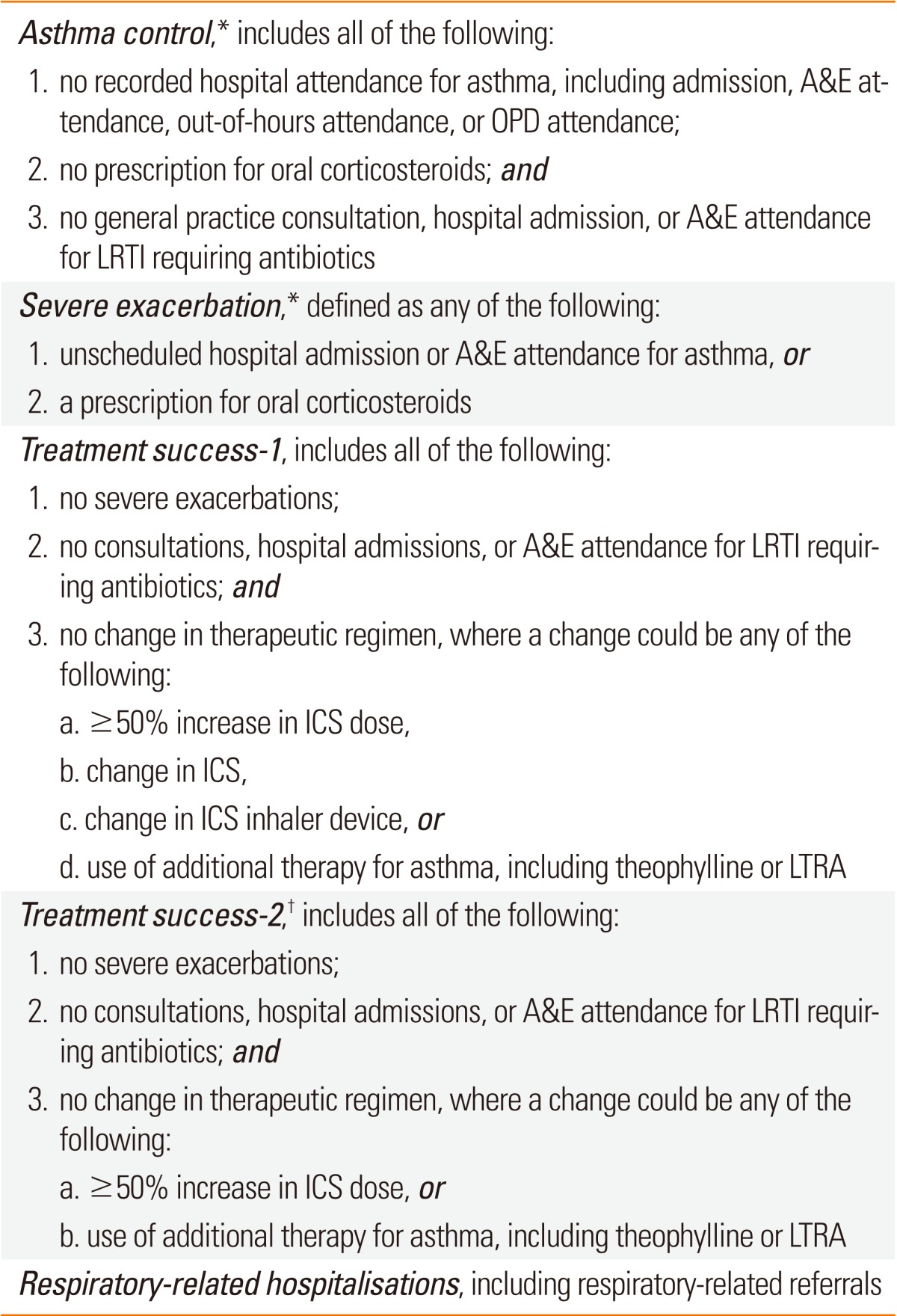
The co-primary endpoints, defined in Table 1, were designed to capture evidence of asthma control and rate of severe exacerbations during the outcome year, in accordance with recommendations of the joint European Respiratory Society/American Thoracic Society Task Force on outcome measures for asthma trials.19
Secondary endpoints included two composite measures of treatment success and the rate of respiratory-related hospitalisations (Table 1).
Statistical analyses
Summary statistics were used to assess all baseline and outcome variables. Continuous variables were compared using the t test for normally distributed data and the Mann-Whitney test (Wilcoxon rank sum test) for skewed data; categorical variables were compared using the χ2 test. Differences between treatment cohorts with P<0.10 were examined for collinearity as well as clinical importance to select those used as potential confounders in the regression modelling of outcomes.
Multivariate analyses were used to identify baseline variables predictive (P<0.05) of outcomes; these were considered as potential additional confounders when modelling outcome variables. Spearman correlation coefficients were calculated between all potential confounders to determine strengths of linear relationships between variables; the correlation coefficients were considered, in conjunction with clinical interpretation, to identify possible collinearity issues. All outcomes were adjusted for appropriate non-collinear baseline confounders.
The adjusted odds of achieving asthma control was compared between treatment cohorts using a binary logistic regression model. Asthma control status was used as the dependent variable with treatment and potential confounding factors as explanatory variables. The same model was used to assess other binary outcomes. A Poisson regression model was used to compare the total number of severe exacerbations in the outcome period between treatment cohorts and to obtain estimates of exacerbation rates. The model was adjusted for over-dispersion using robust standard errors, and adjustments were made for potential baseline confounders. This model was used also to analyse respiratory-related hospitalisation rates.
Study endpoints and the main analyses were established a priori according to standard operating procedures of the study group.20 We also performed a post hoc sensitivity analysis to explore differences in odds of asthma control and severe exacerbation rates after excluding children (ages 4-11) as well as patients receiving the highest doses of ICS at the index date.
Adjusted odds ratios and rate ratios were calculated together with 95% confidence intervals. Statistical significance was defined as P<0.05 and trends as 0.05≤P<0.10. All analyses were carried out using SPSS/PASW versions 17 and 18 (SPSS Statistics, IBM, Somers, NY, USA), SAS version 9.2 (SAS Institute, Marlow, Buckinghamshire, UK), and Excel 2007 (Microsoft, Bellevue, WA, USA).
RESULTS
Patients
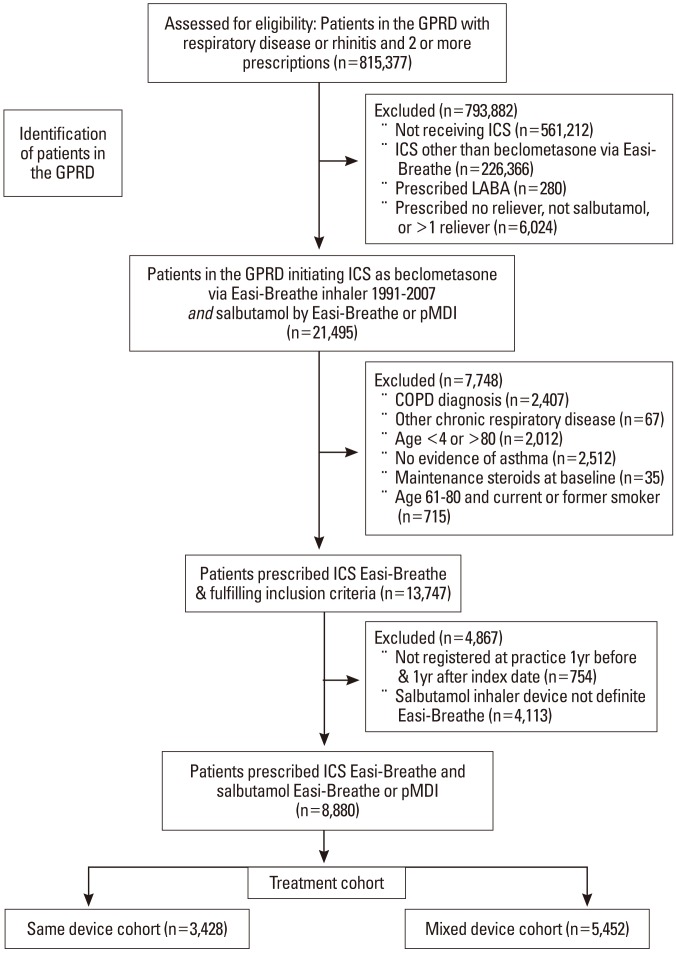
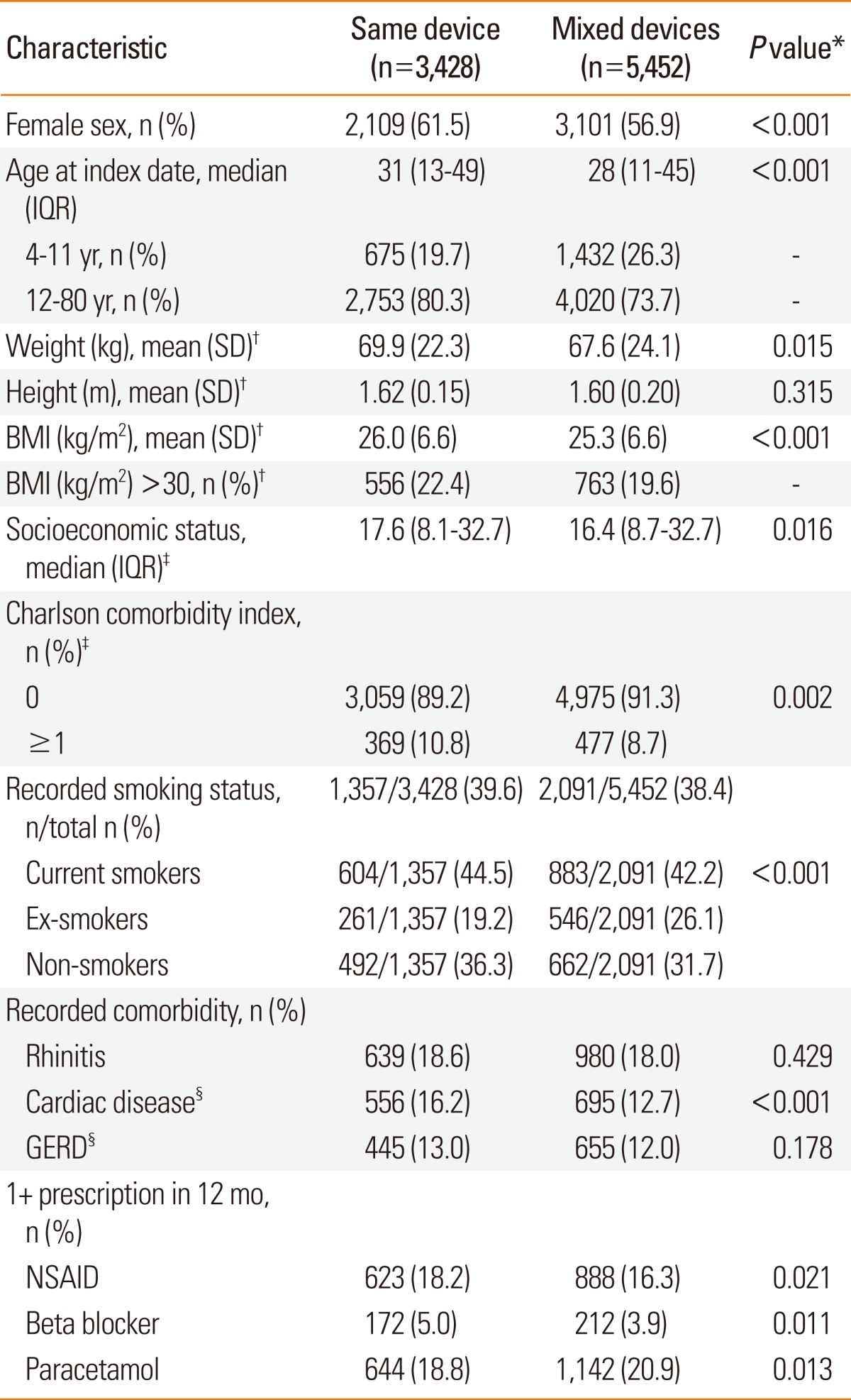
We identified 8,880 patients who met study selection criteria: 3,428 in the same device cohort (who received Easi-Breathe inhalers for both beclometasone and salbutamol) and 5,452 in the mixed devices cohort (who received beclometasone by Easi-Breathe and salbutamol by pMDI). Fig. 1 depicts the patient selection process, and Table 2 summarises patient characteristics at the index date. Approximately one quarter (2,107 or 23.7%) of patients were children aged 4-11 years. Of these, 45% were girls, whereas in the full cohort, 59% were female. The mean year of the index date was 1999 in both cohorts.
There were several statistically significant differences in demographic characteristics between the cohorts at baseline (Table 2), with proportionately more female patients and more current smokers in the same device cohort. The median age was higher in the same device cohort, and patients were heavier with somewhat higher BMI.
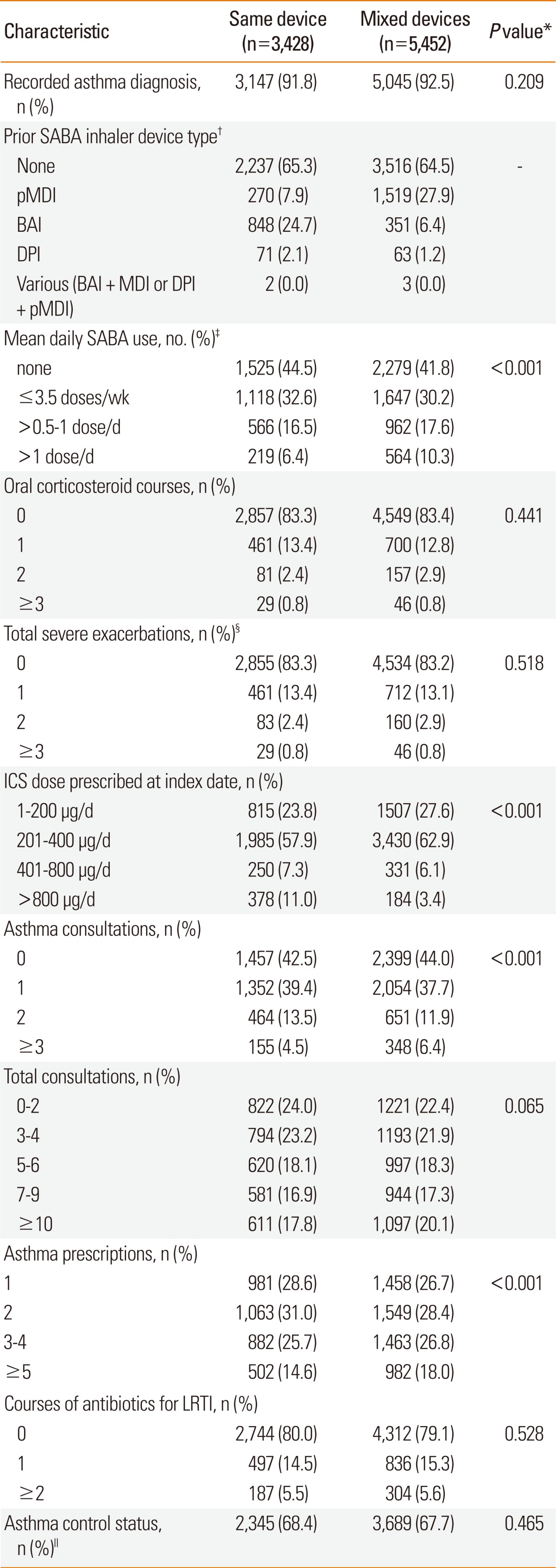
During the baseline year, the proportions of patients in each cohort who met study criteria for the asthma control measure were similar, as were those who had experienced a severe exacerbation (Table 3). Patients in the mixed devices cohort were more likely to have received paracetamol, a higher SABA dose, and more asthma prescriptions than those in the same device cohort during the baseline year (Tables 2 and 3).
At the index date, the median (IQR) prescribed ICS doses were 400 (400-400) µg and 400 (200-400) µg in the same device and mixed devices cohorts, respectively (P<0.001). There were more patients in the same device cohort who received a high ICS dose (>800 µg/day; Table 3). Of the patients with known height and weight who were prescribed doses >800 µg/day, the proportions who were obese (body mass index ≥30 kg/m2) were similar in the two cohorts, namely 82/327 (25.1%) and 37/153 (24.2%).
Outcomes
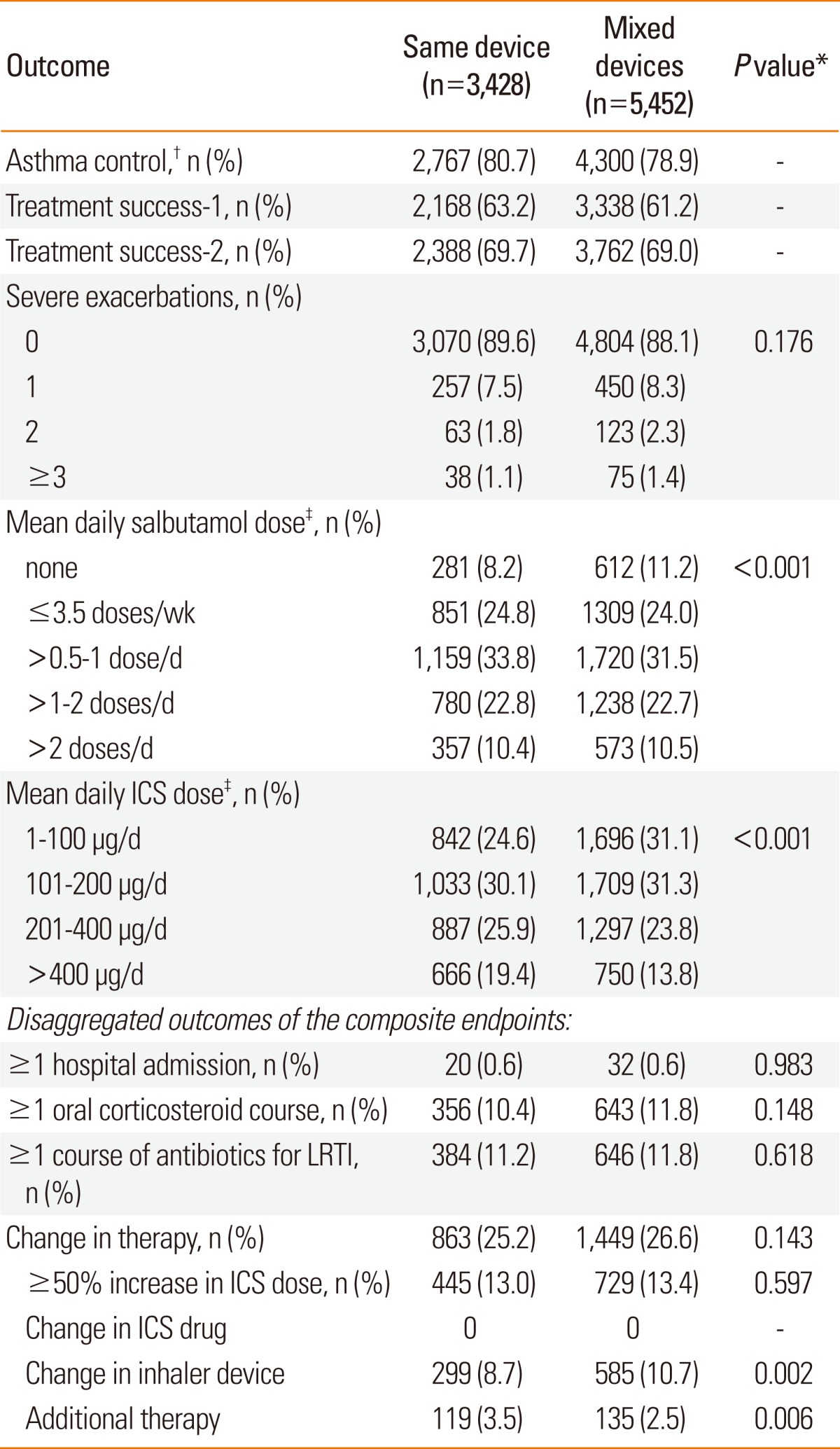
There were several statistically significant differences between cohorts in the unadjusted outcomes, summarised in Table 4. More patients in the same device cohort consumed a mean daily ICS dose of >400 µg/day, and fewer used no SABA, during the outcome year, as compared with patients in the mixed devices cohort. (The daily ICS and salbutamol doses consumed during the outcome year were calculated as the dispensed amount divided by 365.) The median (interquartile range [IQR]) dose of ICS consumed during the outcome year was 164 µg/day (110-329) for patients using the same device versus 137 µg/day (55-274) for patients using mixed devices (P<0.001). The median (IQR) salbutamol doses were the same in both cohorts, namely, 110 µg/day (55-219; P=0.638). Additional therapy was more likely to have been prescribed in the same device cohort, while a change in ICS device was more likely in the mixed devices cohort (Table 4).
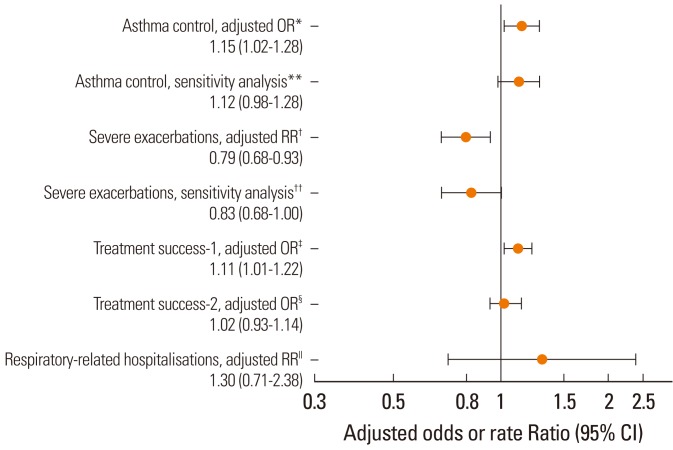
Patients in the same device cohort were significantly more likely to achieve asthma control during the outcome year, and they experienced a significantly lower rate of severe exacerbations, than those in the mixed devices cohort (Fig. 2). Moreover, treatment success-1 was significantly more likely for patients in the same device cohort. There were no differences between cohorts in the adjusted odds for treatment success-2 or in the adjusted rate of respiratory-related hospitalisations (Fig. 2).
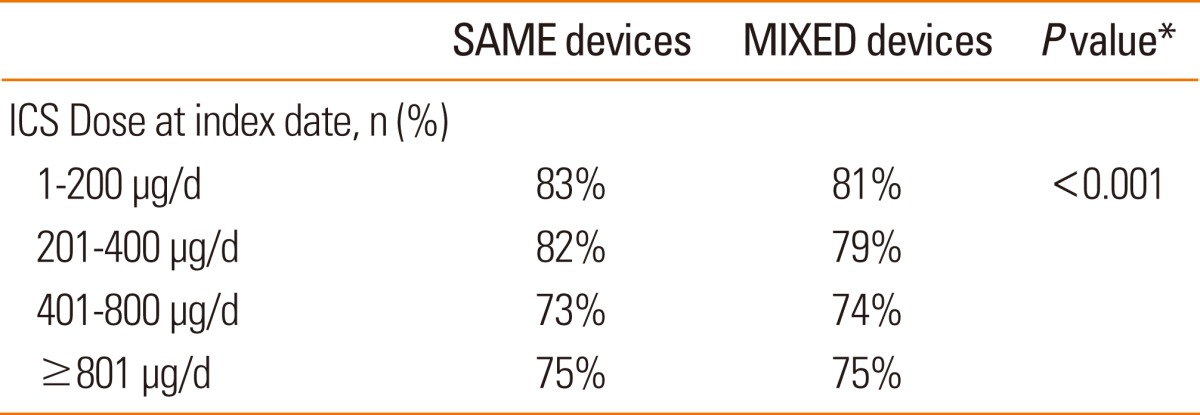
Because of recorded differences between cohorts in both prescribed ICS dose at the index date and ICS dose consumed over the outcome year, we examined the percentage of patients who achieved asthma control according to index date ICS dose. The differences between cohorts in asthma control were evident at the lower ICS doses, whilst at the higher ICS doses the percentages of patients achieving control in each cohort were similar (Table 5).
In a post hoc sensitivity analysis of the asthma control and severe exacerbation endpoints, we excluded 1) patients prescribed >800 µg/d at the index date (patients prescribed a high ICS dose were more numerous in the same device cohort) as well as 2) children younger than 12 years (there were fewer patients under the age of 12 in the same device cohort). With these exclusions, differences in asthma control and severe exacerbation rates were no longer significant but showed a strong signal supporting the main analyses, with higher odds of asthma control in the same device cohort than in the mixed devices cohort (Fig. 2).
DISCUSSION
The results of this retrospective observational study indicate that over 1 year after a first ICS prescription, patients prescribed the same inhaler device type for both ICS controller and salbutamol reliever therapy were significantly more likely to achieve asthma control than those prescribed mixed devices. Moreover, patients prescribed the same inhaler device type had a significantly lower recorded rate of severe exacerbations requiring a hospital visit or oral corticosteroid course, as well as higher odds of treatment success after incorporating changes in therapeutic regimen. The two treatment cohorts had comparable rates of respiratory-related hospitalisations and odds of treatment success after excluding changes in therapeutic regimen that could be driven by cost savings.
A small proportion of patients in the same device cohort were prescribed a higher ICS dose at the index date than those in the mixed devices cohort, and the median ICS dose consumed during the outcome year was significantly higher in the same device cohort. However, we believe it unlikely that ICS dose influenced outcomes in favour of the same device cohort. Firstly, the sensitivity analysis that excluded patients prescribed high doses of beclometasone (>800 µg/day) and paediatric patients (ages 4-11) supported the main analyses. Secondly, the differences between treatment cohorts in the proportion of patients achieving asthma control were driven by patients receiving the lower ICS doses (similar proportions of patients achieved asthma control in the higher ICS dose categories).
The problem and prevalence of incorrect inhaler use have been the subject of several reviews over the last decade.7-9,21 Proposed solutions to this problem include educating health-care providers about different inhaler device characteristics; individualising inhaler selection; accommodating patient preferences with regard to their inhaler device; reinforcing inhaler technique at each visit; using tools for training and checking technique; and avoiding a switch in ICS device without an accompanying consultation.9,22,23 The results of this study suggest an additional solution, namely, that, when possible, patients-especially those initiating ICS therapy-should be prescribed the same type of device for their asthma controller and reliever therapy.11
We can speculate why patients prescribed the same device type had better outcomes. Specifically, because both ICS drug and device were the same in both cohorts, and the SABA formulations in the two devices are the same, it is reasonable to conclude that the findings likely relate to the impact of salbutamol inhaler device choice. However, it is the ICS that influences asthma control and future risk of asthma exacerbations; SABA does not determine asthma control. Therefore, the outcomes in this study most likely result from the effect on ICS inhaler technique of mixing devices, very possibly because the need to use different breathing patterns with the two devices adversely impacted ICS inhaler technique.
The strengths of this study include the large patient population and the 1-year outcome period, which allowed us to examine less frequent outcomes such as hospitalisations and minimised the influence of seasonal changes in asthma and allergies. The GPRD is an established source for primary care data and draws from a geographically and socioeconomically diverse population; this improves the generalisability, or applicability, of study results to real-world clinical practice. We note that the prescribing patterns recorded in this study were rational, namely, as the ICS dose increased, the percentages of patients meeting the study asthma control measure decreased, suggesting that higher doses were prescribed for patients with more difficult asthma.
While there were some differences between study cohorts at baseline, the two cohorts were comparable in terms of baseline asthma control and severe exacerbations. Moreover, the effectiveness analyses adjusted for differences between cohorts determined to be potential confounders. For example, at baseline the mixed devices cohort was more likely to use more SABA and to have more asthma prescriptions; however, neither of these variables had a significant effect on the asthma control outcome and thus were omitted from the final model. Instead, for the severe exacerbation outcome, the model was adjusted for baseline differences in asthma prescriptions.
The composite asthma control endpoint was designed to capture indicators of asthma control that would be recorded in the GPRD, including unscheduled asthma care and hospitalisations, oral corticosteroid prescriptions, and antibiotic prescriptions for lower respiratory tract infection, as in real-world practice asthma exacerbations can be confused for acute respiratory infections.24,25 There were some significant differences between cohorts in the unadjusted results of the disaggregated outcome measures, including more patients in the same devices cohort who took additional therapy (3.5% vs. 2.5%) and more patients in the mixed devices cohort who had a change in inhaler device (8.7% in same devices cohort vs. 10.7%) and overall with a change in therapy (25.2% same devices vs. 26.6% mixed devices cohort); however, these differences were small and unlikely to be clinically significant.
Study findings should be interpreted with an understanding of potential study limitations, common to observational studies. These include the potential for unrecognised confounding factors, including selection bias. Moreover, while the GPRD is recognised to be a high-quality database, there were missing data for some patients, including smoking history, that could influence outcomes. The smoking status was more likely to be recorded for patients with more difficult disease (i.e., those not achieving asthma control), a possible explanation for the high recorded smoking prevalence (-43%) among the 40% of patients with recorded smoking history. While there is no assurance that patients actually took the medications as prescribed and dispensed, it is unlikely there would be differences between cohorts in this parameter that could bias the results. In the UK, the pharmacist must dispense as prescribed by the physician, and the GPRD prescribing data are considered a reliable proxy for dispensed medications.14,26 Finally, the consistency of the outcomes, including the sensitivity analyses, provide support for the overall findings.
In conclusion, we found that patients prescribed the same BAI device for both controller ICS and reliever salbutamol therapy had better odds of asthma control and lower risk of severe exacerbations over 1 year after their first ICS prescription than those prescribed a BAI for ICS and a pMDI for salbutamol. These findings suggest that, when possible, the same device should be prescribed for both ICS and reliever therapy when patients are initiating ICS. The devices we studied are relatively similar, and it is possible that the adverse effects of mixing other device types, such as DPIs and pMDIs, might be greater. Further research is needed to investigate asthma-related outcomes with other potential inhaler device combinations and whether consistent device prescribing is optimal also for other inhaler device types.
 XML Download
XML Download