

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Allergic diseases are multifactorial and induced by a combination of genetic and environmental factors.1,2 Atopic dermatitis (AD) is more strongly related to food allergens in children than in adults.3 In pediatric patients with AD, the major food allergens include egg white, cow's milk, soybean, wheat, and peanut.4 Food allergies manifest various symptoms in the skin, gastrointestinal tract, and airways as a result of adverse responses to a food protein via IgE-mediated or non-IgE-mediated immune mechanisms. Allergic reactions to food present as both acute and chronic inflammation due to cellular responses activated through specific IgE against the food allergen.5
The basic principle in the treatment of food allergies is the avoidance of the allergen. AD associated with food allergy can be successfully controlled with meticulous skin care, drug therapy, and the restriction of foods containing sensitized allergens.6 However, the restriction of food consumption can lead to nutritional deficiency, and thus for normal body growth and the prevention of disease, a nutritional balance must be achieved through the intake of alternative foods.7-9 Additionally, malnutrition owing to food avoidance results in weight loss and damage to the immunomodulatory system, which subsequently exerts a negative effect on the progress, treatment, and prognosis of disease.10 It has been reported that some pediatric AD patients are short,11 and growth retardation such as short height or low body weight has been reported in patients with AD.12 Previous studies have reported the occurrence of nutritional problems related to food allergies, including kwashiorkor,13 rickets,14 and marasmus,15 in infants with AD, following food restriction.
In addition, because they are in an active growth phase, pediatric AD patients with food allergies are at particularly high risk for developing growth retardation and nutritional deficiency; these patients require careful management for growth and nutrition.16 Therefore, this study investigated both growth and nutritional status according to the number of sensitized food allergens in infants and young children with AD.
MATERIALS AND METHODS
Subjects
This study included a total of 165 children between the ages of 5 and 47 months who were diagnosed with AD according to the diagnostic criteria proposed by Hanifin and Rajka17, by pediatricians at our clinic.
Anthropometric assessment
For children aged <24 months, the height and weight were measured with the child in a recumbent position, with the shoes off, and with a light top on, using an automated height and weight measuring instrument. For children aged ≥24 months, the height and weight were measured to 0.1 cm with the child in a standing position, with the shoes off, and with a light top on, using an automated height and weight measuring instrument. The normal values of Korean children and adolescents proposed by the Korean Pediatric Society in 2007 were used as reference values. The growth and nutritional status were evaluated using the z-scores of the World Health Organization.18 Weight for age, height for age, and weight for height are expressed as z-scores in standard deviation units. A weight for age, height for age, or weight for height z-score of less than -2 represents moderate to severe undernutrition.19
Biochemical tests
The eosinophil counts obtained by routine blood tests were used as a biochemical marker. Total serum IgE and specific IgE against sensitized food allergens were measured using an ImmunoCAP assay (Pharmacia, Uppsala, Sweden). A specific IgE level of ≥0.7 kUA/L defined sensitization to egg white, cow's milk, soybean, peanut, wheat, and fish. The number of these six sensitized food allergens was calculated for each patient, and the patients were divided into four groups according to the number of sensitized allergens: none (0-allergen group), 1 (1-allergen group), 2 (2-allergen group), and ≥3 (≥3-allergen group).
Assessment of the severity of AD
Following the patient's examination by a pediatrician, the severity of AD was assessed according to the scoring of atopic dermatitis (SCORAD) index.
Statistical analysis
Continuous variables such as age, birth weight, and eosinophil counts are expressed as means±SD. One-way ANOVA was applied to compare the differences in growth and nutritional status according to the number of sensitized food allergens, and Duncan's test was performed for post hoc analysis. The severity, eosinophil counts, total serum IgE, and time of food weaning according to the number of sensitized allergens were adjusted for age, gender, and birth weight. The z-scores were adjusted for birth weight, which was used for partial correlation analysis. All statistical analyses were performed using STATA version 11.0. A value of P<0.05 indicated statistical significance.
RESULTS
Clinical characteristics according to the number of sensitized food allergens
A total of 165 pediatric patients were enrolled in this study. They included 105 boys (63.6%) and 60 girls (36.4%). The patients ranged in age between 5 and 47 months, and the highest number of patients were <1 year old (n=77, 46.7%; data not shown). Overall, the mean birth weight was 3.29±0.40 kg, the mean eosinophil count was 694.00±784.47/µL, and the mean total serum IgE was 194.46±454.49 IU/mL. The mean SCORAD index values according to the number of sensitized food allergens were 24.91±16.02, 29.72±17.54, 26.87±15.41, and 40.37±21.14 for the 0-, 1-, 2-, and ≥3-allergen groups, respectively. As the number of sensitized food allergens increased, the SCORAD index increased (P=0.001). Total serum IgE values were 54.91±80.51, 84.01±111.06, 315.51±596.25 and 467.00±750.55 IU/mL for the 0-, 1-, 2-, and ≥3-allergen groups, respectively, and these values were significantly different (P<0.001). The time of initiating food weaning did not differ significantly among the groups.
The mean z-scores of weight for age, height for age, and weight for height were -0.06±1.03, -0.16±0.90, and 0.05±1.09, respectively. The mean z-scores of weight for age according to the number of sensitized food allergens were 0.21±1.08, 0.02±0.87, -0.14±0.96, and -0.57±1.90 for the 0-, 1-, 2-, and ≥3-allergen groups, respectively, and these scores were significantly different (P=0.006). The z-score of height for age differed significantly (P=0.018) between the 1-allergen group (1.10±0.90) and the ≥3-allergen group (-0.50±1.01). The z-score of weight for height was 0.18±1.03 in the 0-allergen group, 0.08±1.12 in the 1-allergen group, 0.12±0.93 in the 2-allergen group and 0.28±1.24 in the ≥3-allergen group (P=0.286) (Table 1).
Number of sensitized food allergens and age distribution
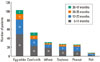
The mean number of sensitized food allergens per patient was 1.47±1.68. The most frequently sensitized food allergen was egg white, followed by cow's milk and wheat. A sensitization to egg white occurred most commonly in patients aged <1 year (n=48, 47.1%), followed by cow's milk (n=22, 42.3%) (Figure).
Correlation between the number of sensitized food allergens and clinical characteristics
Following the adjustment for age, gender, and birth weight, the number of sensitized food allergens significantly correlated with the SCORAD index (r=0.308, P=0.002), time at which food weaning began (r=0.332, P=0.001), eosinophil counts (r=0.266, P=0.009), and total serum IgE (r=0.394, P<0.001) (Table 2).
Correlation between the number of sensitized food allergens and z-scores
Following the adjustment for birth weight, the number of sensitized food allergens significantly correlated with the z-scores of weight for age (r=-0.358, P<0.001), height for age (r=-0.278, P=0.001), and weight for height (r=-0.224, P=0.006) (Table 3).
DISCUSSION
AD is a common chronic inflammatory skin disease in children. This disease shows a significant correlation with food allergies and thus can exert a negative effect on growth and nutritional status in children who are in an active growth phase. In this study, both weight (a predictor of short-term nutritional status) and height (a predictor of relatively long-term nutritional status) significantly decreased according to the number of sensitized food allergens, and the time of initiating food weaning showed an increased delay as the number of sensitized food allergens increased. Given the negative correlations between the number of sensitized food allergens and the z-scores of weight and height for age, it is conceivable that sensitization to a food allergen can affect both growth and nutritional status in infants and young children.
It has been reported that the height for age percentile and the consumed dietary food intake are significantly less in children with two or more food allergies compared to those with a single food allergy.20 We can successfully restrict food allergens in patients by completely restricting foods that contain the offending allergens, in combination with nutritional supplementation.21 However, passive permeability of the small intestine is increased in some patients with atopic eczema,22 and continuous food restriction may increase the body's metabolic requirements.23 In particular, the requirements for energy and protein may be increased in children with AD, as energy and protein are needed for skin regeneration to compensate for the loss of skin components in AD.7 In addition, the rapid growth and high metabolic rate in infants and young children demand more nutrition per kg of body weight than that needed in adults. Previous studies have reported that growth retardation occurs during a 1-year period24 and that height is decreased more severely in children with AD than in healthy children, despite improved nutritional intake in children with AD.25 In the present study, although we could not verify a causal relationship between food restrictions and growth retardation, our results suggest a correlation between the number of sensitized food allergens and long-term/short-term nutrition and growth. Thus, adequate treatment and continuous management of growth and nutrition are crucial in infants and young children with AD.
The major sensitized food allergens are egg white, cow's milk, soybean, wheat, and peanut, all of which are important sources of protein and energy. In this study, the food allergens with the highest rates of sensitization were egg white followed by cow's milk, as in previous studies.26-29 The rates of sensitization were particularly high in infants. Low calcium intake and high risk for growth retardation have been reported in children sensitized to multiple food allergens, including cow's milk.20 Beginning at 6 months after birth, the iron reservoir continues to be depleted, while the iron requirements for rapid growth are increased at this age.30 Thus, in children who have restricted intake of cow's milk and egg white, an appropriate supply of alternative foods should be provided to meet the recommended requirements for protein and calcium.7
In the present study, the number of sensitized food allergens significantly correlated with the number of eosinophils, total IgE levels, and the time at which food weaning was initiated, as previously reported.29,31,32 Food weaning is typically initiated at the age of 4 to 6 months, depending on the development status of the infant.33 Although it has been recommended that AD-prone infants begin weaning after the age of 6 months, there is still no definitive evidence that this prevents the occurrence of AD.34 In our study, we observed that the initiation of food weaning was increasingly delayed as the number of sensitized food allergens increased. Based on reports that the prevalence of food allergies is higher at younger ages, many parents of children with AD regard food allergy as the main cause of the AD, and hence hesitate to begin weaning or eliminating foods containing major food allergens without a definitive diagnosis. When allergic tests in a child are positive for egg white or cow's milk, the parents tend to restrict this food without any supplementation, resulting in an inadequate nutritional intake.23 However, up to the age of 1 year, food-related problems can occur in children in the absence of food allergies.35 Thus, we should avoid unnecessary food restrictions by keeping in mind that not all food-related symptoms occurring during the food weaning period are attributable to food allergy. In all infants with AD, it is necessary to begin weaning foods at an appropriate time while simultaneously providing foods to satisfy growth patterns and nutritional requirements.
In this study, we could not evaluate growth patterns according to nutritional intake, and any specific food restrictions of the subjects were not verified. Nevertheless, we confirmed that an increased number of sensitized food allergens is associated with negative effects on both short-term and long-term nutritional status and may cause growth retardation. Further studies are required to determine the relationship between nutritional intake, growth, and nutritional status.
In conclusion, the results of this study suggest that food allergies may be a risk factor for growth retardation in infants and young children with AD, and the risk increases with an increase in the number of sensitized food allergens. The meticulous and continuous evaluation and management of both growth and nutritional status should be considered in AD patients with a high number of sensitized food allergens.



 XML Download
XML Download