

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aspirin-exacerbated respiratory diseases (AERD) refers to the development of bronchoconstriction and naso-ocular manifestations in asthmatic individuals following the ingestion of aspirin or other nonsteroidal anti-inflammatory drugs (NSAIDs).1 Recently, aspirin hypersensitivity has attracted a great deal of attention because of its association with increased asthma severity, including life threatening asthma attacks and possible remodeling of both the upper and lower airways.2 Twenty-five percent of asthma patients who required emergency mechanical ventilation were aspirin intolerant.3,4 Aspirin has been the most commonly used medication for pain control or as a prophylactic for primary and secondary prevention of coronary artery disease and other vascular diseases.5 However, AERD remains widely underdiagnosed in the asthmatic population due to insufficient awareness of the relationship of aspirin ingestion and asthma exacerbation. In a multicenter study in 10 European countries including 500 patients, 15% of patients were unaware that they may be susceptible to aspirin intolerance and learned about it only after undergoing provocation tests.6
The diagnosis of aspirin hypersensitivity and AERD is usually obvious from taking a clear history. Patients often have a history of rhinosinusitis and moderate to severe asthma.7,8 AERD typically develops in individuals according to a characteristic sequence of symptoms. Following ingestion of aspirin or certain NSAIDs, patients have an acute asthma exacerbation, typically within 3 hours. Bronchoconstriction can be accompanied by profuse rhinorrhea and periorbital edema. This progresses to recurrent and chronic sinusitis and frequently to nasal polyposis.9 Thus, this syndrome is characterized by the 'aspirin triad' syndrome of aspirin hypersensitivity, bronchial asthma, and nasal polyposis.10 Chronic hyperplastic eosinophilic sinusitis is a fourth hallmark of AERD.1 A fairly limited number of epidemiological studies have offered estimates on the prevalence of AERD. The prevalence of aspirin hypersensitivity in adult asthmatic patients was reported to vary depending on whether it was determined by clinical history alone or by challenge with aspirin.6 Thus, the identification of aspirin hypersensitivity, especially cases not recognized by the patients, is essential to avoid the serious complication associated with this condition.
Diagnosis can be established with certainty only by provocation tests using increasing doses of aspirin. The four commonly used types of provocation tests are defined by the route of aspirin administration: oral, bronchial (inhaled), intravenous, and nasal.11 Oral aspirin challenge (OAC) is the gold standard to confirm the diagnosis. Nasal or bronchial provocation with lysine-ASA may be a valuable alternative diagnostic tool. Both oral and bronchial tests have similar specificity, but the oral test has a somewhat higher sensitivity. However, OAC is a time-consuming procedure, and some cases experience serious complications. Thus, the development of non-invasive methods is necessary for easy diagnosis to prevent unexpected complications associated with aspirin use in susceptible patients. In the present study, we evaluated the diagnostic merits of clinical parameters including the well-known manifestation of aspirin hypersensitivity history and nasal polyposis to predict aspirin hypersensitivity in asthmatic patients.
MATERIALS AND METHODS
Subjects
Seven hundred two asthmatic patients without AERD and 134 subjects with AERD were recruited from the Asthma Genome Research Center, which comprises three university hospitals in Korea. All subjects were Korean and gave their informed consent to participate in the study. All patients were diagnosed by physicians and met the criteria for asthma according to the Global Initiative for Asthma (GINA) guidelines.12 All patients had a history of dyspnea and wheezing during the previous 12 months, plus one of the following: 1) >15% increase in forced expiratory volume in 1 second (FEV1) or >12% increase plus 200 mL following inhalation of a short-acting bronchodilator, 2) <10 mg/mL PC20 methacholine, and 3) >20% increase in FEV1 following 2 weeks of treatment with inhaled or systemic corticosteroids. Twenty-four commonly inhaled allergens were used for a skin-prick test. Total IgE was measured by the CAP system (Pharmacia Diagnostics, Uppsala, Sweden). Atopy was defined as a wheal reaction with a diameter of 3 mm or greater than the reaction to histamine. In the questionnaires designed to reveal the presence of aspirin hypersensitivity, questions related to five specific elements of aspirin hypersensitivity and NSAIDs (dyspnea, wheezing, nasal blockage, skin eruption, loss of consciousness) were incorporated. The asthmatic patients had experienced no exacerbation of asthma or respiratory tract infection in the 6 weeks preceding OAC. OAC was performed in all subjects with increasing doses of aspirin using methods slightly modified from those described previously.13,14 Briefly, patients having a history of aspirin hypersensitivity were given a dose of 30 mg, and those with no history were started on 100 mg of aspirin orally. Symptoms, external signs (urticaria, angioedema, rhinorrhea), blood pressure, and FEV1 were documented every 30 minutes for a period of 2 hours. In the absence of any symptoms or signs suggestive of adverse reaction after 2 hours, 60 mg or 100 mg of aspirin was administered and the same measurements were repeated every hour, with doses of 450 mg given until the patient developed a reaction. If no reaction occurred within 4 hours after the final dose, the test was deemed negative. Aspirin-induced bronchospasms, as reflected by decline (%) in FEV1, were calculated as the pre-challenge FEV1 minus the post-challenge FEV1 divided by the pre-challenge FEV1. OAC reactions were categorized into two groups as follows: 1) a 15% or greater decrease in FEV1 or naso-ocular reactions (AERD), and 2) a decrease of less than 15% in FEV1 without naso-ocular or cutaneous reactions (aspirin-tolerant asthma [ATA]).
A diagnosis of nasal polyps was made based on the presence of endoscopically visible nasal polyps arising from the middle nasal meatus. Chronic rhinosinusitis was diagnosed from patients' documented medical histories and the haziness of the ethmoidal and maxillary sinuses as visualized by a simple X-ray of the paranasal sinuses. The protocols were approved by the Ethics Committee of the Soonchunhyang University Medical Center.
Statistical analysis
Differences in the mean values or frequencies were evaluated with chi square analysis for discrete variables or by independent t-tests for continuous variables. We tested the independent effects of the parameters that showed significant (P<0.01) association with aspirin hypersensitivity using conditional backward logistic regression analysis. The sensitivity and specificity of the parameters were tested using receiver operating characteristic (ROC) curves. All statistical analyses were performed using SPSS version 10.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Comparison of clinical and laboratory parameters between AERD and ATA
A total of 836 subjects were recruited from the asthma cohort. The clinical characteristics of the study subjects are summarized in Table 1. The subjects with AERD had more severe bronchospasm following aspirin challenge as measured by percent decline of FEV1 after OAC (P=1.63×10-34). Significant differences (P<0.01) were found in nine parameters (Table 1): age at diagnosis, body mass index (BMI), FEV1%, PC20, history of urticaria, nasal polyps, chronic sinusitis, and history of aspirin hypersensitivity. Mean age and BMI were slightly lower in subjects with ATA than those with AERD (P=0.01 and P=0.006, respectively). FEV1 and PC20 methacholine were also significantly lower in AERD than in ATA patients (P=1.66×10-7 and P=3.95×10-5, respectively). Subjects with AERD had nearly double the frequency of nasal polyps (61.4% vs. 31.5%, P=1.31×10-8) and chronic sinusitis (72.6% vs. 42.0%, P=8.06×10-9) compared with those with ATA. The history of aspirin hypersensitivity was eight times higher in AERD patients compared with those with ATA (64.7% vs. 8.0%, P=6.81×10-48). The frequency of urticaria history was also significantly higher in AERD patients compared with ATA patients (54.3% vs. 28.11%, P=0.002).
Evaluation of independent effects of clinical parameters on AERD using backward logistic regression analysis
To identify factors affecting the risk of aspirin intolerance, logistic regression analysis with a conditional backward method was used. Among the eight clinical parameters shown to have a P value <0.01 in the comparison between AERD and ATA patients, the presence of nasal polyps, a history of aspirin intolerance, sinusitis, and log [PC20 methacholine] remained significant, and these factors showed a significant association with AERD (P<0.05, Table 2). The ratio of individuals with nasal polyposis, a history of ASA intolerance, and chronic sinusitis were significantly higher in AERD patients than in those with ATA. The logarithm of PC20 values for methacholine challenge was significantly lower in the AERD group than that in the ATA group. Although the FEV1 was significantly lower in AERD patients than in ATA patients, the difference became non-significant after logistic regression analysis. The factor showing the highest association was a history of aspirin intolerance (odds ratio [OR]=23.9), followed by chronic sinusitis (OR=4.28), PC20 methacholine (OR=0.4), and nasal polyps (OR=2.4).
Diagnostic value of clinical parameters for the prediction of AERD in asthmatic patients
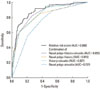
We tested the sensitivity and specificity for AERD using ROC curves (Fig. 1). The area under the curve (AUC) of the four variables ranged from 0.672 to 0.768. The history of aspirin intolerance showed the highest AUC value (0.768). A history of aspirin hypersensitivity was observed in 50 of 628 subjects with ATA (8%) and in 66 of 102 subjects with AERD (64.7%). Thus, 15.9% of all subjects studied had a positive history of aspirin hypersensitivity. In subjects having a history of aspirin hypersensitivity (n=116), AERD was proven in 66 subjects (56.9%) by the oral provocation test. The other 43.1% of subjects with histories of aspirin hypersensitivity had negative OAC test results.
The sensitivity and specificity of a history of aspirin hypersensitivity for predicting AERD were 64.7% and 92.0%, respectively (Table 3). The positive and negative predictive values were 56.9% and 94.1%, respectively. The overall accuracy of the test was 88.2%. When nasal polyps were present, the sensitivity and specificity to predict AERD were 61.4% and 68.5%, respectively. The positive and negative predictive values when polyps were present were 28.1% and 89.8%, respectively. The overall accuracy of the test was 67.3%. The presence of chronic sinusitis predicted AERD with sensitivity and specificity of 72.6% and 58.0%, respectively. The positive and negative predictive values were 25.6% and 91.4%, respectively. The overall accuracy of the test was 60.4%.
Diagnostic values of the clinical parameters to predict AERD according to the presence or absence of history of aspirin hypersensitivity
To identify additional parameters affecting the development of AERD, we compared clinical parameters between four groups: ATA groups and AERD groups with or without a history of aspirin hypersensitivity. As shown in Table 4, ATA subjects with a history of aspirin hypersensitivity had a higher female proportion, PC20 value, and FEV1% than those in the AERD group. In contrast, AERD subjects without a history of aspirin hypersensitivity showed lower FEV1% and PC20 values than did those in the other groups.
Additionally, we analyzed the clinical parameters related to AERD in asthmatic patients with or without a history of aspirin hypersensitivity using backward logistic regression analysis (Table 5). Among patients without a history of aspirin hypersensitivity, the ratio of individuals with chronic sinusitis was significantly higher in AERD patients than in ATA subjects (OR=4.95, P=0.0056). Furthermore, the logarithm of PC20 values for methacholine challenge was significantly lower in the AERD group than in the ATA group (OR=0.39, P=0.0016). In contrast, the ratio of patients with nasal polyposis was significantly higher in AERD patients than in ATA patients without a history of aspirin hypersensitivity (OR=11.54, P=0.0019).
In the asthmatic patients without a history of aspirin hypersensitivity, the sensitivity and specificity of the presence of chronic sinusitis to predict AERD were 81.3% and 58.4%, respectively (Table 6). The positive and negative predictive values were 11.5% and 97.9%, respectively. The overall accuracy of the test was 59.8%. When patients had a history of aspirin hypersensitivity, the sensitivity and specificity of the presence of nasal polyposis to predict AERD were 68.0% and 64.9%, respectively. The positive and negative predictive values were 72.3% and 60.0%, respectively. The overall accuracy of the test was 66.7% (Table 6).
Function for calculating relative risk score to predict AERD in asthmatic patients
Using the beta value of each parameter, we calculated the relative risk score for individual subjects as follows: Σ (beta for variables×dummy values of clinical parameter)=0.874×nasal polyp+3.174×history of aspirin hypersensitivity+1.453×sinusitis+(-0.918)×log [PC20 methacholine]. The mean and standard deviation of this score were 3.70±1.74 and 0.69±1.46 in the AERD and ATA groups, respectively (t=12.91, df=71.84 and P=2.08×10-20, Fig. 2). The ROC curve for the risk score showed an AUC of 0.9, which was the highest value among all combinations of parameters (Fig. 3).
Considering the difference and standard deviations, we defined a cut-off value for AERD prediction at 2.06. Then, we compared the ratio of AERD and ATA individuals showing risk scores above the cut-off value. As shown in Table 7, the ratio of subjects showing a positive score was significantly higher in the AERD than that in the ATA group (OR: 16.62, P=2.19×10-24). The sensitivity and specificity of the risk scores for AERD prediction were 0.787 and 0.818, respectively. The positive and negative predictive values were 0.369 and 0.966, respectively. The overall accuracy of the test was 0.814.
DISCUSSION
In the present study, we evaluated clinical parameters as diagnostic tools to predict AERD. When clinical parameters were compared between the subjects with AERD and those with ATA, significant differences were found for eight parameters including age, BMI, FEV1%, PC20, urticaria, nasal polyps, chronic sinusitis, and history of aspirin hypersensitivity. A decline in FEV1 after aspirin provocation was not used as a covariate because it is a determinant for AERD. To exclude the interactions among the factors, a logistic regression analysis using the conditional backward method was applied. Among the eight clinical parameters, the presence of nasal polyps, a history of aspirin hypersensitivity, chronic sinusitis, and log [PC20 methacholine] remained significantly associated with AERD. Among these parameters, the most highly associated parameter was a history of aspirin hypersensitivity, followed by chronic sinusitis (OR=4.28), PC20 methacholine (OR=0.4), and nasal polyps (OR=2.4).
A history of aspirin hypersensitivity, chronic sinusitis, and nasal polyps has been described as the most important pattern of clinical parameters since the initial definition of the aspirin triad10 and AERD1. However, the presence of a positive clinical history varies widely across populations.6 Based on patients' histories alone, the incidence of aspirin sensitivity in Caucasian adults with asthma is 3-5%, but this percentage doubles or triples when adult asthmatic patients are prospectively challenged with aspirin.15-19 In an unselected Caucasian asthma population assessed by a meta-analysis, aspirin- and NSAID-induced hypersensitivity was shown to be 2.7% by verbal history only, in contrast to the 21.1% shown by the oral provocation test. In a preselected population with a history of aspirin-induced asthma, the incidence of aspirin- and NSAID-induced hypersensitivity was shown to be 12.2% by verbal history only, in contrast to the 29.5% identified by oral provocation test.20 In the present study, 15.9% of the total population studied had a positive history of aspirin hypersensitivity. In subjects having an aspirin hypersensitivity history (n=116), AERD was shown in 66 subjects (56.9%) by the OAC. These data indicated that the frequency of a history of aspirin hypersensitivity was markedly higher in Korean asthmatic patients in the present study compared with Caucasians. One possible explanation for this observation is that the study subjects were all patients with asthma. Several reports suggest that the prevalence of aspirin hypersensitivity increases significantly in populations with nasal polyposis, sinusitis, atopy, or asthma.15,19 Even in asthmatic patients, the prevalence of AERD is known to vary according to severity and subtype.21 Additionally, because the development and pathophysiology of AERD are considered to be dependent on genetic factors, the proportion of subjects with a history of AERD in a study population could be affected by genetic and racial differences.
Interestingly, 43.1% of the subjects with an aspirin hypersensitivity history had a negative OAC test result. This relationship indicates a very high ratio of false positivity associated with a history of aspirin hypersensitivity. This finding prompted us to estimate the diagnostic values of these clinical parameters. We applied ROC curves to test the sensitivity and specificity for aspirin hypersensitivity in asthmatic patients. Although the AUC of the four variables was statistically significant, the history of aspirin intolerance had the highest AUC value. Because the value of PC20 methacholine is continuous, this parameter was not analyzed for diagnostic sensitivity and specificity.
A history of aspirin hypersensitivity has low diagnostic sensitivity for aspirin hypersensitivity but the highest value for diagnostic specificity. Thus, the accuracy ratio was 88.2%. Interestingly, the positive predictive ratio was 56.9%. This result indicates that more than 40% of subjects with a history of aspirin hypersensitivity do not respond to aspirin challenge. The negative predictive ratio was 94.1%. This finding indicates that more than 6% of subjects having no history of aspirin hypersensitivity positively respond to aspirin challenge. A European survey showed that 15% of provocation-test-proven AERD patients were entirely unaware that they had aspirin intolerance.6 Thus, the 6% negative predictive ratio from our results was lower than that found in European populations.
The presence of nasal polyps and chronic sinusitis showed lower positive and negative predictive values compared with a history of aspirin hypersensitivity. Thus, among the parameters we studied, a history of aspirin hypersensitivity showed the best accuracy ratio. However, there was still a 40% false-positive and a 6% false-negative rate when predictions were based on the presence of a history of aspirin hypersensitivity.
Although the FEV1 was significantly lower in AERD patients compared with ATA patients in the present study, the difference was not significant after logistic regression analysis. The hyperreactive airway and low FEV1 associated with AERD may reflect the severity of asthma in subjects with AERD.2 A history of urticaria was more frequently observed in AERD. However, after multiple regression analysis, the significant association with AERD disappeared. This result may reflect the effects of more strongly associated parameters including a history of aspirin intolerance, chronic sinusitis, nasal polyps, and PC20 methacholine.
Comparisons between groups according to AERD status and AERD history (Table 4) showed that ATA subjects with a history of aspirin hypersensitivity had higher FEV1% values than did those in the AERD groups, which suggests that a subject with a lower FEV1% is more likely to have a positive response to the OAC test. In contrast, AERD subjects without a history showed lower PC20 and FEV1% values than those of the other groups, which suggests that a subject having airway hyperreactivity or reduced pulmonary function could be more susceptible to weak bronchospasms induced by the OAC test and therefore show a positive OAC result. Thus, these observations suggest that bronchoconstriction induced by the OAC test may be partially dependent on basal FEV1% and PC20 values. We also found that chronic sinusitis could be an additional predictor of AERD in subjects without a history of aspirin intolerance, and on other hand, nasal polyposis could be an additional predictor in subjects with an history of aspirin hypersensitivity (Tables 5 and 6). These results suggest that the absence of a history of a aspirin hypersensitivity and chronic sinusitis could be useful in predicting negative results on an OAC test and that a history of aspirin hypersensitivity and the presence of nasal polyposis could be helpful in identifying OAC-positive subjects.
To establish an integrating function to predict the results of OAC, we defined the relative risk score for AERD using the beta values obtained by logistic regression analysis for nasal polyposis, history of aspirin hypersensitivity, chronic sinusitis, and PC20 methacholine values (Figs. 2 and 3). The calculated risk score was very significantly higher in AERD patients compared with that in ATA patients, and the AUC of the score was 0.9 for each parameter. Furthermore, the sensitivity, specificity, and accuracy of the risk score for AERD prediction were 0.787, 0.818, and 0.814, respectively. These results suggest that a combination of parameters could be useful for predicting results of the OAC test. However, false-positive and -negative values were relatively high, at 0.16 and 0.025, respectively. Although this observation means that a combination of parameters is hard to apply to the prediction of AERD in clinical practice, the analysis of these parameters can provide basic information for developing non-invasive methods to diagnose AERD.
Several studies have aimed to develop non-invasive methods for easier diagnosis of AERD. In peripheral blood, flow-cytometric determination of basophil activation has been proposed for in vitro diagnosis of NSAID hypersensitivity syndrome.22 Galectin -10 mRNA23 and plasma eotaxin 224 have been shown to be elevated in subjects with AERD compared with those with ATA. Several proteomic candidates have been found to be associated with an increased risk of AERD.25 Urine leukotriene E4 and 9alpha 11beta in exhaled breath condensate showed a high sensitivity and specificity for discriminating between the two groups.26 Many genetic variants in the arachidonate pathway27-30 and immune and inflammatory pathways14,31,32 seem to be involved in the development of AERD. However, future studies must determine whether these biomarkers are superior to clinical parameters such as history of aspirin hypersensitivity.
In summary, we evaluated the diagnostic value of clinical parameters including the well known manifestation of aspirin hypersensitivity history, nasal polyposis, and chronic sinusitis to predict AERD in asthmatic patients. Among these parameters, a history of aspirin hypersensitivity has the best positive and negative predictive values for forecasting the outcome of the positive aspirin challenge test, demonstrating an overall accuracy of 88.2%. However, false-positive and -negative rates were still high. Thus, additional non-invasive methods are needed to reduce the errors in the use of these parameters as diagnostic tools.









 XML Download
XML Download