

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is defined as a reversible airway obstructive disease with increased airway hyperresponsiveness (AHR) and chronic airway inflammation.1 However, irreversible airflow obstruction, which is largely caused by airway remodeling, can occur in some asthmatics. Histological changes that define airway remodeling include smooth muscle hyperplasia and hypertrophy, vascular proliferation, increased number of bronchial glands, and collagen deposition.2-5 The avoidance of irreversible structural changes is critical in managing asthma, because the changes can cause partially irreversible airway obstruction and sustained AHR even after prolonged steroid therapy.2 Importantly, airway remodeling can begin in early childhood and with mild intermittent asthma.4,6
The most direct way of assessing airway remodeling is by histological examination of lung biopsy specimens. Alternatively, pulmonary function testing (PFT), which is has been used in clinical settings and epidemiological studies, can link changes in mechanical properties of airways with airway remodeling. Measurement of airway wall thickening on computed tomography (CT) is a noninvasive method for assessing structural airway changes. In several trials, high-resolution CT (HRCT) to assess airway remodeling in asthma has provided information about a broad range of lung morphological features,7-15 in a less invasive manner than biopsy.16 However, with CT, a possibility of errors exists because measurements of airway dimensions are based on manual tracing. To minimize errors, the full-width/half-maximum (FWHM) principle has recently been introduced for the quantitative assessment of airway wall dimensions.17
Although PFT can be used to evaluate the degree of airflow obstruction, the results can be affected by concomitant diseases or the short-term condition of the patient. For PFT to be applicable as a noninvasive method of assessing airway remodeling, the findings must correlate with those of HRCT. A low post-bronchodilator FEV1/FVC ratio has recently been proposed as a noninvasive marker of airway remodeling4 and as evidence of the need for preventative inhaled corticosteroid therapy in mild intermittent asthma.6 In terms of mechanical properties, airway wall thickening and collagen deposition can stiffen the subepithelial matrix and make the airways less responsive to bronchodilators.18-20 This alteration can also present as decreased distensibility during inspiration or as collapsibility during expiration. Airway collapsibility (AC) during expiration can be assessed by measuring the change in luminal area between inspiration and expiration CT.
The purpose of our study was to investigate the usefulness of automatic measurements of airway dimensions on CT for the assessment of airway remodeling, by analyzing the relationships between airway wall indices and PFT parameters. To our knowledge, this is the first study to analyze the correlations between airway wall indices on CT and post-bronchodilator FEV1/FVC, which is a known surrogate marker of airway remodeling, and to directly assess AC using automatic airway wall measurements on inspiration and expiration CT.
MATERIALS AND METHODS
Subjects
Forty-one patients experiencing dyspnea, cough, and wheezing for longer than 3 months were recruited from the allergy clinic at Asan Medical Center. The patients were diagnosed with asthma according to the American Thoracic Society criteria.1 Study inclusion criteria included a baseline FEV1/FVC of ≤80% and either demonstrated significant AHR (PC20 methacholine, <8 mg/mL) or significant bronchodilator responsiveness (>12% improvement in %FEV1 predicted after administration of 180 µg of albuterol via a metered-dose inhaler) before asthma treatment.21 One patient was excluded because the CT scan was obtained using a different protocol, and 18 patients were excluded because they had smoked more than five packs of cigarettes throughout their lifetime. Thus, 22 patients (3 men and 19 women; mean age, 50.2 years; age range, 25-70 years) were enrolled. All participants were non-smokers or ex-smokers who had smoked less than five packs throughout their lifetime. Each had received inhaled corticosteroid therapy (mainly 250-500 µg fluticasone) for several months to years, with or without other asthma medication, to maintain optimal physical condition. All patients gave informed consent to undergo PFT and CT, and the study protocol was approved by the institutional review board of our hospital.
CT
CT was performed in patients in a stably managed state and without evidence of asthma exacerbation. In all patients, volumetric CT scans were performed at both full inspiration and expiration, using a 16-channel, multidetector CT scanner (Somatom Sensation 16; Siemens Medical Solutions, Erlangen, Germany) with 16×0.75-mm collimation, 100 eff. mA, and 140 kVp. The CT dose index (approximately 22.5 mGy) was within the acceptable in range. The acquired data were reconstructed using a standard kernel (B30) with 0.75 thickness and 0.7-mm increments. Images were stored in the Digital Imaging and Communications in Medicine (DICOM) format, which is the international standard for connecting medical imaging devices on standard networks.
In-house software was used for airway measurements. Figure shows the overall procedure and snapshots of each stage of the procedure. After loading the DICOM images, the user is requested to select a point in the airway lumen. The software then estimates the central axis of the airway lumen using a depth map algorithm and reconstructs an oblique image orthogonal to the axis. The software magnifies the oblique image 10-fold using a bi-cubic interpolation algorithm, segments the lumen according to a Hounsfield unit-based thresholding technique, and then calculates the center of inertia of the lumen. The airway wall indices are determined by analysis of 120 rays cast around 360° from the center, according to the FWHM method.17 The software was validated using polyacryl tubes with various inner diameters and wall thicknesses.22,23
Airway dimensions were measured at the origin of four segmental bronchi: right apical bronchus, left apico-posterior bronchus, and the posterior basal segmental bronchus in each lower lobe. Measurements were made at the same anatomic locations on both inspiration and expiration CT scans. Mean values were used for each subject. To analyze luminal changes, the bronchial-to-arterial diameter (BA) ratio was measured on CT images obtained on inspiration, and the luminal area (LA) was measured on inspiration and expiration CT images. The measured luminal areas were used to calculate AC as [(LAinsp - LAexp)/LAinsp]×100. The airway wall indices included wall thickness (WT), wall thickness percentage [WT%=(WT/outer diameter)×100], and wall area percentage [WA%=(WA/WA+LA)×100].
Given that an increase in end-expiratory lung volume (EELV) caused by air trapping can influence AC, we analyzed the relationship between AC and EELV. The ratio between mean whole-lung density (MLD) on expiration and inspiration (MLDexp/MLDinsp) was used as the air trapping index (ATI).
Clinical parameters
The clinical indices included body mass index (BMI), asthma severity, and spirometry data before and after use of bronchodilators. The severity of asthma was evaluated by physicians at the time of CT scanning and was classified as mild, moderate, or severe based primarily on the Global Initiative for Asthma guidelines.24 All subjects were prohibited from using any kind of bronchodilators for a minimum of 6 hours before CT scanning, and the time between inhaled corticosteroid use and CT scanning did not differ among the subjects. Pre- and post-bronchodilator tests were performed on the same day as CT scanning, or on the day before or after. To evaluate the presence of atopy, skin prick testing for 11 common aeroallergens (Allergopharma, Reinbek, Germany) was performed as previously described.25 Atopy was defined as a positive skin prick test response (allergen/histamine ratio >1.0 plus mean wheal size >3 mm) to one or more allergens. Testing was performed at the time asthma was diagnosed, irrespective of CT scanning.
Statistical analysis
The SPSS statistical package (version 12.0; Chicago, IL, USA) was used for statistical analysis. The relationships between airway wall indices measured on CT and clinical indices were evaluated using Spearman's correlation test. Values of P<0.05 were considered to indicate statistical significance.
RESULTS
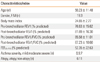
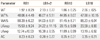
The demographic characteristics and clinical indices of our study subjects are presented in Table 1, and the airway dimensions measured in four segmental bronchi are shown in Table 2. There was no significant difference between airway dimensions in four segmental bronchi.
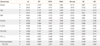
Table 3 lists the correlations between the CT measurements and clinical indices. WT% showed negative correlations with %FEV1, FEV1/FVC, FEF25-75%, and post-bronchodilator FEV1/FVC (r=-0.434, P=0.043; r=-0.431, P=0.019; r=-0.540, P=0.009; and r=-0.503, P=0.017, respectively) and a positive correlation with asthma severity (r=0.470, P=0.027). WT was negatively correlated with FEV1/FVC, FEF25-75%, and post-bronchodilator FEV1/FVC (r=-0.431, P=0.045; r=-0.581, P=0.005; and r=-0.576, P=0.005, respectively), and WA% was negatively correlated with FEF25-75% (r=-0.459, P=0.032) and BMI (r=0.453, P=0.034). The BA ratio showed positive correlations with %FEV1, FEF25-75%, and post-bronchodilator FEV1/FVC (r=0.459, P=0.032; r=0.479, P=0.024; and r=0.454, P=0.034, respectively). AC showed a strong positive correlation with FEV1/FVC (r=0.592, P=0.004) and post-bronchodilator FEV1/FVC (r=0.475, P=0.025). ATI was negatively correlated with FEV1/FVC, FEF25-75%, and post-bronchodilator FEV1/FVC (r=-0.534, P=0.011; r=-0.591, P=0.004; and r=-0.610, P=0.003, respectively). AC showed no significant correlation with EELV (r=-0.416, P=0.054).
DISCUSSION
We demonstrated that the WT%, WT, BA ratio, AC, and ATI were correlated with post-bronchodilator FEV1/FVC, which is a surrogate marker of airway remodeling. In practice, it is important to noninvasively assess airway remodeling during treatment and follow-up of patients with asthma. Our study is believed to be the first to reveal that in addition to post-bronchodilator FEV1/FVC, airway wall indices on CT can be used as surrogate markers of airway remodeling.
Although biopsy is the most accurate method of determining airway remodeling, it is an invasive procedure. In children and young adults, the ratio of FEV1 to FVC is a useful index of the status of the airway.26,27 Rasmussen et al.4 have shown that airway remodeling is demonstrated by a low post-bronchodilator FEV1/FVC, and several studies have used low post-bronchodilator FEV1/FVC as a marker of persistent airflow limitation or airway remodeling.6,28 Although those studies measured post-bronchodilator FEV1/FVC in a consecutive manner, it is thought that a one-time check of post-bronchodilator FEV1/FVC reflects the real-time state of persistent airflow limitation in patients who have received optimal treatment to reach a stable condition. Considering the association between airway structural alterations and severe asthma,5 post-bronchodilator FEV1/FVC may be an important marker of airway remodeling. In addition, pre-bronchodilator FEV1/FVC has been used as an indicator of global airway obstruction in asthma in several HRCT studies.16,29 Our data showed significant correlations of asthma severity with both pre- and post-bronchodilator FEV1/FVC.
In previous studies, the airway wall was thicker in patients with asthma, and greater wall thickening was associated with more severe asthma.7-15,30 These studies measured the apical bronchus of the right upper lobe because of its tangential orientation. We used the mean values of the airway dimensions of four segmental bronchi, presuming that these would be closer to the actual airway dimensions. Kasahara et al.11 compared the airway dimensions, the reticular basement membrane (Rbm) on biopsy, and FEV1 between asthmatics and control subjects, showing that WA% and WT% were strongly correlated with Rbm thickness. These findings suggest that Rbm thickening parallels the airway wall thickening, which can cause irreversible airflow obstruction in asthma.
We investigated the luminal change between inspiration and expiration CT and defined it as AC. Brown et al.31 used HRCT to test the hypothesis that when the lungs of asthmatics become inflated by deep inspiration, the airways do not distend; however, they found no defect in airway distensibility in patients with asthma, perhaps because they selected stable patients with mild intermittent asthma who used only sympathomimetic inhalers on an as-needed basis. In our study of patients with asthma of various severities, AC had a strong positive correlation with pre- and post-bronchodilator FEV1/FVC, indicating that more severe obstruction showed a lower AC. One possible explanation of this finding is that in at least some patients, the process that thickens the airways also makes them stiffer and less collapsible during expiration. Wilson et al.20 have reported that patients with asthma exhibit less distensible airways during inspiration, based on the change in anatomic dead space. Other researchers have attributed this phenomenon to Rbm thickening by showing an inverse correlation between anatomic dead space and Rbm thickness.19 Using an esophageal balloon and a Pitot static probe to obtain area-versus-transmural pressure curves during forced expiration, Brackel et al.18 also indicated that asthmatic airways may be less collapsible or distensible and concluded that airway remodeling may result in stiffer dynamic elastic properties of the airway walls. Fibrotic changes induced by airway remodeling may cause airways with persistent airflow obstruction to become less collapsible. Alternatively, an increase in residual lung volume due to air trapping in patients with obstructive lung disease may decrease airway collapse during expiration. In the present study, because AC did not correlate with EELV, the decrease in AC is thought to reflect the intrinsic stiffness of the airway resulting from wall thickening.
In our study, ATI showed negative correlations with FEV1/FVC, FEF25-75%, and post-bronchodilator FEV1/FVC. These results are similar to previous observations. Gono et al.9 have reported that the expiration/inspiration ratio of MLD is negatively correlated with FEV1, and Mitsunobu et al.32 have demonstrated that MLD is lower in unstable asthmatics than in stable asthmatics. However, our results more accurately reflect the actual CT value because we obtained volumetric data, whereas others obtained data from selected levels. Carroll et al.33 have reported that small airways are the predominant obstruction sites in postmortem studies.34 Although changes in small airways cannot be directly visualized on CT, air trapping is indirectly reflected by abnormal decreases in lung attenuation.34 In our study, ATI obtained by CT has been proven to be a useful parameter for assessing the presence of small airway obstruction.
The BA ratio showed positive correlations with FEV1, FEF25-75% and post-bronchodilator FEV1/FVC. The pulmonary artery diameter is largely influenced by circulating volume and local hypoxia.35 In general, the BA ratio increases with altitude, presumably due to to hypoxic bronchodilatation and vasoconstriction.36 However, a reduced BA ratio is more common in patients with asthma than in control subjects.14 This is an interesting observation considering that asthma patients exhibit a higher expression level of vascular endothelial growth factor compared with controls. Given that increased vascular endothelial growth factor is correlated with increased vascularity and angiogenesis,37 it may contribute to airway wall remodeling.
The BMI showed a positive correlation with WA%. This is consistent with a previously reported association between obesity and asthma.38
This study is believed to be the first to use the FWHM principle for measuring airway dimensions in asthma. Since McNamara et al.39 first measured airway dimensions using HRCT in canine lung, investigators have sought to demonstrate the relationship between airway wall thickness and function.7-15,30 In earlier studies, airway dimensions were measured by semi-quantitative assessment using manual tracing,15 which created problems when measuring small bronchi because the boundaries between the lumen, wall, and parenchyma became difficult to define. Forkert et al. overcame this problem by using the density plot of a straight line perpendicular to the airway wall.40 Nakano et al.17 used the FWHM principle to measure airway dimensions in the lungs of smokers, and the FWHM technique has been demonstrated to be a reproducible method of airway measurement.41
One limitation of our study is the uncertainty regarding how closely CT measurements reflect in vivo airway dimensions; for example, secretions might have caused an overestimation of WT. Another limitation is that the CT scans were performed when the patients were taking inhaled corticosteroids. Our subjects had taken inhaled corticosteroids for at least the previous 3 months, to maintain optimal physical condition; therefore, corticosteroids might have caused an underestimation of airway dimensions in patients with severe asthma. Nevertheless, we believe that the relative influence of medication in our subjects was minimal, because all subjects used corticosteroids at similar doses. Moreover, there are minimal data indicating that corticosteroid use influences airway remodeling,42-45 and there is a theoretical advantage to evaluating the status of airway remodeling in stably maintained asthma. The use of post-bronchodilator FEV1/FVC as a marker of airway remodeling in our study may be criticized, because it has been not yet been confirmed to represent airway remodeling. In addition, this was a small study of 22 subjects, 86% of whom were female, which was not unexpected given that we excluded heavy smokers. The results of this study will need to be reproduced in different and larger patient populations. As another limitation, we were unable to apply multivariate regression analysis because of the small number of study subjects. However, we believe that the level of FEV1 reflected the impact of age and gender. In patients with stable asthma, radiation exposure may limit the clinical application of CT, and CT protocols with reduced radiation doses need to be developed further. Finally, AC might have been underestimated, because we measured the airway dimensions on suspended end-expiration and not dynamic expiration. On suspended end-expiration, the airway may collapse less because the intrathoracic pressure is not maximal during dynamic expiration.46 However, owing to motion artifacts and higher radiation dose, it is difficult to elicit the difference in airway dimensions in the segmental bronchi during dynamic expiration.
In the present study, we demonstrated that post-bronchodilator FEV1/FVC was significantly correlated with CT parameters, including WT%, WT, BA ratio, AC, and ATI. Our results support the theory that airway wall thickening associated with remodeling causes a decrease in airway luminal collapsibility during expiration in asthma. In conclusion, airway wall indices measured on inspiration and expiration CT, together with post-bronchodilator FEV1/FVC, are useful indicators of the state of airway remodeling in stably managed patients with asthma.

 XML Download
XML Download