

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is an airway disorder characterized by inflammation, variable airflow obstruction, and airway hyperresponsiveness (AHR). The infiltration of eosinophils, mast cells, and CD4 lymphocytes, in addition to airway remodeling (including subepithelial fibrosis and hyperplasia of goblet cells and smooth muscle fibers), are all characteristic of asthma.1 Excessive production of interleukin (IL)-4, -5, and -13 by T helper type 2 (Th2) cells has been implicated in the pathogenesis of allergic asthma. IL-5 mobilizes eosinophils from the bone marrow pool while chemokines such as eotaxin-1 induce the recruitment of eosinophils to the airway.2 Eosinophils are multifunctional leukocytes that release a plethora of immunomodulatory compounds, including potent inducers of the inflammatory and immune responses observed in asthma, eczema, rhinitis, and other autoimmune diseases.3 Airway eosinophils, which release mediators that damage the airway epithelium, have been thoughted as a major contributor to AHR in asthmatic patients4; however, this paradigm has been challenged by data obtained from studies in humans. In one such study, the administration of an anti-IL-5 antibody decreased peripheral blood and sputum eosinophilia in asthmatic patients but did not affect airway hyperreactivity.5 Subsequent analysis of bronchial biopsies confirmed these findings and highlighted the role of eosinophils in airway tissue remodeling.6 Thus, while much has indeed been learned about the role of eosinophils in asthma, many unanswered questions remain. In this manuscript, I shall first describe the results of studies performed in my laboratory and discuss the biological and morphological differences between asthma and eosinophilic bronchitis (EB). EB is an interesting clinical manifestation of eosinophilic airway disease that does not involve AHR, demonstrating that airway eosinophilia alone is insufficient to merit a diagnosis of asthma. Second, I will describe and discuss the effect(s) of single-nucleotide polymorphisms (SNPs) in the genes CCR3, IL-5 RECEPTOR ALPHA (IL5RA), and IL1RL1, and the in vitro and in vivo effects of Notch inhibition on both eosinophil differentiation and experimental asthma.
LESSONS FROM A CLINICAL PHENOTYPE OF EOSINOPHILIC BRONCHITIS
There exists a poorly defined group of patients with similar levels of eosinophilic airway inflammation but normal airflow and no evidence of BHR.7 EB is a common cause of chronic cough syndrome.8,9 Morphologic and cellular changes, including alterations in basement membrane thickness and in the numbers of eosinophils, mast cells, and T-lymphocytes in the submucosa, are comparable in EB and asthma. In addition, no differences in the expression of eosinophil-active cytokines, chemokines, T-cell activation markers, or exhaled nitric oxide have been found among individuals with these conditions.10,11 However, in our study using thin-section CT scanning, those patients with EB showed no thickening of the large airway walls, whereas the amount of trapped air and centrilobular prominence were similar in patients with EB and asthma (Fig. 1).12 These results suggest that eosinophilic inflammation is not always accompanied by large airway wall thickening, which may explain the normal responsiveness to methacholine in the airways of EB patients. The absence of BHR in EB is also attributed to the normal number of mast cells in airway smooth muscle as compared to asthma.13 The infiltration of airway smooth muscle by IL-4- and IL-13-expressing mast cells is characteristic of asthma but not EB.14 This was confirmed by assays of the IL-13 level in sputum samples. IL-13 was present at higher concentrations in the sputum of asthmatics as compared to those with EB; IL-5 levels were similar between the two groups (Fig. 2). In addition, sputum IL-13 levels were inversely correlated with the PC20 concentration in subjects with asthma.15 These findings raise the possibility that interactions between mast cells and airway smooth muscle in addition to the overproduction of cytokines contribute to bronchial wall thickening and the development of AHR, but that eosinophils do not. However, in a long-term prospective follow-up study,16 EB recurred in one-fifth of patients who stopped using inhaled steroids. A progressive reduction in FEV1 was observed in individuals with recurrent EB, but not in those whose EB was non-recurrent (Fig. 3). This suggests that recurrent EB is accompanied by deterioration of the airflow rate. Based on these findings, it is possible that some subjects with recurrent EB also have a component of asthma or chronic asthmatic bronchitis; thus, further research is needed.
ASSOCIATION OF GENETIC VARIANTS WITH BLOOD EOSINOPHILIA
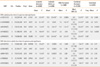
Prior to the publication of a genome-wide association study, research on candidate genes provided information on the contribution of eosinophilia-associated genetic alterations to asthma. Eosinophilic infiltration and peripheral blood eosinophilia are dependent on the cooperative action of eosinophil-specific cytokines and chemokines (e.g., IL-5 and members of the eotaxin family). CCR3, an eotaxin receptor, plays an important role in the infiltration of eosinophils into target tissues in cooperation with IL-5.2 The human CCR3 gene (MIM number 601268), located on chromosome 3p21.3, has been linked to atopic dermatitis and asthma.17 IL-5 is important for the terminal differentiation, activation, and survival of committed eosinophil precursors, via an effect mediated by IL-5 receptor (IL-5R).18 The human IL-5R complex is a heterodimer composed of alpha and beta subunits.19 The IL5RA gene (MIM number 147850), located on chromosome 3p26-p25, has also been linked to the development of asthma.20 In a genome-wide scan using polymorphic markers, the linkage of chromosome 5q with familial eosinophilia was shown.21 This region contains a cytokine gene cluster that includes three genes, the products of which play important roles in the development and proliferation of eosinophils: IL3, IL5, and CSF2. However, no other studies have demonstrated sporadic eosinophilia-associated genetic variants in this region. We previously reported the association of variations in candidate genes with eosinophilia in asthma. Three completely linked SNPs (222557G>A, 2520T>G, and 2174C>T) in CCR3 as well as the c.25091G>A polymorphism and c.2480_482ins/del in IL5RA were associated with eosinophil abundance in the peripheral blood of asthmatics.22 There is an intergenetic association between CCR3 ht2 and c.25091G>A of IL5RA, such that the genetic effect of this combination lowers P values more than the effect of either condition alone (Table 1).
Data from a genome-wide SNP study of 9,392 Icelanders with known blood eosinophil counts suggested that an SNP (rs-1420101) in IL1RL1 was associated with asthma; a similar phenomenon was observed in a collection of ten different populations (7,996 cases, including 1,958 Koreans and 44,890 controls; Table 2).23 SNPs within the genes encoding WDR36, IL-33, and MYB that showed a suggestive association with eosinophil counts were also associated with atopic asthma in these populations. Rs1420101 on 2q12 is located in IL1RL1, while rs3939286 on 9p24 is located 32 kb proximal to the start codon of IL-33. IL-33 encodes a cytokine belonging to the IL1 superfamily, and is the natural ligand for the IL1RL1 receptor. IL-33 also functions as a chromatin-associated nuclear factor with transcriptional regulatory properties.24 Signaling through the IL1RL1-IL-33 complex has an important role in eosinophil maturation, survival, and activation, both by direct effects on eosinophils and indirectly through the recruitment and regulation of Th2 cell effector functions. These findings are consistent with the proposed function of IL1RL1-IL-33 signaling in eosinophil-mediated inflammation.25 After functional analysis reveals how these genetic variances affect the differentiation of eosinophils and development of asthma, they may be used as targets for novel diagnostic assays and therapies.
REGULATION OF EOSINOPHIL DIFFERENTIATION AND NOTCH SIGNALING
During eosinophil development, the early action of IL-3 and GM-CSF results in the proliferation and differentiation of stem cells into multipotent myeloid and eosinophil progenitor cells, while IL-5 supports the expansion, terminal differentiation, and functional activation of eosinophils. Notch is an evolutionarily conserved transmembrane protein involved in the regulation of a broad spectrum of cell fate decisions and differentiations.26 Notch signaling regulates the terminal differentiation and subsequent effector phenotypes of eosinophils, partly through modulation of the ERK pathway.27 Enzymatic cleavage of Notch by γ-secretase is essential for Notch-mediated signaling. Gamma-secretase inhibitor (GSI) has been used to effectively block Notch signaling; the pharmacological equivalent of a loss of Notch function. We previously demonstrated that GSI induces the differentiation of eosinophils lacking effector functions.28 Notch signaling is also required for the development of Th2-type immunity.29 It is, therefore, possible that the restriction of Th2 and eosinophil inflammatory responses by GSI will ameliorate the symptoms of asthma. GSI administration has been shown to inhibit many of the pathological and histological characteristics of asthma, including eosinophilic airway inflammation, goblet cell metaplasia, methacholine-induced AHR, and elevated serum IgE levels (Fig. 4A and B).30 An ex vivo study of the effect of GSI on stimulated BAL cells showed both the inhibition of Th2 cytokine production and the augmentation of Th1 cytokine production (Fig. 4C). This skewing of the cytokine production profile from Th2- to Th1-type responses provides an empirical basis for the use of GSI as an antiasthma agent. Notch has been shown to directly induce the transcription of GATA-3.31 Reduced GATA-3 levels in BAL cells due to GSI treatment cause decreased Th2 cytokine production via a Notch-dependent pathway, thereby inhibiting Th2-associated responses in the airway. GSI treatment also increases T-bet levels, which promote a Th1 response, as evidenced by enhanced IFN-γ expression. The marked effect of GSI on eosinophil differentiation and the balance of Th1- and Th2-type responses mediated by Notch-dependent signaling demonstrate the potential therapeutic value of this protein in the treatment of asthma.
In summary, the data presented herein suggest that eosinophilic airway inflammation is not as important in the pathogenesis and maintenance of asthma as had previously been thought. However, the role of eosinophils in other asthma subphenotypes, including refractory or severely remodeled asthma, needs to be evaluated further. High-throughput methodologies such as genomics and proteomics will facilitate the discovery of new markers of inflammation; these, in turn, will aid in the evaluation of the role of eosinophils in asthma and its various subphenotypes. Biomarkers detected as important in airway eosinophilia will help highlight processes involved in the pathogenesis of subphenotypes of asthma, including the possible participation of eosinophils.





 XML Download
XML Download