

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Peroxisome proliferator-activated receptors (PPARs) are transcriptional factors activated by ligands of the nuclear hormone receptor superfamily. This superfamily is divided into the steroid receptor family and the thyroid, vitamin D, and retinoid (or non-steroid) receptor family.1 Three different PPAR subtypes have been identified: PPARα (PPARA), PPARγ (PPARG), and PPARδ (PPARD, which is also called PPARβ). PPARG (MIM #601487), located on chromosome 3p25, plays an important role in regulating adipocyte differentiation and lipid metabolism2 as well as cell turnover.3 However, the production of immune-modulating cytokines in various cell types was reported to downregulate the expression of PPARG, and block adipocyte differentiation. It is well established that a variety of natural substances, including arachidonate pathway metabolites such as 15-hydroxyeicosatetranoic acid (15-HETE), strongly promote PPARG expression.3-5 Stimulation of the PPARG ligand significantly inhibited the downregulation of eosinophil function.6 PPARG expression is associated with the inflammatory and remodeling responses in the asthmatic airway.7
Among the sub-phenotypes of asthma, aspirin-intolerant asthma (AIA) refers to the development of bronchoconstriction in asthmatic individuals following the ingestion of aspirin or other non-steroidal anti-inflammatory drugs. This syndrome is characterized by the 'aspirin triad' of aspirin hypersensitivity, bronchial asthma, and nasal polyposis.8 Most clinical investigators now include chronic hyperplastic eosinophilic sinusitis (CHES) as a fourth hallmark of aspirin-exacerbated respiratory disease (AERD).9 As is true for other asthmatic individuals, the airways of patients with AIA show signs of persistent inflammation, with marked eosinophilia, epithelial disruption, cytokine production, and upregulation of inflammatory molecules.10 Although the pathogenesis of AIA has not been elucidated completely, multiple points of overproduction or underproduction of critical mediators in the metabolism of arachidonic acid, including leukotrienes, lipoxins, thromboxane, and prostaglandins, probably account for the susceptibility to aspirin.10 In addition, the levels of proinflammatory, immune cytokines and chemokines, including IL-2, IL-3, IL-4, IL-5, IL-13, GM-CSF, and eotaxin, are increased in the airways and systemic circulation in AIA.11,12 The production of these molecules is regulated by various transcription factors, including PPARG. Therefore, genetic variants of the PPARG gene may be associated with the development of asthma or aspirin intolerance in asthmatics.
Recently, Palmer et al. reported that PPARG gene polymorphisms are associated with a risk for asthma exacerbation in Caucasian populations.13 We also reported that the homozygous haplotype combination of +34C>G (Pro12Ala) was associated with an increased risk for asthma exacerbation.13 To our knowledge, however, no study has analyzed the potential associations of the two common polymorphisms of the PPARG gene [+34C>G (Pro12Ala) and +82466C>T (His449His)] with the risk for aspirin intolerance in asthmatics.
MATERIALS AND METHODS
Subjects
The subjects were recruited from the Asthma Genome Research Center, comprising Soonchunhyang Bucheon, Seoul, and Chunan Hospitals, and Chunnam and Chungbuk University Hospitals in Korea. All of the subjects were Korean. A clinical history was obtained for each patient, using a physician-administered questionnaire that included the history of aspirin hypersensitivity. The asthmatics had compatible clinical symptoms and physical characteristics (Global Initiative for Asthma).14 All patients had a history of dyspnea and wheezing during the previous 12 months plus one of the following: 1) >15% increase in FEV1 or >12% increase plus 200 mL following inhalation of a short-acting bronchodilator; 2) <10 mg/mL PC20 methacholine; or 3) >20% increase in FEV1 following 2 weeks of treatment with inhaled steroids and long-acting bronchodilators. The asthmatics had experienced no exacerbation of asthma or any respiratory tract infection in the 6 weeks preceding the oral aspirin challenge (OAC). Based on the results of the OAC, the asthmatics (n=403) were categorized into two groups: those with a decrease in FEV1 of 15% or greater (AIA, n=60), and those with a decrease of less than 15% [aspirin-tolerant asthma (ATA), n=343]. The oral provocation test was performed with increasing doses of aspirin (10-450 mg Astrix; Mayne Pharma, Melbourne, Australia) using a modification of a previously described method.15,16 Aspirin-intolerance bronchospasm, as reflected by the rate (%) of FEV1 decline, was calculated as the difference between the pre-challenge and post-challenge FEV1 values divided by the pre-challenge FEV1. Subjects who developed skin manifestations were labeled as positive responders (n=60). Normal controls (n=449) were recruited from among spouses of the patients or members of the general population who answered negatively to a screening questionnaire regarding respiratory symptoms.17 The normal controls had no history of aspirin intolerance and had FEV1 values >80% predicted, PC20 methacholine >10 mg/mL, and normal findings on simple chest radiograms. Skin prick tests were performed with 24 common aeroallergens (Bencard, Brentford, UK). Atopy was defined as one or more positive reactions (>3 mm in diameter) on the skin prick test. Total IgE was measured using a UniCAP system (Pharmacia Diagnostics, Uppsala, Sweden). Subjects with diabetes mellitus were excluded because the PPARG polymorphism is reported to be associated with the development of diabetes mellitus in Koreans.18 All subjects gave written informed consent to participate in the study, and the protocol was approved by the local ethics committees.
Genotyping the SNPs in the PPARG gene
The amplifying primers and probes used to genotype the polymorphic sites by the single base method were as described previously.19 Primer Express (Applied Biosystems, Foster City, CA, USA) was used to design the PCR primers and MGB TaqMan probes. One allelic probe was labeled with FAM dye; and the other, with fluorescent VIC dye. PCR was performed in TaqMan Universal Master Mix, without uracil-N-glycosylase (Applied Biosystems), containing 900 nM TaqMan MGB-probe and 200 nM primer. The reaction was performed in a 384-well plate in a total reaction volume of 5 µL, using 20 ng of genomic DNA. The plate was heated in a thermal cycler (PE 9700; Applied Biosystems) for 2 min at 50℃ and then for 10 min at 95℃, followed by 40 cycles of 95℃ for 15 s and 60℃ for 1 min. The fluorescence intensity of each reaction was determined using a Prism 7900 HT detector (Applied Biosystems), and the fluorescence data were analyzed by automated software (SDS 2.1).
Statistical analysis
We applied the widely used Lewontin's D' (|D'|) and R2 measures of linkage disequilibrium to all pairs of biallelic loci.20 Haplotype associations were estimated using HaploScore (http://www.biostat.wustl.edu/genetics/geneticssoft/), which computes score statistics to test for associations between a given haplotype and a wide variety of traits, including binary, ordinal, quantitative, and Poisson parameters. The genetic effects of the haplotypes were analyzed in the same way as the SNPs. The distributions of the PPARG SNP genotypes and haplotypes among the subjects with asthma and the normal subjects were analyzed with logistic regression models that controlled for age (continuous value), gender (male=0, female=1), atopy status (non-atopy=0, atopy=1), body mass index (BMI; continuous value), and smoking status (nonsmoker=0, ex-smoker=1, smoker=2) as covariates. The data were managed and analyzed using SPSS ver. 10.0 (SPSS, Chicago, IL, USA). A value of P≤0.05 was regarded as statistically significant.
RESULTS
Characteristics of the study subjects
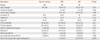
We recruited 403 subjects from the asthma cohort. The clinical characteristics of the study subjects are summarized in Table 1. The maximum fall in FEV1 during the 5-hr follow-up period after aspirin challenge was used as the value for the aspirin-induced fall in FEV1. Aspirin-induced declines in FEV1 ranged from -15% to 68%. The log transformed PC20 methacholine values for the asthmatics were significantly lower among those with AIA than among those with ATA (P=0.013, Table 1).
PPARG polymorphisms and the risk for aspirin intolerance in asthmatics
Two SNPs, +34C>G (P12A) on exon 3 and +82466C>T (H449H) on exon 8, in the PPARG gene were genotyped for the association study. The minor allele frequencies (MAFs) of these two SNPs in the Korean population were 0.042 (+34C>G) and 0.168 (+82466C>T) (Table 2). The genotype distributions of the two SNPs were in Hardy-Weinberg equilibrium for all subjects (P>0.05, Table 2). Four haplotypes were constructed, and two haplotypes with a frequency >0.05 were used for the analysis. Using multiple logistic regression models, both SNPs and the two haplotypes (ht1 and ht2) were analyzed for associations with the risk for aspirin intolerance in the asthmatics (Table 3). The analysis revealed that PPARG+82466C>T was associated with aspirin intolerance in the recessive model, and there were more subjects homozygous for the rare alleles PPARG+82466C>T in the AIA group than in the ATA group in the recessive model (6.66% vs. 2.04%, P=0.04, OR=3.97 [1.08-14.53]). In the haplotype analysis, there were fewer subjects with ht1 in the AIA group than in the ATA group (93.33% vs. 97.96%, P=0.04, OR=0.25 [0.07-0.92]) in the dominant model. The rate (%) of FEV1 decline after aspirin challenge is the most important parameter for the diagnosis of aspirin intolerant asthmatics, and thus we used linear regression analysis to investigate the associations between the SNP (+82466C>T), haplotype 1, and percentage fall of FEV1 following aspirin challenge. Haplotype 1 and +82466C>T showed the strongest association with the rate (%) of FEV1 decline after aspirin challenge in the asthmatics. Asthmatics homozygous for the rare +82466C>T allele had a greater decline in FEV1 after aspirin provocation than those with the common allele (P=0.0004, Fig. 1A). In the haplotype analysis, the decline in FEV1 after aspirin provocation was greater in asthmatics lacking the ht1 haplotype than in those with the haplotype (P=0.0004, Fig. 1B).
DISCUSSION
PPARs are receptors for steroids, thyroid hormone, vitamin D, and retinoic acid,1 and they regulate adipocyte differentiation, lipid metabolism,2 and cellular turnover.3 Furthermore, polymorphisms of the PPARG gene have been associated with diabetes, obesity, and metabolic syndrome.18,21-25 The two common polymorphisms of PPARG were reported to modify susceptibility to type II diabetes mellitus, obesity, and sub-phenotypes of metabolic syndrome in Koreans18,21,22 and Caucasians.23-26 Therefore, we excluded subjects with diabetes from the analysis and adjusted the results for the BMI.
In addition to their metabolic effects, PPARs/RXRs heterodimerize with various receptors, and these heterodimers regulate the transcription of genes involved in allergic inflammation and airway remodeling.7 A notable finding in our study was that the SNP PPARG+82466C>T was associated with aspirin intolerance. There were more subjects homozygous for the rare PPARG+82466C>T allele with AIA than with ATA in the recessive model (Table 3). In the haplotype analysis, there were significantly fewer subjects with ht1 in the AIA group than in the ATA group. Based on linear regression analysis, the decline in FEV1 after aspirin challenge in asthmatics homozygous for the rare +82466C>T allele was 2.5 times that in asthmatics with the common allele. In the haplotype analysis, the decline in FEV1 after aspirin provocation was greater in asthmatics without the ht1 haplotype than in those with the haplotype. These results suggest that a rare PPARG+82466C>T allele and haplotype 1 are predisposing factors for aspirin intolerance in asthmatics.
Some eicosanoids activate PPARG; these include 13-hydroxyoctadecadienoic acid,27 15-hydroxyeicosatetraenoic acid (15-HETE), and 15-deoxy-12,14 prostaglandinJ2 (15d-PGJ 2),28 a prostaglandin D2 metabolite. The accumulation of 15-HETE after aspirin-stimulation of peripheral leukocytes from patients with AIA may activate PPARG to modulate airway inflammation.29 As metabolites of the arachidonate pathway, such as 15-HETE and 15d-PGJ 2, regulate transcription and endogenous ligands for the PPARG gene, changes in these mediators in AIA may be responsible for the change in the amount of PPAR-r in the target organ of aspirin hypersensitivity. Therefore, altered synthesis of 15-HETE and 15d-PGJ 2 in AIA may activate PPARG differently from the activation in ATA. In addition, the PPARG agonist rosiglitazone upregulates both the mRNA expression of two lipoxygenase enzymes (platelet-type 12-lipoxygenase and 15-lipoxygenase) and the secretion of their eicosanoid products, 12- and 15-HETE. The rosiglitazone-induced increase in PPARG mRNA expression is blocked entirely by the lipoxygenase (LO) inhibitor baicalein and is restored by the addition of exogenous 12-HETE.30 In the process of lipoxin formation, aspirin acetylation does not totally inhibit the catalysis of COX-2, and this can affect the production of 12-HETE, 15-HETE, and 13-HODE. Previously, we observed that the alleles of the ALOX5 and ALOX5AP promoters cannot be considered prominent risk factors for the development of AIA. However, a genetic variant involving a tandem repeat (GGGCGG; Sp1-binding motif) in the ALOX5 promoter is associated with the severity of airway hyper-responsiveness in AIA patients.31 Therefore, genetic polymorphism of the rare PPARG+82466C>T allele may contribute to the development of aspirin intolerance via a functional change in the gene, such as an altered response to the LO products or altered induction of the two LO enzymes. The molecular mechanism by which the rare PPARG+82466C>T allele, which does not change the encoded protein, modulates the phenotype is even less clear. It is possible that these variants are in linkage disequilibrium with other functional variants, although the PPARG locus has been the focus of intense scrutiny as a candidate for diabetes and related traits, and no such variant has been found.
In summary, we genotyped two SNPs in the PPARG gene, +34C>G (Pro12Ala) and +82466C>T (His449His), and examined the association of each with the development of aspirin intolerance in asthmatics. Association analysis showed that PPARG+82466C>T and PPARG haplotypes were associated with the development of aspirin intolerance. Therefore, the +82466C>T polymorphism in the coding region of the PPARG gene may confer aspirin hypersensitivity via the regulation of gene expression. This information may be useful in the development of new strategies for the diagnosis and control of aspirin intolerance. Further studies are required to define the molecular mechanisms by which common variation at the PPARG locus modulates aspirin hypersensitivity, and to determine whether this suggests treatment strategies in asthmatics with different PPARG genotypes.



 XML Download
XML Download