

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Asthma is a chronic inflammatory disease of the airways, which is characterized by the characteristic symptoms of dyspnea, chest tightness, cough and wheezing, and by variable airflow obstruction and airway hyperresponsiveness to a wide variety of physical and inhaled chemical stimuli. Over the past 40 yr, very effective medications have been developed to treat asthma, the most effective of which are inhaled β2-agonists for acute symptom relief and inhaled corticosteroids (ICS) for long term management.1 Important insights into the optimal management of asthma were made in the early 1980's, when the central role of airway inflammation was identified to be important in asthma pathogenesis, even in very mild disease.2 This resulted in a change of focus from the relief of symptoms with frequent use of inhaled short acting β2-agonists, to the prevention of symptoms and asthma exacerbations by the regular use of ICS. This approach is extremely effective in the majority of asthmatic patients, and in those who remain symptomatic despite ICS treatment, the combination of ICS and a long-acting inhaled β2-agonists (such as formoterol or salmeterol) is generally sufficient to control asthma.3
Asthma treatment guidelines have identified that the primary goal of management is to achieve optimal asthma control.1 Asthma control means the minimization of night time and day-time symptoms, and no activity limitation, rescue bronchodilator use or airway narrowing. The search for new and effective asthma treatments has persisted and the approaches developed to assess these new treatment approaches have changed in light of the appreciation of inflammation as central to asthma pathophysiology and the focus on asthma control as the most important treatment outcome. This review will focus on the value and limitations of allergen inhalation challenge and its associated increase in airway inflammation in the evaluation of new therapeutic options for asthma.
ACTIVITY vs EFFICACY vs EFFECTIVENESS
Drug development is a 4 phase process. Phase I is the evaluation of the new pharmacological entity for safety in normal volunteers; although this phase is sometimes also used to look for some evidence of activity. Phase II is when the "proof of concept" study are done, and in studies for new entities in asthma, this is usually in mildly symptomatic patients with airflow obstruction, or in a clinical model of allergic inflammation. These studies are really examining for activity of the new entity in asthmatic airways and evidence of this activity does not always translate to evidence of efficacy in asthma. Also, these Phase II studies are usually small in size and of short duration, which provides little information of the safety of the entity in asthmatic patients. Phase II is sometimes divided into Phase IIa, where the proof of concept study is done, and Phase IIb, where the entity is evaluated in small studies of more symptomatic patients, to help develop the designs for the efficacy studies. Efficacy is evaluated in Phase III studies, which are designed to meet the requirements of regulatory agencies to show both efficacy and safety in the patient population for whom the new drug is to be prescribed. These studies are large (often >1,000 patients) and long (usually 1 yr of treatment). Evidence of efficacy is required in two such studies to obtain regulatory approval of the new treatment. The requirement for the outcomes to be evaluated in these Phase III studies differs in different countries granting regulatory approval. The final phase of clinical trial development involves Phase IV studies, conducted after drug approval has been obtained. These studies are usually used to best position the drug in the marketplace and to collect additional information on safety. However, very few new drugs for asthma have been formally evaluated for effectiveness, which is the usefulness of the drug in the real world setting.
ALLERGEN INHALATION CHALLENGE
In 1873, Blackley published a monograph describing grass pollen as the cause of these seasonal symptoms of allergic rhinitis and seasonal asthma.4 The late asthmatic response (LAR), which occurs 3 to 8 or more hours after allergen exposure, is now recognized as clinically more important than the early asthmatic response (EAR). In the 1950's, Herxheimer identified that many of patients undergoing allergen hyposensitization complained of late symptoms, and he record the development of allergen-induced LAR in a significant number of patients, more common with house dust than with pollen.5 It is now recognized that inhaled allergens by a sensitized subject results in acute bronchoconstriction, usually beginning within 15-30 min and lasting 1-3 hr. This is called the EAR. This can then be followed by the development of an LAR beginning after the spontaneous resolution of the EAR, but which is more insidious in onset, gradually worsening over 3-12 hr, is more prolonged and often more severe than the EAR (Fig. 1).6 Individuals who develop both an EAR and LAR after inhaled allergen (dual responders) also have more marked and prolonged increases in airway hyperresponsiveness,7,8 and greater increases in allergen-induced airway inflammation, particularly in airway eosinophils3,9 and basophils.10 This clinical model of allergen inhalation challenge has been extremely useful for examining the mechanisms of allergen-induced airway inflammation and the associated physiological changes and for documenting the efficacy of drugs to treat asthma.
It is now known that inhaled allergen induced their airway responses by cross-links antigen-specific immunoglobulin (Ig)E that is bound to IgE receptors (FCεRI) on mast cells resident in the airway and circulating basophils. This is followed by mast cell degranulation to release a variety of preformed mediators (e.g., histamine),11 as well as the up regulation of eicosanoid pathways to produce newly formed mediators (e.g., leukotrienes, prostaglandins) of bronchoconstriction,12 which also lead to increasing vascular permeability. Indeed, allergen-induced bronchoconstriction occurring during the EAR and LAR can be abolished by treatment with a combination of anti-histamine and leukotriene antagonists,13 indicating that histamine and cysteinyl leukotrienes together are responsible for these allergen-induced effects.
PHARMACOLOGICAL MODIFICATION OF ALLERGEN-INDUCED RESPONSES
All of the currently available and effective treatments for asthma modify some aspects of allergen-induced responses. These medications include short-acting and long-acting inhaled β2-agonists (SABAs and LABAs), inhaled corticosteroids (ICS), cromones, methylxanthines, leukotriene inhibitors, and anti-IgE monoclonal antibody.
Inhaled β2-agonists
Treatment with SABAs immediately before allergen inhalation inhibits or reverses the EAR and, if administered during the LAR, can partially reverse the LAR, when it is not too severe; however, they neither prevent the LAR, nor allergen-induced airway inflammation. By contrast, the regular use of SABAs has been demonstrated to enhance most aspects of the allergen-induced airway responses including the EAR,14 the LAR15 and the allergen-induced airway inflammation.16 This evidence provided part of the rationale for avoiding the regular use of SABAs as monotherapy for asthma.
LABAs are difficult to evaluate because of their prolonged bronchodilator, as well as functional antagonist effects. Functional antagonism means their ability to prevent the onset of bronchoconstriction. Initial reports showing inhibition of EAR and LAR and induced AHR were thought to represent more than just the functional antagonist effect.17 However, subsequent studies have generally shown minimal inhibition of the allergen-induced inflammation,18 and it is currently believed that LABAs act mainly as functional antagonists in their inhibition of allergen-induced airway responses.19-25
Methylxanthines
Theophylline has a prolonged effect as a weak bronchodilator and a functional antagonist, which results in at most partial inhibition of the LAR.26-30 A small study demonstrated the partial inhibition of the LAR, but little effect on the induced AHR.30 There are few studies addressing allergen-indcued airway inflammation, however, one study showed no inhibition of allergen-induced airway eosinophilia, but a small reduction in airway activated T cells.31
Inhaled corticosteroids
The most important controller medications for asthma are ICS. They are known to improve all aspects of asthma control,1 reduce eosinophilic airway inflammation32 and reduce some components of airway remodelling.32 ICS also have profound effects on allergen-induced airway responses. When used in single dose shortly before allergen challenge (or in the interval phase between the EAR and the LAR),33 ICS demonstrate no effect on the EAR, but markedly inhibit the LAR.19,34-36 Regular treatment with ICS for several weeks improves the EAR, abolishes the LAR and markedly reduces allergen-induced airway inflammation.37-41
Cromones
The cromones consist of two drugs, cromoglycate and nedocromil. The earliest studies of pharmacoprotection against allergen-induced responses were done with cromoglycate. These studies demonstrated that when used before, but not after, allergen challenge cromoglycate inhibits allergen-induced EAR, LAR, and allergen-induced airway hyperresponsiveness.34,35,42-44 These data were used to support the mechanism of action of the cromones as inhibiting allergen-induced mast cell degranulation. There are no studies addressing the effects of treatment with either cromoglycate or nedocromil on allergen-induced airway inflammation.
Leukotriene inhibitors
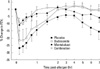
Leukotriene inhibitors inhibit either the production of the cysteinyl leukotrienes (5-lipoxygenase inhibitors) or the action of cysteinly leukotrienes on their receptor (Cys LT1 receptor antagonists). Treatment with leukotriene inhibitors attenuates all aspects of allergen-induced airway responses. They attenuate the EAR,45-50 and do so to a greater extent than do ICS,49 but are less effective than ICS in their ability to attenuate the LAR (Fig. 1), or allergen-induced AHR.49 Leukotriene inhibitors also markedly reduced allergen-induced airway eosinophilia to a similar extent as ICS (Fig. 2).49,50
Various histamine antagonists (H1 blockers) have been examined with the allergen challenge model and have been demonstrated to have small degrees of protection against the EAR, with little effect on the LAR.50-57 Of interest, however, the combination of a leukotriene antagonist and a H1 blocker completely abolishes both the EAR and LAR.13 This means that the bronchoconstriction that develops after allergen inhalation is caused by the release of histamine and the cysteinyl leukotrienes, likely from mast cell activation causing the EAR and basophil activation causing the LAR.10
Anti-IgE monoclonal antibody
Allergen inhalation challenge was used in two of the pivotal early investigations in the study of anti-IgE (omalizumab) in asthma.58,59 Following treatment with anti-IgE, despite administration of approximately twice as much allergen compared to the placebo treatment, subjects had marked reduction in the LAR.59
The evaluation of ineffective therapies for asthma
The consistent demonstration of the benefits of drugs effective for asthma treatment on aspects of allergen-induced airway responses has resulted in allergen inhalation challenge becoming the most common method for the evaluation of new therapies for asthma (particularly if these are thought to have anti-inflammatory properties). Several drugs candidates have failed to modify allergen-induced responses and have also failed in larger clinical trials in asthma. Perhaps the best example of this was the evaluation of esterase-sensitive ICS. These were corticosteroids which were rapidly metabolized by esterases in the blood and therefore had the profile of being active in the airway, but potentially having no corticosteroid side effects. An interesting study was performed with one such molecule, which had been demonstrated not to work in clinical trials in asthma. This clinically ineffective esterase-sensitive ICS was compared with the clinically effective ICS, budesonide, in a single dose trial involving allergen inhalation challenge. This study demonstrated that allergen challenge was able to differentiate between the clinically effective and clinically ineffective corticosteroid with regard to its effect on the allergen-induced LAR.36 There are other examples of candidate drugs failing to protect against allergen challenge and failing in clinical trials. These include platelet activating factor (PAF) antagonists,60,61 thromboxane inhibitors,62,63 VLA4 antagonists,64 and inhaled leukotriene inhibitors.65
The results of these studies suggest that a well conducted and interpreted allergen challenge study can be of value to predict efficacy or lack of efficacy of asthma controller therapies. Thus, drugs which inhibit the asthmatic responses, particularly allergen-induced LAR, allergen-induced increase in AHR and allergen-induced inflammation are generally effective in asthma therapy (Table 1). Perhaps of more value in drug development for asthma is that compounds that have not influenced the allergen-induced late sequelae have never been subsequently proven to be effective in asthma treatment (Table 1). Thus, the test has a moderate positive predictive value, but an excellent negative predictive value.
INVESTIGATION OF NEW AGENTS TO STUDY THE PATHOPHYSIOLOGY OF ALLERGIC RESPONSES
A large number of new molecules targeting various mechanisms or pathways of the airway inflammatory process are under scrutiny and considerable efforts will be devoted to determine if these agents may be clinically useful and improve airway inflammatory conditions such as asthma and rhinitis.66,67 Allergy is a key mechanism leading to both the development and persistence of airway inflammation and structural changes that may result in symptomatic asthma and rhinitis.68 Methods that could rapidly determine if a new product will be useful in treating those conditions are welcome.
With standardized methods and validated outcomes, the allergen bronchoprovocation test has become such tool which may quickly, in a very limited number of patients, provide key information on the therapeutic potential of the tested agent.36 As stated earlier in this manuscript, the test may indicate that the drug will be ineffective to treat asthma, for example, although it does not provide accurate data on the degree of therapeutic efficacy of the agent. Nevertheless, as an initial "screening test", it may avoid spending large amount of money and resources to evaluate its clinical usefulness.
Not only can this method help forecast clinical efficacy of the agent, but it may provide valuable information on how the agent is influencing the pathophysiology of immune responses and airway inflammation. With the new non-invasive methods of assessment of airway inflammation such as induced-sputum analysis, exhaled NO or exhaled breath condensate analysis (e.g. isoprostanes, pH, etc.) various aspects of the inflammatory response may be explored.69,70
Although there are still limitations to these tests, standardization procedures and improved methods of measurement of various mediators are being developed, as well as surrogate markers of airway remodelling processes. The allergen bronchoprovocation test therefore provides a dynamic model to evaluate various clinical, physiological and inflammatory changes following the acute trigger of the inflammatory cascade. The newly developed low dose allergen challenges may as well be useful, in mimicking more closely natural exposures.
CONCLUSIONS
When embarking on the clinical development of therapeutic agents in airway disease, designing effective studies to investigate the airway response requires an understanding of the available outcomes that are clinically relevant, such as asthma exacerbations and asthma control. These should also be considered in association with the appropriate standardized physiological and biochemical markers to validate efficacy, such as markers for inflammation and airway hyperresponsiveness; the hallmarks of dysfunction in airway disease that are likely the targets of a new therapeutic agent. All outcome measures, whether chosen as primary or secondary outcomes, may have certain limitations that need to be understood before they are applied in an effort to maximize their usefulness in establishing efficacy of a therapeutic agent.
The practical and safety considerations of a chosen outcome measure, in particular those that are more invasive, should be well understood and carefully considered. When designing a clinical trial, prior studies that demonstrate the success of known therapies in airway disease should also be considered in an effort to demonstrate equivalent or superior efficacy and safety compared to existing therapies. Finally, and with no less importance, the most appropriate patient population at each stage of development of a therapeutic agent needs to be selected that reflects the broadest applicable patient population that will translate to benefits in the real world population with airway disease.


 XML Download
XML Download