

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The accurate diagnosis of a pelvic mass is a challenge to a gynecologist before the pelvic cavity is explored by laparotomy or laparoscopy, because of pelvic masses' bizarre and atypical behavior. Pelvic masses are one of the most common clinical presentations. These masses represent a number of benign and malignant conditions. Treatment can be optimally planned if it is known beforehand whether an ovarian neoplasm is benign or malignant. The prognosis for women with ovarian cancer may be greatly influenced by appropriate first-line therapy.1~6
Used alone, the diagnostic accuracy of demographic, sonographic and biochemical variables is poor for clinical use. Jacobs et al.7 developed the risk of malignancy index (RMI) for referral of relevant patients to gynecologic oncology centers. The RMI 1 was the first diagnostic model in the assessment of patients with pelvic masses. The RMI was adjusted by Tingulstad et al.8 in 1996 (RMI 2) and again in 1999 (RMI 3).9 The three versions of the RMI have been validated retrospectively and prospectively in different clinical studies7~19 where a cut-off value of 200 showed the best discrimination between benign and malignant pelvic masses, with high sensitivity and specificity levels (sensitivity 51-90%, specificity 51-97%). Recently RMI 4 was introduced by Yamamoto et al.20 Four RMIs had some different characteristics. RMI 1 was the first version as developed by Jacobs et al.7 and gave an ultrasound score (U) of 0 when none of the ultrasound features were present, resulting in an RMI 1 of 0 regardless of the cancer antigen (CA) 125 level. But, RMI 2-4 had not ultrasound score of 0. Yamamoto et al.20 have published their study in which RMI 4 was created, that includes tumor size as an additional parameter.
The main advantage of four RMIs is that it is a simple scoring system that can be applied directly into clinical practice without the introduction of expensive or complicated methods (such as computed tomography scan, magnetic resonance imaging, and whole-body positron emission tomography). The RMIs can be applied in less specialized centers. The RMI 1 was the first diagnostic model that combined demographic, sonographic and biochemical data in the assessment of patients with pelvic masses.
The purpose of the present study was to assess ability of the RMI 1 to discriminate between benign and malignant pelvic masses.
Materials and Methods
This is a retrospective study. The clinical data were obtained from consecutive 547 women with pelvic masses scheduled for laparotomy or laparoscopy at the Department of Obstetrics and Gynecology of a single institution between January 2007 and December 2010. Preoperative serum CA 125 levels, ultrasound findings, and menopausal status were noted. In all cases, ultrasound was performed transvaginally with a 6.0 MHz transducer (Acuvix XQ, Medison, Korea); an abdominal scan was also conducted when indicated.
As proposed by Jacobs et al.7 in 1990, the RMI 1 is defined as the multiplied value of the ultrasound score (U), menopausal status (M) and serum CA 125 level: RMI 1 = U × M × CA 125.
Multilocularity, solid areas, bilaterality, ascites and intraabdominal metastases score one point each. A total of 2 or more points gives U = 3, 1 point gives U = 1, 0 points gives U = 0. Postmenopausal status is defined as more than 1 year of amenorrhea, or age 50 years or older among women who had prior hysterectomies, and scores M = 3; premenopausal status scores M = 1. Serum CA 125 (U/mL) is entered directly into the equation. The ultrasounds were performed by gynecologic oncologists, general gynecologists, or residents.
The histopathologic diagnosis was regarded as a definitive outcome. When a gynecological cancer was found, it was staged according to the International Federation of Gynecology and Obstetrics (FIGO) classification.21
The sensitivity was defined as the percentage of patients with malignant disease having a positive test result. The specificity was defined as the percentage of patients with benign disease having a negative test result. The positive predictive value was defined as the percentage of patients with a positive test result having malignant disease and the negative predictive value was defined as the percentage of patients with a negative test result having benign disease.
Statistical analyses were performed using the Statistical Packages for the Social Sciences Version 14.0.1 (SPSS Inc., Chicago, IL, USA). The χ2-test was used to test differences in distribution of menopausal status, and the ultrasound score. The Mann-Whitney U-test was applied in the cases where the assumptions of the 2-sample t-test do not hold (when testing differences in distribution of CA 125 among women with benign and malignant pelvic masses). A receiver operating characteristic (ROC) curve was created to show the relation between sensitivity and specificity of the CA 125, menopausal status, the ultrasound score, and the RMI 1 in the discrimination between benign and malignant pelvic masses.
Results
A total of 547 patients were included in the study. A number of 434 patients (79.3%) were diagnosed with benign conditions, whereas 113 patients (20.7%) had malignant disease (Table 1). The malignancies included serous cystadenocarcinoma (n = 35), mucinous cystadenocarcinoma (n = 13), endometrioid adenocarcinoma (n = 6), clear cell carcinoma (n = 6), transitional cell carcinoma (n = 7), granulosa cell tumor (n = 6), Yolk sac tumor (n = 2), dysgerminoma (n = 2), immature teratoma (n = 1), Sertoli-Leidig cell tumor (n = 1), malignant mixed mullerian tumor (n = 2), mullerian adenosarcoma (n = 1), Krukenberg's tumor (n = 2), and borderline malignancy (n = 29). The benign gynecological conditions included mature cystic teratoma (n = 184), mucinous cystadenoma (n = 85), serous cystadenoma (n = 93), endometriosis (n = 27), fibroma (n = 12), fibrothecoma (n = 5), tubo-ovarian abscess (n = 5), paratubal cyst (n = 6), functional follicle (n = 6), struma ovarii (n = 3), actinomycosis (n = 2), Brenner tumor (n = 2), sclerosing stromal tumor (n = 1), and leiomyoma (n = 1).
The distribution of benign and malignant cases by menopausal status, the ultrasound score, and CA 125 is described in Table 2. In univariate analysis, a significant linear trend for malignancy was found by postmenopausal state, increasing ultrasound score, and increasing CA 125, respectively. The mean serum level of CA 125 was significantly higher among women with malignancies when compared with women with benign lesions (507 U/mL vs 35 U/mL). The sensitivity, specificity, and positive and negative predictive values of different levels of serum CA 125, the ultrasound score, and menopausal status are reported in Table 3. The best performance was obtained for a serum CA 125 level of 40 U/mL. At a serum level of CA 125 40 U/mL, the sensitivity of detecting malignancy was 73.4% and the specificity was 83.1%, positive and negative predictive values were 53.2% and 92.3%, respectively. The sensitivity, specificity, and positive and negative predictive values of the ultrasound score of 2 were 94.7, 62.2, 39.5, and 97.8%, respectively. When individual parameters were compared, CA 125 performed better than the ultrasound score and menopausal status, even though the ultrasound score of 2 had more sensitivity than CA 125, but with considerable loss of specificity.
The performance of RMI 1 at different cut-off values is shown in Table 3. The overall best performance in the index was obtained at a cut-off level of 150. RMI 1 at a cut-off of 150 with a sensitivity of 77.9%, specificity of 81.1%, and positive predictive value of 51.7% and negative predictive value of 93.4% had the highest performance in determining malignant tendency of a pelvic mass.
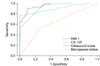
The diagnostic performance of the ultrasound score, CA 125, and menopausal status with the RMI 1 were shown in ROC curves (Fig. 1). ROC analysis of the RMI 1, CA 125 serum levels, the ultrasound score, and menopausal status showed that the values of area under the curve had values of 0.795, 0.782, 0.784, and 0.594, respectively. The RMI 1 had the largest area under the ROC curve when compared with CA 125, the ultrasound score, and menopausal status. The ROC curve evaluation of CA 125, the ultrasound score, and the RMI 1 were all found to be relevant predictors of malignancy. The RMI 1 was found to be statistically significant to the menopausal status (P = 0.001), while were not statistically significant to CA 125 (P = 0.628) and the ultrasound score (P = 0.541).
Discussion
This study was designed to identify the ability of the RMI to correctly identify benign and malignant pelvic masses. The RMI was originally developed by Jacobs et al.7 and subsequently the same group reproduced the results in a new group of patients, establishing the superiority of RMI 1 over the individual parameter.10
The most useful individual criteria in discriminating benign gynecologic lesions from malignant ovarian tumors in the present study were serum CA 125 40 U/mL with a sensitivity of 73.4% and specificity of 83.1%, and an ultrasound score of 2 with a sensitivity of 94.7% and specificity of 62.2%. These results are similar to those of a previous study by Jacobs et al.7 in 1990, which calculated a sensitivity and specificity of 71% and 75% for CA 125 and sensitivity and specificity of 71% and 83% for an ultrasound score of 2. In the present study menopausal status performed less well than the RMI 1, while CA 125 and the ultrasound score had similar performances. The RMI 1 was a useful preoperative method in the classification of women with pelvic masses into low and high risk for malignancy. The high sensitivity, specificity, positive predictive value and negative predictive value of 82.1%, 78.1%, 40.6% and 96.0%, respectively found in the present study at a cut-off of 150 is similar to other studies that found that the RMI was a better diagnostic marker in diagnosing ovarian cancer.10,17
The previous studies indicate that a RMI 1 of 200 gives the most optimal cut-off, while some authors have suggested a different cut-off value.7,11 Using an RMI 1 cut-off of 150, Torres et al.15 showed a sensitivity and specificity of 79%, and Ulusoy et al.19 showed a sensitivity, specificity, positive and negative predictive value of 76.4%, 77.9%, 65.9% and 85.5%, respectively, with a 79.4% correct diagnosis rate. This study showed that a RMI 1 of 150 yields the optimal cut-off value. There are probable reasons to describe the different cut-off values: First, the malignancy prevalence is different. It is well known that, for any test, the positive predictive value will be lower and the negative predictive value higher when used in populations where the disease is uncommon. In our study population, 20.7% of the patients were diagnosed with malignancies while Manjunath et al.13 reported 61.2% of malignant disease. Second, the lower cut-off value, obtained in our study may be associated with the higher number of malignant cases in the premenopausal group - 56.6% in our study versus 19%7 and 20%.8 Third, the diagnostic accuracy of a serum CA 125 assay is expected to be lower in premenopausal patients. CA 125 levels fluctuate during the menstrual cycle, being the highest during menstruation. Also, diseases such as endometriosis and pelvic inflammatory disease are more frequent in premenopause. These diseases are known to cause elevated CA 125 values.22
Borderline malignancies tend to have lower RMI 1-values compared to invasive malignancies and are therefore less detectable. This can be explained by the different features they exhibit, and therefore they have low scores both on ultrasound and CA 125 levels.23 One must keep in mind that the primary goal for developing the RMI 1 is the referral of patients with malignant diseases to gynecologic oncologists. Considering the biological nature and behavior of borderline ovarian tumors, in these patients, one can discuss the relevance of primary surgical treatment and staging at the subspecialized department. Further research is needed to evaluate methods able to identify these patients better than in the present and similar studies. A detailed evaluation of the present material is necessary and specifically needed to eventually improve preoperative scoring. Recently Alanbay et al.24 reported that compared to ultrasound, menopausal status, CA 125, CA 19-9, the RMI 4 was fond to be the best predictive method for differentiation of borderline ovary tumor from benign adnexal masses.
Vaginal ultrasound and new scoring system represent the good diagnostic tool for the detection malignant ovary masses. Parameters of new scoring system were wall thickness, number of septum, volume of mass, irregularity, vascularity and echogenicity. The new scoring system had sensitivity 73.9%, specificity 97.7% and negative and positive predictive values of 96.6% and 80.9% respectively. Sensitivity of new scoring system was similar to previous ones but specificity of that is higher. New scoring system shows better to differentiate benign from malignant ovarian mass than four other scoring systems.25
We have chosen to use the first version RMI 1 as developed by Jacobs et al.7 Some limitation for this include Jacobs et al. allocating an ultrasound score of 0 when none of the ultrasound features were present, resulting in an RMI 1 of 0 regardless of the CA 125 level. In our study, no patient had malignant tumor in ultrasound score of 0.
The major finding of this study, accepting the RMI 1 cut-off value as 150, is statistically significant diagnostic criteria than menopausal status that discriminate between benign and malignant pelvic masses.



 XML Download
XML Download