

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Breast cancer is a top ranking cancer in women and is a leading cause of morbidity and mortality. In most of the western countries, the incidence of breast cancer has been reported to increase with age and the highest age group is usually comprises of women in their postmenopausal period. However, the situation in South Korea is surprisingly different. The breast cancer is rapidly increasing in Korean women and especially in premenopausal women. The occurrence of breast cancer is highest in the women who are in their 40s followed by women who are in their 50s, 30s, and 60s. In other words, high mammography (MMG) density is considered as a strong, independent risk factor for breast cancer in postmenopausal women. Breast constitutional density may be altered and increased, so called acquired density, by exogenous causes such as hormone therapy (HT). The high MMG density before starting HT is also considered as a risk factor for breast cancer. However, the increased MMG density caused by the use of HT is not considered as a risk factor for breast cancer. In terms of postmenopausal HT, it is recently known that not estrogen but progesterone increases the risk of breast cancer. Estrogen-only HT without progesterone has been reported to decrease the risk of breast cancer. Based on these findings, the use of progesterone releasing intrauterine system (IUS) is contraindicated in women with a history of breast cancer. The levonorgestrel (LNG) releasing IUS (Mirena®) releases progesterone, and levonorgestrel at levels of 20 µg/day and the approved indications are contraception, menorrhagia, dysmenorrhea, and endometrial protection during estrogen replacement therapy. The use of LNG-IUS is increasing in Korea. The LNG-IUS is mostly applied to women, who are in their 30s and 40s and the women of these age groups show the highest incidence of breast cancer in South Korea. Therefore we, Korean gynecologic doctors, are concerned about the effect of progesterone releasing-IUS on breast cancer risk in these aged women, who are also referred to as the highest breast cancer incidence aged group. Therefore, the safety aspect of LNG-IUS in breast cancer among premenopausal women is an imperative issue in Korea. However, until date, there is no published data on this issue worldwide. Therefore, our aim is to evaluate the effect of LNG-IUS on the Korean premenopausal women. If we are convinced about the safety of LNG-IUS on the highest breast cancer occurrence age group in Korean women, we, gynecologist can confidentially apply the LNG-IUS.
Materials and Methods
1. Study population
We retrospectively reviewed medical records of 639 premenopausal women, who underwent LNG-IUS insertion in our gynecology department from 2000-2011. Among these women, a total of 46 premenopausal women aged over 35 years, and who underwent MMG and breast US check-up in our radiology department before and after the insertion of LNG-IUS from January 2005 to December 2011 were finally included in this study. We limited the study period as after 2005 for the precise interpretation regardless of the status of X-ray film because our hospital established picture archiving and communication system (PACS) system in 2005. One radiologist with specialization in breast imaging reviewed the PACS images to avoid the bias of inter-radiologist variation and for reducing the effect of changing the criteria of MMG or US interpretation. Women, who had some disease of the breast and personal and family history of breast cancer, were excluded from this study. Women, who were taking certain medications, such as oral contraceptives and other hormonal agents, were not included in this study as there was risk of effect on breast imaging. The review board of committee in our hospital approved this study (ECT 12-07B-22).
2. Methods
We compared the findings of MMG and breast ultrasonography (USG) both before and after the insertion of LNG-IUS. The assessment of breast density in MMG was done based on Breast Imaging Reporting and Data System (BI-RADS) density classification. Basically, this classification is categorized with 4-point scale (fatty, scattered fibroglandular densities, heterogeneously dense, and extremely dense). The pathologic result of any case in which breast biopsy was performed was also reviewed.
3. Equipments
The machines used for MMG were computed radiography (CR) of Senograph DMR + (GE Medical Systems, Milwaukee, WI) and full field digital MMG (FFDM) of Senograph DS (GE Medical System, Milwaukee, WI). The US was performed using iU-22 (Philips Medical Systems, Bothell, WA, USA) and HDI 5000 (ATL, Bothell, WA). This study was approved by the Institutional Review Board Committee of our medical institute (ECT12-07B-22). Data obtained from each individual patient were expressed as the mean ± SD (standard deviation) and the changes in mammographic density and findings of MMG and breast USG, before and after insertion of LNG-IUS were analyzed using Cochran-Armitage trend test. The statistical significance was set at P < 0.05.
Results
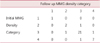
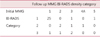
The mean age of the participants was 42.3 ± 4.9 years. The mean gravida and parity were 2.54 (0-5) times, and 1.26 (0-3) times, respectively. The mean height, weight and body mass index were 159.5 ± 5.1 cm, 60.6 ± 9.6 kg, and 24.2 ± 3.6 kg/m2, respectively. The main indication for LNG-IUS insertion was uterine myoma/adenomyosis accompanying anemia in 26 women (38.4%). Twelve women (26.0%) underwent LNG-IUS insertion for contraception and in the remaining 8 women (17.3%) we could not find the exact reason for LNG-IUS insertion by retrospective review. The mean interval for MMG follow up and breast US was 25.5 ± 10.8 months and 25.2 ± 11.5 months, respectively. We tested the accordance of MMG density between initial and follow up MMG category. The initial MMG density results correlated well with those of follow up test (P < 0.001) (Table 1). In terms of MMG category, the initial MMG categories correlated well with those of follow up MMG category (P < 0.001) (Table 2). The breast US categories also correlated well with those of follow up test (P < 0.001) (Table 3). There was no case of breast cancer among women who were supposed to undergo breast biopsy because of abnormal findings in MMG and USG.
Discussion
The present study was designed to investigate the effect of LNG-IUS on the breast imaging study results, including the MMG density, MMG category and breast US category in Korean women, who were in the highest breast cancer incidence aged group. The main findings of this study were that the LNG-IUS does not cause any changes in the MMG density nor the BI-RADS MMG category and the breast US in healthy premenopausal women. Approximately, 12 million women worldwide use the LNG-IUS and it was launched in South Korea over a decade ago, and has become one of the most popular forms of long-acting contraception. LNG-IUS has a high contraceptive efficacy with the primary mode of action based on local progestogenic effects. Compared to other LNG-only methods (implants, progestin-only pills), the serum level in LNG-IUS users are low.1 However the potential breast cancer risk of progestin-only contraceptives has been discussed occasionally,2~5 and gynecologist have raised concern about the safety of LNG-IUS in women with breast cancer. LNG-IUS is well known for its low systemic hormone exposure; however, a potential tumor-promoting or tumor-inducing effect by LNG-IUS cannot be excluded. Previous studies reported no increased breast cancer risk in LNG-IUS users. A retrospective analysis of 23,885 women did not show an increased risk of breast cancer. This previously reported study involved Finnish women, who were regularly using LNG-IUS for contraception with an average age of 35.4 years at the time of insertion. The authors were also convinced about the safety of LNG-IUS without any risk of development of breast cancer.6 In terms of Norplant use, in a review by Sivin,5 the author noted that malignancy rates in the Norplant Post-marketing Surveillance Study were low and were as expected for women of reproductive age. Curtis7 reported that to date, no studies had found evidence for increase in rates of cancer with the use of LNG implants. It has been suggested that the breast cancer risk with the LNG-IUS is lower than that with LNG implants, which is due to lower serum LNG levels and reduced systemic exposure.6 Dinger et al.8 concluded that the LNG-IUS is not associated with a higher risk of breast cancer in "ever users" or "current users" in an analysis of 5,113 breast cancer cases and 20,452 controls. The limitation of our study was the relatively small size of the study population and retrospective nature of the study. We did not adjust the interval period from the insertion of LNG-IUS and the follow up of MMG and breast US. We could not use the continuous MMG density calculation system (e. g., Percent Mammographic Density, PMD) because the equipment was not available in our hospital. However, to the best of our knowledge, this study is the first of its type to investigate the effect of LNG-IUS on the MMG and breast US, which is the most powerful strength of our study. The most meaningful one, especially for the Korean gynecologic doctors is the mean age of this study which was 42.3 years (the age group which demonstrate the highest breast cancer incidence in Korean women). We also included women, who underwent MMG and breast US only after establishment of PACS system in our hospital for the avoidance of interpretation bias caused by the difference in the status of X-ray film. One radiologist with specialization in breast imaging reviewed the PACS images to avoid the bias of inter-radiologist variation and to reduce the effect of change in the criteria of MMG or US interpretation. These results indicate that the use of LNG-IUS in healthy premenopausal women might not be related with increased risk factor (mammographic density) for breast cancer. Dense breast on MMG and benign looking mass lesion on breast US are not relative contraindications for the use of LNG-IUS in otherwise healthy premenopausal women. In summary, we demonstrated that the use of LNG-IUS doesn't cause any changes in MMG density, findings of MMG, and findings of breast US in healthy premenopausal Korean women.

 XML Download
XML Download