

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Objectives
To investigate bone responses to hormone therapy (HT) according to basal bone mineral density (BMD) and previous responses to HT, as well as the frequency and clinical characteristics of HT non-responders in Korean postmenopausal women.
Methods
We retrospectively reviewed a total of 1,836 postmenopausal women who received HT from seven university hospitals. BMD data at the lumbar spine (LS), femur neck (FN), femur trochanter (FT) and total hip (TH) before HT, and at one, two, and three years after HT were collected. All patients were divided into three groups according to basal BMD: normal, osteopenia, and osteoporosis.
Results
Women with a greater loss of BMD during the first year of HT were more likely to gain BMD in the second year at any of the four skeletal sites. Bone responses to HT during the third year were not related to the responses during the first year. Mean BMD changes during the first year were significantly higher in the osteoporosis group, but mean BMD changes during the second year were not different between three groups except in LS. The frequency of non-responder (annual BMD losses more than 3%) during the first year was significantly higher in the normal basal BMD group. Mean basal BMDs were higher in the two-year consecutive non-responder group at LS, FN and FT, but those of the three-year consecutive non-responder group were not significantly higher except in FN.
Figures and Tables
Table 1
Mean percentage change of bone mineral density (BMD) in the lumbar spine during year 1 compared with the mean percentage change of BMD in the lumbar spine during the second and third year of hormone therapy
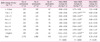
Table 2
Mean percentage change of bone mineral density and the proportion of non-responders at 1, 2 and 3 years after hormone therapy according to the basal status of bone mass of the lumbar spine
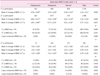
Table 3
Mean percentage change of bone mineral density and the proportion of non-responders at 1, 2, and 3 years after hormone therapy according to the basal status of bone mass in the lumbar spine, femur neck, and femur trochanter

Table 4
Comparison of clinical characteristics, hormone therapy type and basal status of bone mineral density between 2-year consecutive hormone therapy non-responders and others in lumbar spine, femur neck, and femur trochanter


References
1. NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy Osteoporosis prevention, diagnosis, and therapy. JAMA. 2001. 285:785–795.
2. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA. 2002. 288:321–333.
3. The Writing Group for the PEPI. Effects of hormone therapy on bone mineral density: results from the postmenopausal estrogen/progestin interventions (PEPI) trial. JAMA. 1996. 276:1389–1396.
4. Cauley JA, Robbins J, Chen Z, Cummings SR, Jackson RD, LaCroix AZ, et al. Effects of estrogen plus progestin on risk of fracture and bone mineral density: the Women's Health Initiative randomized trial. JAMA. 2003. 290:1729–1738.
5. Torgerson DJ, Bell-Syer SE. Hormone replacement therapy and prevention of nonvertebral fractures: a meta-analysis of randomized trials. JAMA. 2001. 285:2891–2897.
6. Sturdee DW, Pines A, Archer DF, Baber RJ, Barlow D, Birkhauser MH, et al. Updated IMS recommendations on postmenopausal hormone therapy and preventive strategies for midlife health. Climacteric. 2011. 14:302–320.
7. Hassager C, Jensen SB, Christiansen C. Non-responders to hormone replacement therapy for the prevention of postmenopausal bone loss: do they exist? Osteoporos Int. 1994. 4:36–41.
8. Stevenson JC, Hillard TC, Lees B, Whitcroft SI, Ellerington MC, Whitehead MI. Postmenopausal bone loss: does HRT always work? Int J Fertil Menopausal Stud. 1993. 38:Suppl 2. 88–91.
9. Rozenberg S, Gevers R, Peretz A, Vandromme J, Robyn C, Ham H. Decrease of bone mineral density during estrogen substitution therapy. Maturitas. 1993. 17:205–210.
10. Greendale GA, Wells B, Marcus R, Barrett-Connor E. How many women lose bone mineral density while taking hormone replacement therapy? Results from the Postmenopausal Estrogen/Progestin Interventions Trial. Arch Intern Med. 2000. 160:3065–3071.
11. Kim JG, Kim KR, Gee BC, Kim SH, Choi YM, Moon SY, et al. The bone response to hormone replacement therapy according to basal bone mineral density in postmenopausal women. Korean J Obstet Gynecol. 2001. 44:1450–1454.
12. Crandall C. The role of serial bone mineral density testing for osteoporosis. J Womens Health Gend Based Med. 2001. 10:887–895.
13. Kanis JA. Calcium requirements for optimal skeletal health in women. Calcif Tissue Int. 1991. 49:Suppl. S33–S41.
14. Gardner MJ, Heady JA. Some effects of within-person variability in epidemiologic studies. J Chronic Dis. 1973. 26:781–795.
15. Yudkin PL, Stratton IM. How to deal with regression to the mean in intervention studies. Lancet. 1996. 347:241–243.
16. Cummings SR, Palermo L, Browner W, Marcus R, Wallace R, Pearson J, et al. Fracture Intervention Trial Research Group. Monitoring osteoporosis therapy with bone densitometry: misleading changes and regression to the mean. JAMA. 2000. 283:1318–1321.
17. Chun SW, Kim H, Ku SY, Suh CS, Kim SH, Choi YM, et al. The bone response to second year hormone therapy according to the basal bone mineral density and the bone response to first year hormone therapy in Korean postmenopausal women. J Korean Soc Osteoporos. 2009. 7:168–178.
18. Christiansen C, Mazess RB, Transbol I, Jensen GF. Factors in response to treatment of early postmenopausal bone loss. Calcif Tissue Int. 1981. 33:575–581.
19. Kim DY. Clinical application of bone mineral density measurement. Korean J Nucl Med. 2004. 38:275–281.
20. Bonnick SL, Johnston CC Jr, Kleerekoper M, Lindsay R, Miller P, Sherwood L, et al. Importance of precision in bone density measurements. J Clin Densitom. 2001. 4:105–110.
21. American Medical Association. Part 1: Detection and clinical issues in testing. Managing osteoporosis. 1999. Chicago, IL: American Medical Association.
 XML Download
XML Download